You might also like
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5795)
- Peripheral Nerve and Muscular WeaknessDocument17 pagesPeripheral Nerve and Muscular WeaknessSamuel kuriaNo ratings yet
- Leukamia and Transfusion MedicineDocument26 pagesLeukamia and Transfusion MedicineSamuel kuriaNo ratings yet
- Disorders of The PancreaseDocument14 pagesDisorders of The PancreaseSamuel kuriaNo ratings yet
- Haematological DisordersDocument28 pagesHaematological DisordersSamuel kuriaNo ratings yet
- Glomerular DiseasesDocument16 pagesGlomerular DiseasesSamuel kuriaNo ratings yet
- Disorders of Small IntestineDocument41 pagesDisorders of Small IntestineSamuel kuriaNo ratings yet
- Acute and Chronic Kidney DiseaseDocument17 pagesAcute and Chronic Kidney DiseaseSamuel kuriaNo ratings yet
- DementiaDocument11 pagesDementiaSamuel kuriaNo ratings yet
- Disorders of Esophagus and StomachDocument29 pagesDisorders of Esophagus and StomachSamuel kuriaNo ratings yet
- Acute Liver FailureDocument29 pagesAcute Liver FailureSamuel kuriaNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
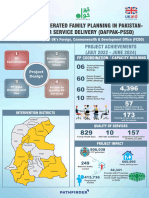
- Poster Sindh 2-01-2024Document11 pagesPoster Sindh 2-01-2024FM Printers111No ratings yet
- Pain Managementin TemporomandibularDocument10 pagesPain Managementin Temporomandibularirfanadil2006No ratings yet
- Borrescio-Higa Valenzuela - Gender Inequality and Mental Health.Document9 pagesBorrescio-Higa Valenzuela - Gender Inequality and Mental Health.Firdaus Silabi Al-AttarNo ratings yet
- HayalllDocument41 pagesHayalllchalie tarekegnNo ratings yet
- Can Your Baby Get Pregnant If You Have Sex While PregnantDocument6 pagesCan Your Baby Get Pregnant If You Have Sex While Pregnanteng-scribd100% (2)
- Mobile Phone Addiction Among YouthDocument10 pagesMobile Phone Addiction Among Youthda dadadfgNo ratings yet
- Niche and Sub-NicheDocument3 pagesNiche and Sub-NichehoneybeeNo ratings yet
- Universiti Kuala Lumpur Royal College of Medicine Perak: Year 3 Module Handbook (Medicine) 2014-2015Document15 pagesUniversiti Kuala Lumpur Royal College of Medicine Perak: Year 3 Module Handbook (Medicine) 2014-2015Codillia CheongNo ratings yet
- SOP-32-06 - Vendor Assessment (Oct 21)Document11 pagesSOP-32-06 - Vendor Assessment (Oct 21)parwana formuliNo ratings yet
- Crohn's Disease Seminar FinalDocument27 pagesCrohn's Disease Seminar Finalshahad alshareefNo ratings yet
- Addisons DiseaseDocument1 pageAddisons DiseaseAndreia Palade100% (1)
- q2 Grade 7 Health DLL Week 1Document8 pagesq2 Grade 7 Health DLL Week 1johann reyes0% (1)
- American Journal of Infection ControlDocument6 pagesAmerican Journal of Infection ControlfathimzahroNo ratings yet
- Paper 2 - Abisha AliDocument7 pagesPaper 2 - Abisha Aliapi-269596566No ratings yet
- DM No. 2022-0287 Updated Moa and Tor PRDPDocument8 pagesDM No. 2022-0287 Updated Moa and Tor PRDPDRMC Infirmary100% (1)
- PEBC Qualifying Exam References and Resources ListDocument5 pagesPEBC Qualifying Exam References and Resources ListAnkit ShahNo ratings yet
- Soal PAS BIG Xi, SMT 3, OnlineDocument10 pagesSoal PAS BIG Xi, SMT 3, OnlineRivaldi Lukman HakimNo ratings yet
- Cebu Technological University: Main CampusDocument2 pagesCebu Technological University: Main CampusLeonard Patrick Faunillan BaynoNo ratings yet
- Aggregates - Limestone Dolomite Safety Data SheetDocument8 pagesAggregates - Limestone Dolomite Safety Data SheetJEAN KATHLEEN SORIANONo ratings yet
- K5 - Sistem Informasi KesehatanDocument29 pagesK5 - Sistem Informasi KesehatanPusvaNurmalaSariNo ratings yet
- R.A. No. 6969 - Brown GroupDocument35 pagesR.A. No. 6969 - Brown GroupAngelNo ratings yet
- An Tropo Metri Status GiziDocument73 pagesAn Tropo Metri Status GiziMochammad Fariz AmsalNo ratings yet
- GL3655EDocument0 pagesGL3655EandyhrNo ratings yet
- The Sleep Doctor'S Diet Plan by Michael Breuss, PHD The Sleep Doctor'S Diet PlanDocument5 pagesThe Sleep Doctor'S Diet Plan by Michael Breuss, PHD The Sleep Doctor'S Diet PlanshubhangivsNo ratings yet
- Mindfulness Exercise 1: Attending To BreAthingDocument2 pagesMindfulness Exercise 1: Attending To BreAthingcruz210No ratings yet
- Chain of Hope Teams With Gift of LifeDocument1 pageChain of Hope Teams With Gift of LifeJonathan DanosNo ratings yet
- Veterans Affairs Presumptive Service Connection and Disability CompensationDocument33 pagesVeterans Affairs Presumptive Service Connection and Disability CompensationChuck Achberger100% (1)
- Biological Warfare Agents - AgronDocument129 pagesBiological Warfare Agents - AgronMARK ARQUE LACANARIANo ratings yet
- Professional Development Plan PPT 1Document10 pagesProfessional Development Plan PPT 1api-355484042No ratings yet
- Inpatient Management of Adolescents With Eating Disorders ToolkitDocument191 pagesInpatient Management of Adolescents With Eating Disorders ToolkitAjutor Anorexie-BulimieNo ratings yet