You might also like
- The Placenta and Neurodisability 2nd EditionFrom EverandThe Placenta and Neurodisability 2nd EditionIan CrockerNo ratings yet
- Study of Respiratory Distress in Newborn: International Journal of Contemporary Pediatrics March 2017Document6 pagesStudy of Respiratory Distress in Newborn: International Journal of Contemporary Pediatrics March 2017Elison J PanggaloNo ratings yet
- Short-Term Outcomes and Mortality of Late Preterm Infants: Cahide Bulut, Tuğba Gürsoy, Fahri OvalıDocument6 pagesShort-Term Outcomes and Mortality of Late Preterm Infants: Cahide Bulut, Tuğba Gürsoy, Fahri OvalızulfikarNo ratings yet
- Risks and Outcomes of Infants with Transient Tachypnea of the NewbornDocument5 pagesRisks and Outcomes of Infants with Transient Tachypnea of the NewbornVerushka CrespoNo ratings yet
- 2174 8646 1 PBDocument5 pages2174 8646 1 PBKiran PantheeNo ratings yet
- NakatoIJP Volume6 Issue9 Pages8215-8223Document9 pagesNakatoIJP Volume6 Issue9 Pages8215-8223Siti HumairahNo ratings yet
- Martin 2017Document6 pagesMartin 2017Peregrine Albertus Ricco AzaliNo ratings yet
- Can Tey 2018Document6 pagesCan Tey 2018Desmiyati AdoeNo ratings yet
- Dengue Infection and PlacentaDocument4 pagesDengue Infection and PlacentaGabriella ArgyNo ratings yet
- Ped ProcalcitoninasepsisneoDocument11 pagesPed ProcalcitoninasepsisneoMirna Karime Gar CerNo ratings yet
- Maternal and Neonatal Risk Factors For Neonatal Respiratory Distress Syndrome in Term Neonates in Cyprus - A Prospective Case-Control StudyDocument9 pagesMaternal and Neonatal Risk Factors For Neonatal Respiratory Distress Syndrome in Term Neonates in Cyprus - A Prospective Case-Control StudyAnapaolaNo ratings yet
- Impact of Staffing On Bloodstream Infections in The Neonatal Intensive Care UnitDocument5 pagesImpact of Staffing On Bloodstream Infections in The Neonatal Intensive Care Unitزينب محمد عبدNo ratings yet
- Descriptive Study Knowing The Patients Load in The Neonatal Icu at The Tertiary Care Hospital LahoreDocument4 pagesDescriptive Study Knowing The Patients Load in The Neonatal Icu at The Tertiary Care Hospital LahoreBaru Chandrasekhar RaoNo ratings yet
- RCP y Resultados A Corto Plazo en Prematuros. JPedDocument8 pagesRCP y Resultados A Corto Plazo en Prematuros. JPedSheila Patricia Castro ErazoNo ratings yet
- VAP Incidence, Risk Factors and Bacteria in PICUDocument6 pagesVAP Incidence, Risk Factors and Bacteria in PICURabiatul 'raney' AdawiyahNo ratings yet
- Assessment of Initial Morbidity Patterns in Late Preterm Infants Relative to Those at TermDocument6 pagesAssessment of Initial Morbidity Patterns in Late Preterm Infants Relative to Those at TermInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- 5BJPCBS201005.195D20Holanda20et - Al .2C202019 PDFDocument15 pages5BJPCBS201005.195D20Holanda20et - Al .2C202019 PDFputri vinia /ilove cuteNo ratings yet
- Neonatal Infections PerspectiveDocument13 pagesNeonatal Infections PerspectiveYUDY LORENA GIRALDO ALFONSONo ratings yet
- Time Perception During Neonatal ResuscitationDocument5 pagesTime Perception During Neonatal ResuscitationVictor CarrenoNo ratings yet
- BBLR 2Document8 pagesBBLR 2Radhiatul AdillahNo ratings yet
- Clinicoetiological Profile, Management and Outcome of Neonatal Shock Presenting Within First 72 Hours of LifeDocument6 pagesClinicoetiological Profile, Management and Outcome of Neonatal Shock Presenting Within First 72 Hours of LifeIJAR JOURNALNo ratings yet
- Lung Ultrasound Score As A Predictor of Ventilator Use in Preterm Infants With Dyspnea Within 24 H After Dhospitalization PDFDocument8 pagesLung Ultrasound Score As A Predictor of Ventilator Use in Preterm Infants With Dyspnea Within 24 H After Dhospitalization PDFcesar juarezNo ratings yet
- Newborn Respiratory Distress CausesDocument5 pagesNewborn Respiratory Distress CausesNovia KurniantiNo ratings yet
- Difyeri IndiaDocument5 pagesDifyeri IndiaDian Fajar FebrianiNo ratings yet
- Clinical Profile of Fungal Sepsis in New Born: A Tertiary Centre Experience From BangladeshDocument4 pagesClinical Profile of Fungal Sepsis in New Born: A Tertiary Centre Experience From BangladeshPhilippe Ceasar C. BascoNo ratings yet
- The Problems of Moderate Preterm Infants: Seminars in PerinatologyDocument4 pagesThe Problems of Moderate Preterm Infants: Seminars in Perinatologysam crushNo ratings yet
- Klebsiella PDFDocument4 pagesKlebsiella PDFOscarEduardoNo ratings yet
- Journal Reading AnakDocument19 pagesJournal Reading AnakPutra Priambodo WibowoNo ratings yet
- Clinico-Epidemiological Profile and Predictors of Outcome in Children With Diphtheria: A Study From Northern IndiaDocument6 pagesClinico-Epidemiological Profile and Predictors of Outcome in Children With Diphtheria: A Study From Northern IndiamariaprincesitaNo ratings yet
- Umbilical Cord ClampingDocument10 pagesUmbilical Cord ClampingTika WulandariNo ratings yet
- Clinical Profile of Acute BronchiolitisDocument4 pagesClinical Profile of Acute BronchiolitisInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- 12701-50629-1-PB-1 AnakDocument4 pages12701-50629-1-PB-1 AnakAni RoseNo ratings yet
- Cap 2023Document9 pagesCap 2023Neonatología HGO4No ratings yet
- 9 JurnalDocument83 pages9 JurnalWanda AndiniNo ratings yet
- Epinephrine and Dexamethasone in Children With BronchiolitisDocument11 pagesEpinephrine and Dexamethasone in Children With BronchiolitisAdelina Wahyuni LubisNo ratings yet
- Jurnal 1Document8 pagesJurnal 1aziskarnNo ratings yet
- Acute Respiratory Distress Syndrome Among Premature Neonates: Prevalence, Mortality Rate and Risk Factors of MortalityDocument5 pagesAcute Respiratory Distress Syndrome Among Premature Neonates: Prevalence, Mortality Rate and Risk Factors of MortalityInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Predicting Outcome in Neonates With Possible Clinical Sepsis by Estimating An Early Score For Neonatal Acute Physiology-II (SNAP-II)Document8 pagesPredicting Outcome in Neonates With Possible Clinical Sepsis by Estimating An Early Score For Neonatal Acute Physiology-II (SNAP-II)ida ayu agung WijayantiNo ratings yet
- Neonatal Pneumonia Incidence and Outcomes in BangladeshDocument6 pagesNeonatal Pneumonia Incidence and Outcomes in BangladeshAnonymous Us5v7C6QhNo ratings yet
- Association Between Probiotics and Bronchopulmonary Dysplasia in Preterm InfantsDocument6 pagesAssociation Between Probiotics and Bronchopulmonary Dysplasia in Preterm InfantsDii ScottouNo ratings yet
- Aynalem 2020@journal - Pone.0235544Document14 pagesAynalem 2020@journal - Pone.0235544Huệ MinhNo ratings yet
- JurnalDocument7 pagesJurnalRahmi SilviyaniNo ratings yet
- Articulo ViernesDocument6 pagesArticulo Viernesvelf5No ratings yet
- Cute Appendicitis in Children: Emergency Department Diagnosis and ManagementDocument13 pagesCute Appendicitis in Children: Emergency Department Diagnosis and ManagementMusyawarah MelalaNo ratings yet
- Children: Antenatal Corticosteroids: Extending The Practice For Late-Preterm and Scheduled Early-Term Deliveries?Document10 pagesChildren: Antenatal Corticosteroids: Extending The Practice For Late-Preterm and Scheduled Early-Term Deliveries?ADRIANA FERNANDA MENESES AYALANo ratings yet
- Vap NicuDocument8 pagesVap NicuWiwit ClimberNo ratings yet
- May 2018 1525182462 76 PDFDocument5 pagesMay 2018 1525182462 76 PDFajes coolNo ratings yet
- Infantile Hypertrophic Pyloric Stenosis at A TertiDocument7 pagesInfantile Hypertrophic Pyloric Stenosis at A TertiVașadi Razvan CristianNo ratings yet
- Neonatal Sepsis: A Study of The Risk FactorsDocument42 pagesNeonatal Sepsis: A Study of The Risk FactorsNithin100% (3)
- In Hospital Clinical Course Among Extremely Low Birth Weight Babies Admitted in A Tertiary Care Centre in North Kerala-A Record Based StudyDocument4 pagesIn Hospital Clinical Course Among Extremely Low Birth Weight Babies Admitted in A Tertiary Care Centre in North Kerala-A Record Based StudyIJAR JOURNALNo ratings yet
- Articol 1Document7 pagesArticol 1nistor97No ratings yet
- Liberation and Mortality Outcomes in Pediatric Long Term Ventilation: A Qualitative Systematic ReviewDocument10 pagesLiberation and Mortality Outcomes in Pediatric Long Term Ventilation: A Qualitative Systematic ReviewmarleeramirezNo ratings yet
- The Incidence of Respiratory Distress Syndrome Among Preterm Infants Admitted To Neonatal Intensive Care Unit: A Retrospective StudyDocument6 pagesThe Incidence of Respiratory Distress Syndrome Among Preterm Infants Admitted To Neonatal Intensive Care Unit: A Retrospective StudyImin BuntaraNo ratings yet
- Management of Premature Rupture of Membranes: Ashraf Olabi and Lucy Shikh MousaDocument7 pagesManagement of Premature Rupture of Membranes: Ashraf Olabi and Lucy Shikh MousaDesi SafiraNo ratings yet
- 1 s2.0 S0022347606011851 MainDocument4 pages1 s2.0 S0022347606011851 Main1200009No ratings yet
- Early Hydrocortisone Dosing and Mortality in Premature InfantsDocument13 pagesEarly Hydrocortisone Dosing and Mortality in Premature InfantsIntan Karnina PutriNo ratings yet
- Neonatal Outcomes of Extremely Preterm Infants From The NICHD Neonatal Research NetworkDocument14 pagesNeonatal Outcomes of Extremely Preterm Infants From The NICHD Neonatal Research NetworkKattia FloresNo ratings yet
- Escala BronquiolitisDocument13 pagesEscala BronquiolitisconfesionesdeunatreintaneraNo ratings yet
- Wynn 2016 Defining Neonatal SepsisDocument11 pagesWynn 2016 Defining Neonatal SepsisEllya Latifah IlyasNo ratings yet
- ArticolDocument16 pagesArticolNeagu MariusNo ratings yet
- Articol RJML 2017Document5 pagesArticol RJML 2017MariusNo ratings yet
- Medical Education From Mass-Media 2016Document15 pagesMedical Education From Mass-Media 2016MariusNo ratings yet
- Journal of Surgery: Gas Gangrene: Case Presentation and Literature DataDocument4 pagesJournal of Surgery: Gas Gangrene: Case Presentation and Literature DataMariusNo ratings yet
- Reality or Myth 2014Document14 pagesReality or Myth 2014MariusNo ratings yet
- Viral Respiratory Infections in Preterm Infants During andDocument9 pagesViral Respiratory Infections in Preterm Infants During andMariusNo ratings yet
- Utility of Autopsy in Medical Education - Students' Opinions and AttitudesDocument7 pagesUtility of Autopsy in Medical Education - Students' Opinions and AttitudesMariusNo ratings yet
- Medical Education From Mass-Media 2016Document15 pagesMedical Education From Mass-Media 2016MariusNo ratings yet
- Outcome of Coronavirus Spectrum Infections PDFDocument9 pagesOutcome of Coronavirus Spectrum Infections PDFMichell MarinsNo ratings yet
- Ethical Challenges in Aesthetic DentistryDocument3 pagesEthical Challenges in Aesthetic DentistryMariusNo ratings yet
- Postmortem Examination of COVID-19 Patients RevealsDocument12 pagesPostmortem Examination of COVID-19 Patients RevealsMariusNo ratings yet
- Qualitative Research Methods A Data Collector S Field GuideDocument136 pagesQualitative Research Methods A Data Collector S Field Guidecartegratuita100% (7)
- Prevalence of SARS-CoV-2 Among Patients Admitted For Childbirth in Southern Connecticut.Document3 pagesPrevalence of SARS-CoV-2 Among Patients Admitted For Childbirth in Southern Connecticut.Uri BvNo ratings yet
- Risks of Novel Coronavirus Disease (COVID-19) in Preg-Nancy A Narrative ReviewDocument5 pagesRisks of Novel Coronavirus Disease (COVID-19) in Preg-Nancy A Narrative ReviewdalauNo ratings yet
- Postmortem Examination of COVID-19 Patients RevealsDocument12 pagesPostmortem Examination of COVID-19 Patients RevealsMariusNo ratings yet
- Prevalence of SARS-CoV-2 Among Patients Admitted For Childbirth in Southern Connecticut.Document3 pagesPrevalence of SARS-CoV-2 Among Patients Admitted For Childbirth in Southern Connecticut.Uri BvNo ratings yet
- Outcome of Coronavirus Spectrum Infections PDFDocument9 pagesOutcome of Coronavirus Spectrum Infections PDFMichell MarinsNo ratings yet
- Qualitative Research Methods A Data Collector S Field GuideDocument136 pagesQualitative Research Methods A Data Collector S Field Guidecartegratuita100% (7)
- Can p63 Serve As A Biomarker For Giant Cell TumorDocument7 pagesCan p63 Serve As A Biomarker For Giant Cell TumorMariusNo ratings yet
- Risks of Novel Coronavirus Disease (COVID-19) in Preg-Nancy A Narrative ReviewDocument5 pagesRisks of Novel Coronavirus Disease (COVID-19) in Preg-Nancy A Narrative ReviewdalauNo ratings yet
- Qualitative Research Methods A Data Collector S Field GuideDocument136 pagesQualitative Research Methods A Data Collector S Field Guidecartegratuita100% (7)
- RMD - Lightmix Modular CE IVD Assay BrochureDocument4 pagesRMD - Lightmix Modular CE IVD Assay BrochureDummy Tester JrNo ratings yet
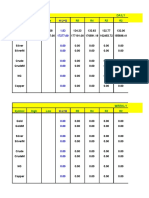
- Symbol High Low R5 R4 R3 R2: DailyDocument8 pagesSymbol High Low R5 R4 R3 R2: Daily257597 rmp.mech.16No ratings yet
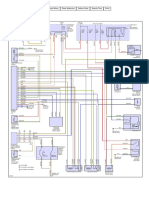
- Aire Acondicionado Mazda 3 2006Document2 pagesAire Acondicionado Mazda 3 2006Jhon ConnorNo ratings yet
- Experiment 1 Marble Race Virtual Science Lab Chem 2Document4 pagesExperiment 1 Marble Race Virtual Science Lab Chem 2Oribe, Narciso A.100% (1)
- CSC 101-CSC 111 - Introduction To Computer Science - Lecture 1Document23 pagesCSC 101-CSC 111 - Introduction To Computer Science - Lecture 1CODE100% (1)
- Test A: Reading - Passage 1Document29 pagesTest A: Reading - Passage 1barishyayNo ratings yet
- Yıldız Technical University - Program Information Form - Page 1/9Document9 pagesYıldız Technical University - Program Information Form - Page 1/9Elsaadawi MohamedNo ratings yet
- MINDFULNESS CALENDARDocument1 pageMINDFULNESS CALENDARNiccy McOrrieNo ratings yet
- Will The Real SMART Goals Please Stand Up?: Robert S. Rubin Saint Louis UniversityDocument2 pagesWill The Real SMART Goals Please Stand Up?: Robert S. Rubin Saint Louis UniversityKyoko TakayanagiNo ratings yet
- Aiesha Edward Resume2Document2 pagesAiesha Edward Resume2api-491571342No ratings yet
- Implementation of Swachh Bharat in MysoreDocument13 pagesImplementation of Swachh Bharat in MysoreDipyaman ChoudhuryNo ratings yet
- 2020 End Year 6 PenulisanDocument8 pages2020 End Year 6 PenulisanZulhillmi ZainuddinNo ratings yet
- Market ReseachDocument3 pagesMarket ReseachSam Cy PuyalesNo ratings yet
- Glover 6e - Chapter 02Document41 pagesGlover 6e - Chapter 02JIGNESH DESAINo ratings yet
- FD2000 DatasheetDocument2 pagesFD2000 DatasheetIvan MihajlovicNo ratings yet
- LC Used in ProteimicsDocument15 pagesLC Used in ProteimicsMandu ManNo ratings yet
- Tutorial Sheet 4Document2 pagesTutorial Sheet 4Syed YousufuddinNo ratings yet
- Kristeva On Melanie Klein's "Oresteia"Document6 pagesKristeva On Melanie Klein's "Oresteia"danthetoasterNo ratings yet
- Ishrae 365 2009 PDFDocument16 pagesIshrae 365 2009 PDFZeeshan HasanNo ratings yet
- Cambridge BiologyDocument78 pagesCambridge BiologyBraweet SapkotaNo ratings yet
- MIS DPCR IPCR July To December 2018 - Summary ListDocument14 pagesMIS DPCR IPCR July To December 2018 - Summary ListZyreen Kate BC100% (1)
- GRADES 1 To 12 Daily Lesson LogDocument5 pagesGRADES 1 To 12 Daily Lesson LogFlordeliza Manaois RamosNo ratings yet
- NCM 106 Acute Biologic CrisisDocument142 pagesNCM 106 Acute Biologic CrisisEllamae Chua88% (8)
- Apcosil 605Document1 pageApcosil 605rihtak123No ratings yet
- Economic Case for Immobilizing EnzymesDocument25 pagesEconomic Case for Immobilizing EnzymesNikki ChauhanNo ratings yet
- Land Tenure SystemsDocument140 pagesLand Tenure SystemsjoeclintNo ratings yet
- S# Isin CFI Code (As Per New ISO) Security Name Security Symbol Sector Name Security Type StatusDocument25 pagesS# Isin CFI Code (As Per New ISO) Security Name Security Symbol Sector Name Security Type StatusahmedalishNo ratings yet
- Laughter Yoga Benefits Workplace ProductivityDocument2 pagesLaughter Yoga Benefits Workplace ProductivityJose Manuel Araujo OrregoNo ratings yet
- Guided Noteboo Kin GED10 2 (Mathe Matics in The Modern World)Document5 pagesGuided Noteboo Kin GED10 2 (Mathe Matics in The Modern World)Chenie BatacNo ratings yet