You might also like
- Ulcerative ColitisDocument63 pagesUlcerative ColitismahalakshmiNo ratings yet
- Biliary Tract DiseaseDocument52 pagesBiliary Tract DiseaseAna Cotoman100% (1)
- Inflammatory Bowel Disease: Younes R YounesDocument38 pagesInflammatory Bowel Disease: Younes R YounesDarawan MirzaNo ratings yet
- Dr. Arif Gunawan Teguh WDocument64 pagesDr. Arif Gunawan Teguh WarifgteguhNo ratings yet
- WelcomeDocument60 pagesWelcomepandem soniyaNo ratings yet
- Digestive System Disorder AssessmentDocument50 pagesDigestive System Disorder AssessmentTaate MohammedNo ratings yet
- (SurgPath) Small and Large IntestinesDocument122 pages(SurgPath) Small and Large Intestinesa20-0353-958No ratings yet
- Inflammatory Bowel Disease: By: Yilak G. Augst 2015Document44 pagesInflammatory Bowel Disease: By: Yilak G. Augst 2015TESFAYE YIRSAWNo ratings yet
- Biliary Tract Disease - Emmet AndrewsDocument52 pagesBiliary Tract Disease - Emmet AndrewsBoneyJalgarNo ratings yet
- Biliary Tract DiseaseDocument40 pagesBiliary Tract DiseaseIsaac MwangiNo ratings yet
- Biliary Tree LectureDocument58 pagesBiliary Tree Lecturesgod34No ratings yet
- Inflammatory Bowel Disease: 7 Year DR Felix MicheloDocument55 pagesInflammatory Bowel Disease: 7 Year DR Felix MicheloFreeburn SimunchembuNo ratings yet
- Disorders of Esophagus and StomachDocument29 pagesDisorders of Esophagus and StomachSamuel kuriaNo ratings yet
- Acute Abdominal Emergencies GuideDocument126 pagesAcute Abdominal Emergencies GuidekityamuwesiNo ratings yet
- Chronic DiarrheaDocument38 pagesChronic DiarrheaShujina ZainabNo ratings yet
- Approach To GI DisordersDocument28 pagesApproach To GI DisordersdrvivekshimlaNo ratings yet
- 5.5 GI Disorders Dr. Jison 2022Document72 pages5.5 GI Disorders Dr. Jison 2022Monique BorresNo ratings yet
- General Surgery SMALL INTESTINES-Dr MendozaDocument101 pagesGeneral Surgery SMALL INTESTINES-Dr MendozaMedisina101No ratings yet
- Ulcerative ColitisDocument18 pagesUlcerative ColitisKyle Ü D. CunanersNo ratings yet
- 8 28 12 R Schaffer MDDocument51 pages8 28 12 R Schaffer MDKay BristolNo ratings yet
- Chronic Diarrhea and Malabsorption: Causes and TreatmentDocument25 pagesChronic Diarrhea and Malabsorption: Causes and TreatmentadelekeyusufNo ratings yet
- Colon 2Document56 pagesColon 2EnydLaRejNo ratings yet
- Acute Pancreatitis, HemakshiDocument25 pagesAcute Pancreatitis, HemakshiUmair FirdousNo ratings yet
- Powerpoint: Chronic Inflammatory DisordesDocument55 pagesPowerpoint: Chronic Inflammatory Disordesj.doe.hex_87No ratings yet
- Gastro Intestinal Disorders: Assessment, Conditions, & ManagementDocument84 pagesGastro Intestinal Disorders: Assessment, Conditions, & ManagementBryan GrafftNo ratings yet
- Сhronic pancreatitis: Lykhatska G.VDocument42 pagesСhronic pancreatitis: Lykhatska G.VOlga CîrsteaNo ratings yet
- Disorders of Biliary SystemDocument29 pagesDisorders of Biliary SystemAjibola OlamideNo ratings yet
- Pancreatitis: M.N. Homoeopathic Medical College & Research Institute, Bikaner B.H.M.S. III YearDocument36 pagesPancreatitis: M.N. Homoeopathic Medical College & Research Institute, Bikaner B.H.M.S. III YearYamini SoniNo ratings yet
- Inflammatory Bowel DiseaseDocument40 pagesInflammatory Bowel DiseaseSK TalkNo ratings yet
- Eric Ji-Yuan Mao, MD Samir A. Shah, MD, Facg, Fasge, AgafDocument18 pagesEric Ji-Yuan Mao, MD Samir A. Shah, MD, Facg, Fasge, AgafMuhammad GassanNo ratings yet
- Gastrointestinal Bleeding Causes, Symptoms and TreatmentDocument84 pagesGastrointestinal Bleeding Causes, Symptoms and TreatmentAngela Kristiana IntanNo ratings yet
- Askep PankreatitisDocument48 pagesAskep PankreatitisYeni DwiNo ratings yet
- Acute PancreatitisDocument36 pagesAcute PancreatitisURo KkuNo ratings yet
- 07a. Non Neoplastic Disease of OesophagusDocument35 pages07a. Non Neoplastic Disease of Oesophagus21701101016 - Juliana Ayu NugrahaNo ratings yet
- The Digestive System: and ItsDocument102 pagesThe Digestive System: and ItsRhea Andrea Uy100% (1)
- By DR.: Haitham Mokhtar Mohamed Abd AllahDocument101 pagesBy DR.: Haitham Mokhtar Mohamed Abd AllahMohamed ElkadyNo ratings yet
- Small and Large IntestineDocument124 pagesSmall and Large IntestinemariahemnksNo ratings yet
- Based on the information provided, the most likely causative organism is Cytomegalovirus (CMV). CMV is a common opportunistic infection in HIV/AIDS patients that can cause esophageal ulcersDocument37 pagesBased on the information provided, the most likely causative organism is Cytomegalovirus (CMV). CMV is a common opportunistic infection in HIV/AIDS patients that can cause esophageal ulcersDanielle FosterNo ratings yet
- Case 5 - Pancreatitis-1Document4 pagesCase 5 - Pancreatitis-1ngNo ratings yet
- Chronic Diarrhea Differential Diagnosis and TreatmentDocument37 pagesChronic Diarrhea Differential Diagnosis and TreatmentAzima AyobNo ratings yet
- IBD Treatment Options for Ulcerative Colitis and Crohn's DiseaseDocument41 pagesIBD Treatment Options for Ulcerative Colitis and Crohn's DiseaseririNo ratings yet
- Colonic and Small Intestine Disorders-1Document28 pagesColonic and Small Intestine Disorders-1YIKI ISAACNo ratings yet
- 5. Chronic pancreatitis. СholelithiasisDocument58 pages5. Chronic pancreatitis. Сholelithiasischai rinNo ratings yet
- Problem 5 GIT Kelompok 16Document116 pagesProblem 5 GIT Kelompok 16Andreas AdiwinataNo ratings yet
- Small & Large Bowel SlidesDocument17 pagesSmall & Large Bowel SlidesHunter ClontsNo ratings yet
- Intestinal Diseases in Cattle 2023Document30 pagesIntestinal Diseases in Cattle 2023Krystyna WędrychowskaNo ratings yet
- NCM 116 Care of Clients With Ibs Malabsorp Ulcerative Colitis Crohns PDFDocument35 pagesNCM 116 Care of Clients With Ibs Malabsorp Ulcerative Colitis Crohns PDFKathlyn Joy DulayNo ratings yet
- Kronik PankreatitisDocument41 pagesKronik PankreatitisEko RistiyantoNo ratings yet
- Pitri - GI.Pemicu 4. GE+ Tifus AbdominalisDocument154 pagesPitri - GI.Pemicu 4. GE+ Tifus AbdominalisCunCunAlAndraNo ratings yet
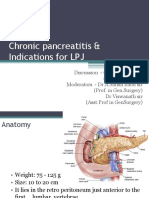
- Chronic Pancreatitis & Indications For LPJDocument73 pagesChronic Pancreatitis & Indications For LPJRadityo Budi LeksonoNo ratings yet
- Pemicu 5 GIT DevinDocument131 pagesPemicu 5 GIT DevinDevin AlexanderNo ratings yet
- Pancreatitis: Causes, Symptoms, and TreatmentDocument5 pagesPancreatitis: Causes, Symptoms, and TreatmentSanthu Su100% (2)
- Approach To Patient With Gall StoneDocument11 pagesApproach To Patient With Gall StonengussutsegawNo ratings yet
- Colilithiasis 2Document53 pagesColilithiasis 2Worku KifleNo ratings yet
- Biliary&Pancreas DisordersDocument34 pagesBiliary&Pancreas DisordersLarry De LaraNo ratings yet
- Examen IM-gastroenterologieDocument15 pagesExamen IM-gastroenterologieNicola BereholschiNo ratings yet
- Southern Luzon State University case analysis on pancreatitisDocument39 pagesSouthern Luzon State University case analysis on pancreatitisAleks MendozaNo ratings yet
- Gastrointestinal Tract (Partial Edit)Document47 pagesGastrointestinal Tract (Partial Edit)applesncoreNo ratings yet
- Pead 3 - Abdominal Pain and VommitingDocument22 pagesPead 3 - Abdominal Pain and Vommitingbbyes100% (1)
- Non Viral Causes of HepatitisDocument20 pagesNon Viral Causes of HepatitisSamuel kuriaNo ratings yet
- Seizure and EpilepsyDocument17 pagesSeizure and EpilepsySamuel kuriaNo ratings yet
- Nephrology 2Document16 pagesNephrology 2Samuel kuriaNo ratings yet
- Peripheral Nerve and Muscular WeaknessDocument17 pagesPeripheral Nerve and Muscular WeaknessSamuel kuriaNo ratings yet
- Neurological DiseaseDocument15 pagesNeurological DiseaseSamuel kuriaNo ratings yet
- NephrologyDocument17 pagesNephrologySamuel kuriaNo ratings yet
- Liver DiseaseDocument20 pagesLiver DiseaseSamuel kuriaNo ratings yet
- Haematological DisordersDocument28 pagesHaematological DisordersSamuel kuriaNo ratings yet
- Disorders of The PancreaseDocument14 pagesDisorders of The PancreaseSamuel kuriaNo ratings yet
- Git BleedingDocument12 pagesGit BleedingSamuel kuriaNo ratings yet
- Glomerular DiseasesDocument16 pagesGlomerular DiseasesSamuel kuriaNo ratings yet
- Leukamia and Transfusion MedicineDocument26 pagesLeukamia and Transfusion MedicineSamuel kuriaNo ratings yet
- Liver CirrhosisDocument22 pagesLiver CirrhosisSamuel kuriaNo ratings yet
- Disorders of Gastrointestinal Tract, Hepatobiliary System andDocument10 pagesDisorders of Gastrointestinal Tract, Hepatobiliary System andSamuel kuriaNo ratings yet
- Brain InfectionsDocument28 pagesBrain InfectionsSamuel kuriaNo ratings yet
- AcdDocument14 pagesAcdSamsul BahriNo ratings yet
- Disorders of LeucocytesDocument12 pagesDisorders of LeucocytesSamuel kuriaNo ratings yet
- Acute and Chronic Kidney DiseaseDocument17 pagesAcute and Chronic Kidney DiseaseSamuel kuriaNo ratings yet
- DementiaDocument11 pagesDementiaSamuel kuriaNo ratings yet
- Disorders of Esophagus and StomachDocument29 pagesDisorders of Esophagus and StomachSamuel kuriaNo ratings yet
- Acute Liver FailureDocument29 pagesAcute Liver FailureSamuel kuriaNo ratings yet
- Faecal AnalysisDocument83 pagesFaecal AnalysisJoseph SabidoNo ratings yet
- Celiac Disease FinalDocument7 pagesCeliac Disease FinalacholineNo ratings yet
- Malabsorption SyndromeDocument31 pagesMalabsorption SyndromeSahilSharma100% (1)
- Approach To Malabsorption (SANJAY)Document58 pagesApproach To Malabsorption (SANJAY)Sanjay KumarNo ratings yet
- Malabsorbsi 2Document33 pagesMalabsorbsi 2Handa YaniNo ratings yet
- Enteral Nutrition GI Disorders - Olivier GouletDocument60 pagesEnteral Nutrition GI Disorders - Olivier GouletBayu KurniawanNo ratings yet
- Laboratory ValuesDocument12 pagesLaboratory ValuesJaney Co100% (2)
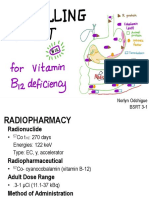
- Schilling TestDocument13 pagesSchilling TestLyn OdchigueNo ratings yet
- Case Study 1-1Document9 pagesCase Study 1-1api-242226130No ratings yet
- Fat MalabsorptionDocument14 pagesFat MalabsorptionTahir MalikNo ratings yet
- Microsoft PowerPoint - Pediatric GI Function CorrectDocument126 pagesMicrosoft PowerPoint - Pediatric GI Function CorrectArchanaNo ratings yet
- Juhairina: Medical Nutrition Therapy For Disorders of The Lower Gastrointestinal TractDocument82 pagesJuhairina: Medical Nutrition Therapy For Disorders of The Lower Gastrointestinal Tractdesy100% (1)
- Macrocytosis - Macrocytic Anemia - UpToDateDocument36 pagesMacrocytosis - Macrocytic Anemia - UpToDateMarvin VillanuevaNo ratings yet
- CMS Medicine 4 (Q&A)Document59 pagesCMS Medicine 4 (Q&A)M. Baidar SaeedNo ratings yet
- Fat Malabsorption in Critical IllnessDocument6 pagesFat Malabsorption in Critical Illnesslakshminivas PingaliNo ratings yet
- Giardia LambliaDocument13 pagesGiardia LambliaindahdwitasariNo ratings yet
- Starvation Biochem NotesDocument8 pagesStarvation Biochem NotesNkosi JupiterNo ratings yet
- Celiac Disease - Case StudyDocument29 pagesCeliac Disease - Case StudyRye HanaNo ratings yet
- Disease: Renal (Dialysis) : Martínez Montes de Oca Jessica. Reyes Del Angel NaimeDocument6 pagesDisease: Renal (Dialysis) : Martínez Montes de Oca Jessica. Reyes Del Angel NaimeOmar De LeonNo ratings yet
- Clinical Manifestations, Diagnosis, and Prognosis of Crohn Disease in Adults - UpToDateDocument45 pagesClinical Manifestations, Diagnosis, and Prognosis of Crohn Disease in Adults - UpToDateAsclepioNo ratings yet
- Nutrition and Liver DiseasesDocument29 pagesNutrition and Liver DiseasesBia Khan100% (1)
- Compiled Do or Die Physio CAT 1 ShowDocument99 pagesCompiled Do or Die Physio CAT 1 ShowSaktai DiyamiNo ratings yet
- NutriDiet ReviewerDocument6 pagesNutriDiet ReviewerCherry BoticarioNo ratings yet
- Non-IgE-mediated Gastrointestinal Food AllergyDocument11 pagesNon-IgE-mediated Gastrointestinal Food AllergyJose Antonio VenacostaNo ratings yet
- Nurseslabs Gi Diseases Nursing Quiz 4Document6 pagesNurseslabs Gi Diseases Nursing Quiz 4Yenny PepitoNo ratings yet
- Management of StomasDocument22 pagesManagement of Stomasmhany12345No ratings yet
- Intestinal FailureDocument586 pagesIntestinal FailurePolyvios Papadimitropoulos67% (3)
- Understanding Short Bowel Syndrome Current StatusDocument10 pagesUnderstanding Short Bowel Syndrome Current StatusMolgen PanjaitanNo ratings yet
- SpringerDocument164 pagesSpringerriri siahaanNo ratings yet
- Approach To Chronic Diarrhea: Moderator-Dr - Ramesh M Presenter-Dr - Deena Kumari SDocument68 pagesApproach To Chronic Diarrhea: Moderator-Dr - Ramesh M Presenter-Dr - Deena Kumari SDana KNo ratings yet