You might also like
- Vagina TrichomoniasisDocument46 pagesVagina Trichomoniasissachikoroseate75% (4)
- Vagina TrichomoniasisDocument46 pagesVagina Trichomoniasissachikoroseate75% (4)
- Vulvovaginal InfectionDocument37 pagesVulvovaginal Infectionmadmax500No ratings yet
- Syndromic Management of Sexually Transmitted InfectionsDocument76 pagesSyndromic Management of Sexually Transmitted Infectionsnamita100% (2)
- 1 Gynecologic Infections 2Document109 pages1 Gynecologic Infections 2Girum SolomonNo ratings yet
- Approach To Vaginal Discharge: DR Faisal Al Hadad Consultant of Family Medicine & Occupational Health PSMMCDocument16 pagesApproach To Vaginal Discharge: DR Faisal Al Hadad Consultant of Family Medicine & Occupational Health PSMMCSupekshya ShresthaNo ratings yet
- Vulvovaginal Infections GuideDocument44 pagesVulvovaginal Infections GuideTeguh Imana NugrahaNo ratings yet
- Infections of Female Genital TractDocument67 pagesInfections of Female Genital TractSana AftabNo ratings yet
- Vaginal Infection 160505210023Document41 pagesVaginal Infection 160505210023Supekshya ShresthaNo ratings yet
- 54.vaginal DischargeDocument40 pages54.vaginal DischargebenNo ratings yet
- 51 Vaginal Discharge & PIDDocument45 pages51 Vaginal Discharge & PIDcollinsmagNo ratings yet
- Vaginal Discharge + PruritisDocument56 pagesVaginal Discharge + PruritisEkoApriandhiNo ratings yet
- Gynecologic Nursing GuideDocument252 pagesGynecologic Nursing GuideQueenete Vallestero CastromeroNo ratings yet
- Chapter 102 Vulvovaginitis: PhysiologyDocument5 pagesChapter 102 Vulvovaginitis: PhysiologyMark LopezNo ratings yet
- Diseases of Vagina, Vulva & Cervix: Natural Defences & Common InfectionsDocument96 pagesDiseases of Vagina, Vulva & Cervix: Natural Defences & Common InfectionsMukesh Thakur100% (1)
- VaginitisDocument14 pagesVaginitisaisa baladjiNo ratings yet
- Vaginal DischargeDocument41 pagesVaginal DischargeIlham Isnin Dolyanov HasibuanNo ratings yet
- Lower Genital Tract Infections & Sexually Transmitted DiseasesDocument38 pagesLower Genital Tract Infections & Sexually Transmitted Diseasesraed faisalNo ratings yet
- Gyn Revalida Review CSL 2 2017Document101 pagesGyn Revalida Review CSL 2 2017Mara Medina - BorleoNo ratings yet
- Gynaecology: Gum, Fertility, Contraception, and UrogynaecologyDocument46 pagesGynaecology: Gum, Fertility, Contraception, and UrogynaecologyOccamsRazorNo ratings yet
- Vaginal Discharge and Vulvar Disease FinalDocument61 pagesVaginal Discharge and Vulvar Disease FinalrohitNo ratings yet
- Obstetrics Vaginitis PresentationDocument4 pagesObstetrics Vaginitis PresentationBlue TechNo ratings yet
- Vaginitis BartolinitisDocument28 pagesVaginitis Bartolinitisfani kurniaNo ratings yet
- Vaginal Discharge Causes and TreatmentDocument47 pagesVaginal Discharge Causes and TreatmentGladstone AsadNo ratings yet
- Genital Tract InfectionDocument96 pagesGenital Tract InfectiondhitaapriliaNo ratings yet
- Vaginal Disorders & Non-Hormonal ContraceptivesDocument31 pagesVaginal Disorders & Non-Hormonal ContraceptivesDr mohamed RashwanNo ratings yet
- Genital Infections: Assoc Prof Suna KABİL KUCURDocument41 pagesGenital Infections: Assoc Prof Suna KABİL KUCURasdNo ratings yet
- Lower Female Genital Tract InfectionsDocument42 pagesLower Female Genital Tract InfectionsAwal Sher khanNo ratings yet
- Genital Candidal InfectionDocument2 pagesGenital Candidal InfectionMalueth AnguiNo ratings yet
- Definition-: Pelvic Inflammatory Disease (PID) Is A Sexually Transmitted Inflammatory Condition of TheDocument7 pagesDefinition-: Pelvic Inflammatory Disease (PID) Is A Sexually Transmitted Inflammatory Condition of TheanweshaNo ratings yet
- VaginitisDocument4 pagesVaginitisBinita ShakyaNo ratings yet
- Sexually Transmitted DiseaseDocument3 pagesSexually Transmitted DiseaseBrianna ValerioNo ratings yet
- Abdominal Pain in Gynecology Non PregnantDocument34 pagesAbdominal Pain in Gynecology Non PregnantRyantino IrdanNo ratings yet
- Activity 18 Fungal InfectionsDocument41 pagesActivity 18 Fungal InfectionsLorena Sobrepeña ApiladoNo ratings yet
- Visual Inspection With Acetic Acid (Via)Document38 pagesVisual Inspection With Acetic Acid (Via)Princess Jeanne Roque GairanodNo ratings yet
- Vaginal Discharge Causes and TreatmentsDocument14 pagesVaginal Discharge Causes and TreatmentsMsharaniaNo ratings yet
- Inflammatory DiseasesDocument83 pagesInflammatory DiseasesIfabiyi OlaniyiNo ratings yet
- Vulvovaginitis: by James Holencik, DODocument70 pagesVulvovaginitis: by James Holencik, DOSyarifa YuliaNo ratings yet
- Urinary Tract Infections in Pregnancy: Jeffrey Pradeep RajDocument29 pagesUrinary Tract Infections in Pregnancy: Jeffrey Pradeep RajjeffreyprajNo ratings yet
- Report On Sexually Transmitted Diseases & PregnancyDocument4 pagesReport On Sexually Transmitted Diseases & PregnancyAdnan Akram, MD (Latvia)No ratings yet
- Genital Tract Infections Guide: TV, VVC, BV, CervicitisDocument70 pagesGenital Tract Infections Guide: TV, VVC, BV, CervicitisAygulNo ratings yet
- Pelvic Inflammatory Disease and Vaginal DischargeDocument50 pagesPelvic Inflammatory Disease and Vaginal DischargeAbdulrahman NajiNo ratings yet
- How STDs SpreadDocument55 pagesHow STDs Spreadjoshy221196No ratings yet
- Slide 1 STIDocument50 pagesSlide 1 STIMatth N. ErejerNo ratings yet
- Nursing Care in Clients With General Disturbance inDocument48 pagesNursing Care in Clients With General Disturbance inJADE MAIKHA A. MIERGASNo ratings yet
- Vaginal DischargeDocument15 pagesVaginal DischargeSyafiq Aiman NaqsyaNo ratings yet
- Bacterial VaginosisDocument20 pagesBacterial VaginosisTum M. TansakulNo ratings yet
- Sexually Transmitted Infections and PregnancyDocument19 pagesSexually Transmitted Infections and PregnancyBeyins TiuNo ratings yet
- Gynecologic Infections GuideDocument91 pagesGynecologic Infections GuideDegefaw BikoyNo ratings yet
- Emergency Obstetrics1Document74 pagesEmergency Obstetrics1Alphine DalgoNo ratings yet
- Bacterial VaginosisDocument2 pagesBacterial VaginosisMalueth AnguiNo ratings yet
- Vaginitis and PID: Wanda Ronner, M.DDocument16 pagesVaginitis and PID: Wanda Ronner, M.DFauzul Nurul AzmiNo ratings yet
- Managing Pelvic Inflammatory DiseaseDocument9 pagesManaging Pelvic Inflammatory DiseaseanweshaNo ratings yet
- Vaginitis and Vaginal DischargeDocument52 pagesVaginitis and Vaginal Dischargedrdoaabakhet148No ratings yet
- Vaginitis EmedicineDocument17 pagesVaginitis EmedicineIndah HaneNo ratings yet
- Dhatchi and Dhinakar PPT FinalDocument46 pagesDhatchi and Dhinakar PPT Final051 DhinakarNo ratings yet
- Pelvic Inflammatory DiseaseDocument3 pagesPelvic Inflammatory DiseaseBigabwa Bernard100% (1)
- Duh Tubuh Wanita, DR SAYU.,SpKK, WMDocument62 pagesDuh Tubuh Wanita, DR SAYU.,SpKK, WMdickypranataNo ratings yet
- Vu Lvo VaginitisDocument3 pagesVu Lvo VaginitisSirly EkaNo ratings yet
- A Simple Guide to Sexually Transmitted DiseasesFrom EverandA Simple Guide to Sexually Transmitted DiseasesRating: 5 out of 5 stars5/5 (9)
- Ureaplasma Infection, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandUreaplasma Infection, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
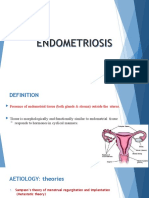
- Endometritis: R.N. Zainab Neamat JumaahDocument19 pagesEndometritis: R.N. Zainab Neamat JumaahSupekshya ShresthaNo ratings yet
- How To Handle Conflict at The Workplace?Document39 pagesHow To Handle Conflict at The Workplace?Supekshya ShresthaNo ratings yet
- Conflict Management: PT-MBA, 1st Year, 2nd Trimester, Group & Organization Dynamics Project, 30th Nov, 2012Document10 pagesConflict Management: PT-MBA, 1st Year, 2nd Trimester, Group & Organization Dynamics Project, 30th Nov, 2012Supekshya ShresthaNo ratings yet
- Organizational Behavior: Presentation On Conflicts By: Shilpi Panchal Mba Ii Semester Oriental College of ManagementDocument23 pagesOrganizational Behavior: Presentation On Conflicts By: Shilpi Panchal Mba Ii Semester Oriental College of ManagementSupekshya ShresthaNo ratings yet
- Resolving Conflict Through Effective CommunicationDocument30 pagesResolving Conflict Through Effective CommunicationSupekshya ShresthaNo ratings yet
- Czzlneulswgbn3st0ysw Signature Poli 180218062304Document39 pagesCzzlneulswgbn3st0ysw Signature Poli 180218062304Supekshya ShresthaNo ratings yet
- Lower Genital Tract Infection: Prepared By: Nibal Shawabkeh Supervised By: Dr. Saada JaberDocument63 pagesLower Genital Tract Infection: Prepared By: Nibal Shawabkeh Supervised By: Dr. Saada JaberSupekshya ShresthaNo ratings yet
- Salpingitis and Related DiseasesDocument20 pagesSalpingitis and Related DiseasesSupekshya ShresthaNo ratings yet
- How To Handle Conflict at The Workplace?Document39 pagesHow To Handle Conflict at The Workplace?Supekshya ShresthaNo ratings yet
- Czzlneulswgbn3st0ysw Signature Poli 180218062304Document39 pagesCzzlneulswgbn3st0ysw Signature Poli 180218062304Supekshya ShresthaNo ratings yet
- Endometritis: Causes, Symptoms, TypesDocument10 pagesEndometritis: Causes, Symptoms, TypesSupekshya ShresthaNo ratings yet
- Romany Lofty: Prepare byDocument27 pagesRomany Lofty: Prepare bySupekshya ShresthaNo ratings yet
- Romany Lofty: Prepare byDocument27 pagesRomany Lofty: Prepare bySupekshya ShresthaNo ratings yet
- Romany Lofty: Prepare byDocument27 pagesRomany Lofty: Prepare bySupekshya ShresthaNo ratings yet
- GyaneDocument188 pagesGyaneSupekshya ShresthaNo ratings yet
- Lower Genital Tract Infection: Prepared By: Nibal Shawabkeh Supervised By: Dr. Saada JaberDocument63 pagesLower Genital Tract Infection: Prepared By: Nibal Shawabkeh Supervised By: Dr. Saada JaberSupekshya ShresthaNo ratings yet
- Romany Lofty: Prepare byDocument27 pagesRomany Lofty: Prepare bySupekshya ShresthaNo ratings yet
- Approach To Vaginal Discharge: DR Faisal Al Hadad Consultant of Family Medicine & Occupational Health PSMMCDocument16 pagesApproach To Vaginal Discharge: DR Faisal Al Hadad Consultant of Family Medicine & Occupational Health PSMMCSupekshya ShresthaNo ratings yet
- Romany Lofty: Prepare byDocument27 pagesRomany Lofty: Prepare bySupekshya ShresthaNo ratings yet
- Vaginitis: - Trichomoniasis - Vulvovaginal Candidiasis (VVC) - Bacterial Vaginosis (BV)Document94 pagesVaginitis: - Trichomoniasis - Vulvovaginal Candidiasis (VVC) - Bacterial Vaginosis (BV)AileenNo ratings yet
- Vaginitis: - Trichomoniasis - Vulvovaginal Candidiasis (VVC) - Bacterial Vaginosis (BV)Document94 pagesVaginitis: - Trichomoniasis - Vulvovaginal Candidiasis (VVC) - Bacterial Vaginosis (BV)AileenNo ratings yet
- Romany Lofty: Prepare byDocument27 pagesRomany Lofty: Prepare bySupekshya ShresthaNo ratings yet
- Lower Genital Tract Infection: Prepared By: Nibal Shawabkeh Supervised By: Dr. Saada JaberDocument63 pagesLower Genital Tract Infection: Prepared By: Nibal Shawabkeh Supervised By: Dr. Saada JaberSupekshya ShresthaNo ratings yet
- REVALIDADocument53 pagesREVALIDAMercy Anne EcatNo ratings yet
- June 2009Document37 pagesJune 2009Onichan KhunNo ratings yet
- Sexually Transmitted DiseasesDocument9 pagesSexually Transmitted DiseasespromiseNo ratings yet
- Local Media7658080159199604674Document31 pagesLocal Media7658080159199604674Ma.Sharja BeloyNo ratings yet
- Causes and management of common vaginal dischargesDocument8 pagesCauses and management of common vaginal dischargesMELVYN HAROLD CHAVEZ MAURICIONo ratings yet
- VaginitisDocument20 pagesVaginitisgpicaulyNo ratings yet
- 1 s2.0 S0223523417309327 MainDocument12 pages1 s2.0 S0223523417309327 MainDan NechitaNo ratings yet
- Pregnancy Signs and SymptomsDocument6 pagesPregnancy Signs and Symptomstio_bsNo ratings yet
- Vaginitis Slides 2013Document97 pagesVaginitis Slides 2013leilacarvalho880% (1)
- Parasites Life CycleDocument12 pagesParasites Life CyclebretonNo ratings yet
- Vaginitis: Diagnosis and TreatmentDocument9 pagesVaginitis: Diagnosis and TreatmentAbigail MargarethaNo ratings yet
- Module 6.4 ParasitesDocument6 pagesModule 6.4 ParasitesPNo ratings yet
- CSE - SDO Pampanga - Sexual and Reproductive Health 4th Revised 2Document32 pagesCSE - SDO Pampanga - Sexual and Reproductive Health 4th Revised 2Ma Concepcion Adriano GuansingNo ratings yet
- CA 2 CDN Review Notes 2Document21 pagesCA 2 CDN Review Notes 2Andrew Del RosarioNo ratings yet
- Care of Clients With STDsDocument30 pagesCare of Clients With STDsSarah Jane MaganteNo ratings yet
- Impact of Incentives on Learning HIV Status and Condom PurchasesDocument35 pagesImpact of Incentives on Learning HIV Status and Condom PurchasesFernanda CáceresNo ratings yet
- Prevalence of Vaginitis Among Women Attending Antenatal Care Centre of Wudil General Hospital, Kano State NigeriaDocument6 pagesPrevalence of Vaginitis Among Women Attending Antenatal Care Centre of Wudil General Hospital, Kano State NigeriaUMYU Journal of Microbiology Research (UJMR)No ratings yet
- Factsheet - Livestock - ReproductiveDiseases in Cattle v2Document3 pagesFactsheet - Livestock - ReproductiveDiseases in Cattle v2lenn chandNo ratings yet
- STIs Part ADocument3 pagesSTIs Part AMihaela EneNo ratings yet
- Communicable DiseaseDocument28 pagesCommunicable DiseaseKhristine Joy NovidaNo ratings yet
- Vaginal Discharge GuidelineDocument4 pagesVaginal Discharge GuidelineGung Bagvs SaputraNo ratings yet
- Incident Action Plan (IAP)Document14 pagesIncident Action Plan (IAP)api-515948346No ratings yet
- Reproductive Diseases in Cattle: Brucellosis (Bang's Disease)Document4 pagesReproductive Diseases in Cattle: Brucellosis (Bang's Disease)Janice Li100% (1)
- VaginitisDocument54 pagesVaginitisgloria100% (1)
- Vaginitis ACOG 2006Document17 pagesVaginitis ACOG 2006xiomara andrea rios coquecoNo ratings yet
- Parasitology: Prepared By: Charriz A. AmoyanDocument99 pagesParasitology: Prepared By: Charriz A. AmoyanRaphylyn EscalonaNo ratings yet
- 4th Lecture on TrichomoniasisDocument17 pages4th Lecture on Trichomoniasisricky hutagalungNo ratings yet
- Wa0045Document96 pagesWa0045Nasser HashimNo ratings yet
- PEARSON VUE 1000 FILE Corrected 11-2017Document245 pagesPEARSON VUE 1000 FILE Corrected 11-2017Dr-Jahanzaib GondalNo ratings yet