You might also like
- Oral Presentation Assessment RubricDocument2 pagesOral Presentation Assessment Rubricapi-280384763100% (4)
- Polyhydramnios CASE STUDYDocument17 pagesPolyhydramnios CASE STUDYamit86% (37)
- Cot in Math 5Document4 pagesCot in Math 5Elpidio Directo100% (2)
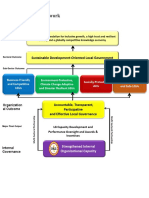
- DILG Outcome FrameworkDocument6 pagesDILG Outcome FrameworkGabo GarboNo ratings yet
- Nursing Care Plan of The MotherDocument20 pagesNursing Care Plan of The Motherbuang2390% (382)
- Growth comparison of breast vs formula fed neonatesDocument7 pagesGrowth comparison of breast vs formula fed neonatesOman SantosoNo ratings yet
- Process of EvaluationDocument28 pagesProcess of EvaluationNaeem JanNo ratings yet
- Toolkit Trainers Guide Training of TrainersDocument91 pagesToolkit Trainers Guide Training of TrainersnzcruiserNo ratings yet
- Problem StatementDocument7 pagesProblem StatementpriyankaNo ratings yet
- Midwifery and Obstetrical Nursing CourseDocument24 pagesMidwifery and Obstetrical Nursing CourseSudipta Kumar BeraNo ratings yet
- Community and Health NursingDocument22 pagesCommunity and Health NursingRam TyagiNo ratings yet
- Position Paper Module 11Document18 pagesPosition Paper Module 11ckayNo ratings yet
- Problem Statement 5Document17 pagesProblem Statement 5priyankaNo ratings yet
- Case Study in Obstetrics and Gynaecology - Lecture Notes, Study Material and Important Questions, AnswersDocument11 pagesCase Study in Obstetrics and Gynaecology - Lecture Notes, Study Material and Important Questions, AnswersM.V. TV100% (2)
- Research Article: An Assessment of The Breastfeeding Practices and Infant Feeding Pattern Among Mothers in MauritiusDocument9 pagesResearch Article: An Assessment of The Breastfeeding Practices and Infant Feeding Pattern Among Mothers in MauritiusNurhikmah RnNo ratings yet
- Nursing Research PaperDocument14 pagesNursing Research Paperapi-735739064No ratings yet
- Perceptions and Practices Regarding Breastfeeding Among Postnatal Women at A District Tertiary Referral Government Hospital in Southern IndiaDocument7 pagesPerceptions and Practices Regarding Breastfeeding Among Postnatal Women at A District Tertiary Referral Government Hospital in Southern IndiaJamby VivasNo ratings yet
- Maternal Profiles and Social Determinants of Malnutrition and The MDGS: What Have We Learnt?Document12 pagesMaternal Profiles and Social Determinants of Malnutrition and The MDGS: What Have We Learnt?FaniaParra FaniaNo ratings yet
- Nutrients 14 05060Document25 pagesNutrients 14 05060fkik unibNo ratings yet
- Assessment of The Knowledge and Attitude of Infants' Mothers From Bushehr (Iran) On Food Security Using Anthropometric Indicators in 2016: A Cross-Sectional StudyDocument13 pagesAssessment of The Knowledge and Attitude of Infants' Mothers From Bushehr (Iran) On Food Security Using Anthropometric Indicators in 2016: A Cross-Sectional Studynewbire vlogNo ratings yet
- Nutrients 13 02376Document28 pagesNutrients 13 02376Garuba Olayinka DhikrullahiNo ratings yet
- Mothers' Attitudes on Childhood Obesity PreventionDocument5 pagesMothers' Attitudes on Childhood Obesity PreventionSENGOTTUVEL CHENNIAPPANNo ratings yet
- Children 09 01773 v3Document11 pagesChildren 09 01773 v3Agustina SisterNo ratings yet
- Research ReportDocument8 pagesResearch ReportAbid SherazNo ratings yet
- Nutrition Education Programs Aimed at African Mothers of Infant Children A Systematic ReviewDocument19 pagesNutrition Education Programs Aimed at African Mothers of Infant Children A Systematic ReviewDicky Estosius TariganNo ratings yet
- Determinants of Exclusive Breastfeeding Practices of Female Healthcare Workers in Jakarta, IndonesiaDocument7 pagesDeterminants of Exclusive Breastfeeding Practices of Female Healthcare Workers in Jakarta, IndonesiaAsriniNo ratings yet
- Human Milk Benefits and Breastfeeding: Fani AnatolitouDocument8 pagesHuman Milk Benefits and Breastfeeding: Fani AnatolitouAndreafika HarqiqiNo ratings yet
- Timely Introduction of Complementary Feeding Among Caregivers of Children 612 Month Sodo Town EthiopiaDocument3 pagesTimely Introduction of Complementary Feeding Among Caregivers of Children 612 Month Sodo Town EthiopiaProdi S1- 1BNo ratings yet
- Breast-Feeding Performance Index - A Composite Index To Describe Overall Breast-Feeding Performance Among Infants Under 6 Months of AgeDocument9 pagesBreast-Feeding Performance Index - A Composite Index To Describe Overall Breast-Feeding Performance Among Infants Under 6 Months of AgeHuan VuongNo ratings yet
- Nutricional DE COCO para La Supervivencia Infantil.Document6 pagesNutricional DE COCO para La Supervivencia Infantil.alexis fernandez ramosNo ratings yet
- Nutrients 15 00988Document17 pagesNutrients 15 00988VIRGINA PUTRINo ratings yet
- Breastfeeding Is An Unsurpassed Method of Providing Ideal Food For The Healthy Growth and Development of InfantsDocument4 pagesBreastfeeding Is An Unsurpassed Method of Providing Ideal Food For The Healthy Growth and Development of InfantsSatra SabbuhNo ratings yet
- Nutrients 04 00859Document16 pagesNutrients 04 00859RameRed LiNo ratings yet
- Who NMH NHD 14.3 EngDocument12 pagesWho NMH NHD 14.3 EngHanny Hernadha Putri DharmawanNo ratings yet
- Jurnal 1Document11 pagesJurnal 1Retno KurniawatiNo ratings yet
- Knowledge and attitude of primigravida mothers regarding antenatal dietDocument6 pagesKnowledge and attitude of primigravida mothers regarding antenatal dietNeha RanaNo ratings yet
- Management of Common Lactation and Breastfeeding Problems: Lisa H. Amir and Verity H. LivingstoneDocument27 pagesManagement of Common Lactation and Breastfeeding Problems: Lisa H. Amir and Verity H. LivingstoneRio Michelle CorralesNo ratings yet
- Breast FeedingDocument17 pagesBreast FeedingMarjorie IntongNo ratings yet
- Abed,+1114 Impacts+of+Dietary+Supplements+and+Nutrient Rich+Food+for+Pregnant+Women+on+Birth+Weight+in+Sugh+El Chmis Alkhoms+–+LiDocument8 pagesAbed,+1114 Impacts+of+Dietary+Supplements+and+Nutrient Rich+Food+for+Pregnant+Women+on+Birth+Weight+in+Sugh+El Chmis Alkhoms+–+LiLydia LuciusNo ratings yet
- NXZ 079Document9 pagesNXZ 079plavado3756No ratings yet
- Gizkes LanjutDocument8 pagesGizkes LanjutSaeful AnhariNo ratings yet
- Adolescent Pregnancy and Linear Growth of Infants: A Birth Cohort Study in Rural EthiopiaDocument9 pagesAdolescent Pregnancy and Linear Growth of Infants: A Birth Cohort Study in Rural EthiopiaLeonardo AzevedoNo ratings yet
- BreastfeedingDocument13 pagesBreastfeedingSintya AulinaNo ratings yet
- Malnutrition-Journal WDocument11 pagesMalnutrition-Journal Wgeng gengNo ratings yet
- 2018 Article 1076Document9 pages2018 Article 1076FandaruzzahraPutriPerdaniNo ratings yet
- Penelitian Food DiversityDocument9 pagesPenelitian Food DiversityRatna PermatarafaNo ratings yet
- Neonatalnutrition: Scott C. DenneDocument12 pagesNeonatalnutrition: Scott C. DenneSugiantoNo ratings yet
- MenyusuiDocument15 pagesMenyusuiIsna WatiNo ratings yet
- Wong 2014Document10 pagesWong 2014eka wahyuni wahyuniNo ratings yet
- Ijpedi2021 5005365Document8 pagesIjpedi2021 5005365KimberlyjoycsolomonNo ratings yet
- Preventing Stunting in ChildrenDocument4 pagesPreventing Stunting in Childrenadkhiatul muslihatinNo ratings yet
- Barrier and Facilitator On Breastfeeding Education and Promotion: A Literature ReviewDocument7 pagesBarrier and Facilitator On Breastfeeding Education and Promotion: A Literature ReviewIJPHSNo ratings yet
- RESEARCH093016Document28 pagesRESEARCH093016Satra Sabbuh100% (1)
- 6.sick Child Feeding Practice and Associated Factors Among Mothers of Children Less Than 24 Months Old, in Burayu Tow, EthiopiaDocument8 pages6.sick Child Feeding Practice and Associated Factors Among Mothers of Children Less Than 24 Months Old, in Burayu Tow, EthiopiaTomas YeheisNo ratings yet
- Nutrients 15 03395Document4 pagesNutrients 15 03395tomniucNo ratings yet
- Healthy Eating and Obesity Prevention For Preschoolers: A Randomised Controlled TrialDocument9 pagesHealthy Eating and Obesity Prevention For Preschoolers: A Randomised Controlled TrialRiftiani NurlailiNo ratings yet
- The Effectiveness of Community-Based Nutrition Education On The Nutrition Status of Under-Five Children in Developing Countries. A Systematic ReviewDocument4 pagesThe Effectiveness of Community-Based Nutrition Education On The Nutrition Status of Under-Five Children in Developing Countries. A Systematic ReviewDesy rianitaNo ratings yet
- American Academy of Pediatrics: Healthy People 2010, Ing, Breastfeeding in The United States: A National AgendaDocument13 pagesAmerican Academy of Pediatrics: Healthy People 2010, Ing, Breastfeeding in The United States: A National AgendaAntoine SchallerNo ratings yet
- Factors Associated Early Termination of Exclusive Breastfeeding Among Infants Under Six MonthsDocument9 pagesFactors Associated Early Termination of Exclusive Breastfeeding Among Infants Under Six MonthsAmedo Hajji MohamedNo ratings yet
- Assessment of Maternal Knowledge, Attitudes, and Practices Regarding Breastfeeding at Kampala International Teaching Hospital A Study Spanning May 2021 To July 2022Document15 pagesAssessment of Maternal Knowledge, Attitudes, and Practices Regarding Breastfeeding at Kampala International Teaching Hospital A Study Spanning May 2021 To July 2022KIU PUBLICATION AND EXTENSIONNo ratings yet
- 543-Original Article-3692-1-10-20211219 - TerbitDocument11 pages543-Original Article-3692-1-10-20211219 - TerbitAtik PramestiNo ratings yet
- 1 s2.0 S2667268522000092 MainDocument13 pages1 s2.0 S2667268522000092 MainveraNo ratings yet
- Notes On Exclusive BreastfeedingDocument6 pagesNotes On Exclusive BreastfeedingNdem BasseyNo ratings yet
- Journal of Nutrition & Food SciencesDocument6 pagesJournal of Nutrition & Food Sciencesfred opinionNo ratings yet
- Jurnal Vol 1 No 1Document58 pagesJurnal Vol 1 No 1bodiwenNo ratings yet
- Prevalence and Determinant of Exclusive Breastfeeding Among Adolescent MotherDocument8 pagesPrevalence and Determinant of Exclusive Breastfeeding Among Adolescent MothermaulidaNo ratings yet
- Jurnal 2 PDFDocument17 pagesJurnal 2 PDFyayu yuliantiNo ratings yet
- Stunting Policy Brief: WHA Global Nutrition Targets 2025Document10 pagesStunting Policy Brief: WHA Global Nutrition Targets 2025Vania Petrina CalistaNo ratings yet
- Introduction Chapter I: 1.1 BackgroundDocument9 pagesIntroduction Chapter I: 1.1 BackgroundOsob MohamudNo ratings yet
- Childhood Obesity: Causes, Consequences and Prevention ApproachesFrom EverandChildhood Obesity: Causes, Consequences and Prevention ApproachesNo ratings yet
- The Feeding Practices and Structure Questionnaire: Construction and Initial Validation in A Sample of Australian First-Time Mothers and Their 2-Year OldsDocument14 pagesThe Feeding Practices and Structure Questionnaire: Construction and Initial Validation in A Sample of Australian First-Time Mothers and Their 2-Year OldsSanket TelangNo ratings yet
- Pone 0230978Document20 pagesPone 0230978Sanket TelangNo ratings yet
- GTDocument26 pagesGTKhunsa JunaidNo ratings yet
- Mrs.G. Prameela, Prof.A.PadmajaDocument9 pagesMrs.G. Prameela, Prof.A.PadmajaSanket TelangNo ratings yet
- Assessment of The Nutritional Status of Bottle-FedDocument7 pagesAssessment of The Nutritional Status of Bottle-FedSanket TelangNo ratings yet
- Efficiency of Breastfeeding As Compared To BottleDocument9 pagesEfficiency of Breastfeeding As Compared To BottleSanket TelangNo ratings yet
- KAB Baseline FeedingQuestionnaire04July07Document7 pagesKAB Baseline FeedingQuestionnaire04July07Sanket TelangNo ratings yet
- Factors influencing high-SES mothers' infant feeding choicesDocument8 pagesFactors influencing high-SES mothers' infant feeding choicesSanket TelangNo ratings yet
- Placenta Previa: Causes, Symptoms and TreatmentDocument9 pagesPlacenta Previa: Causes, Symptoms and TreatmentSanket TelangNo ratings yet
- Abruptio Placentae Nursing Care & ManagementDocument10 pagesAbruptio Placentae Nursing Care & ManagementSanket TelangNo ratings yet
- Efficiency of Breastfeeding As Compared To BottleDocument9 pagesEfficiency of Breastfeeding As Compared To BottleSanket TelangNo ratings yet
- Wardmanagement Peditric WardDocument19 pagesWardmanagement Peditric WardSanket TelangNo ratings yet
- CopfrontDocument1 pageCopfrontSanket TelangNo ratings yet
- (A Depinttom: Public HeDocument4 pages(A Depinttom: Public HeSanket TelangNo ratings yet
- Oertay: PathogevleaisDocument5 pagesOertay: PathogevleaisSanket TelangNo ratings yet
- Neko 3 Z 1573311312Document180 pagesNeko 3 Z 1573311312Sanket TelangNo ratings yet
- Management SyllabusDocument13 pagesManagement SyllabussandhyakrishnanNo ratings yet
- Adobe Scan 03 Dec 2020Document1 pageAdobe Scan 03 Dec 2020Sanket TelangNo ratings yet
- Viva QuestionsDocument2 pagesViva QuestionsSanket TelangNo ratings yet
- MSN Assignment - HeadacheDocument10 pagesMSN Assignment - HeadacheSanket TelangNo ratings yet
- Aniket 1723Document1 pageAniket 1723Sanket TelangNo ratings yet
- Care of Patient With ECTDocument1 pageCare of Patient With ECTSanket TelangNo ratings yet
- Budgeting Basics: Definition, Types, StepsDocument5 pagesBudgeting Basics: Definition, Types, StepsSanket TelangNo ratings yet
- Grounded Theory - WikipediaDocument103 pagesGrounded Theory - WikipediaSanket TelangNo ratings yet
- 2023 Bermuda School Sports Federation Middle School Cross Country ChampionshipsDocument3 pages2023 Bermuda School Sports Federation Middle School Cross Country ChampionshipsBernewsAdminNo ratings yet
- Paper Analysis Bsa Summer 2019Document3 pagesPaper Analysis Bsa Summer 2019Ronalie SustuedoNo ratings yet
- TGCA MATH6185036 CalculusandScientificComputing-QuestionDocument16 pagesTGCA MATH6185036 CalculusandScientificComputing-QuestionStefanus Frans SebastianNo ratings yet
- Course-Transfer MonashDocument3 pagesCourse-Transfer MonashCheeZhen KongNo ratings yet
- Mother Tongue As Medium of Instruction in LambadaDocument2 pagesMother Tongue As Medium of Instruction in LambadaGuguloth Arjun NaikNo ratings yet
- GRADE 1 To 12 Daily Lesson Plan SCHOOL Cabayabasan Elem. School Grade Level Four TEACHER Florante C. Alconcel Quarter Subject Date 6Document8 pagesGRADE 1 To 12 Daily Lesson Plan SCHOOL Cabayabasan Elem. School Grade Level Four TEACHER Florante C. Alconcel Quarter Subject Date 6Karmela VeluzNo ratings yet
- Zimara Mem 645 Lesson 1 and 2Document9 pagesZimara Mem 645 Lesson 1 and 2Rose Ann ZimaraNo ratings yet
- LRS-5 Scores Should Never Influence RetentionDocument1 pageLRS-5 Scores Should Never Influence RetentionDanielle PerjatelNo ratings yet
- Lesson Plan Best VersionDocument13 pagesLesson Plan Best Versionapi-350625811No ratings yet
- Factors Affecting Implementation of CPD in Ethiopian SchoolsDocument75 pagesFactors Affecting Implementation of CPD in Ethiopian SchoolsMatusala BezuNo ratings yet
- Ois NC Cbse ST 1 2 Ev 5Document1 pageOis NC Cbse ST 1 2 Ev 5api-290841998No ratings yet
- PROFESSIONAL EDUCATION SECONDARY SEPTEMBER 2015Document33 pagesPROFESSIONAL EDUCATION SECONDARY SEPTEMBER 2015Briarose Dela CruzNo ratings yet
- Research 7-q3-w1Document8 pagesResearch 7-q3-w1CARMELA LOLONGNo ratings yet
- 2 Lesson Plan BonesDocument4 pages2 Lesson Plan Bonesapi-311797972No ratings yet
- 8 SGC MOV Quarterly Progress Report BBHSDocument4 pages8 SGC MOV Quarterly Progress Report BBHSJiryl AlpuertoNo ratings yet
- Chapter 1Document11 pagesChapter 1Lyn Garcia100% (2)
- Focus 2 2E Students Book With Answers PDF - SECOND EDITION A2+B TEACHER'S BOOK VOCABULARY - StudocuDocument1 pageFocus 2 2E Students Book With Answers PDF - SECOND EDITION A2+B TEACHER'S BOOK VOCABULARY - Studocuxbxdgssmx8No ratings yet
- Education As Factor of Social ChangeDocument2 pagesEducation As Factor of Social Changelaljoel100% (4)
- MDM 4U1 - Culminating Project (Part 1)Document5 pagesMDM 4U1 - Culminating Project (Part 1)Tiffany ChangNo ratings yet
- Pengganti Sistem AperentisDocument42 pagesPengganti Sistem AperentisNur SyafiqahNo ratings yet
- English Lesson Log for Grade 9Document2 pagesEnglish Lesson Log for Grade 9Ellen Mae MalugaNo ratings yet
- UT Dallas Syllabus For Psy3393.003.09f Taught by Dana Roark (Danar)Document8 pagesUT Dallas Syllabus For Psy3393.003.09f Taught by Dana Roark (Danar)UT Dallas Provost's Technology GroupNo ratings yet
- Chaordic Design Process Notes and Narrative - FreeDocument42 pagesChaordic Design Process Notes and Narrative - FreeSimoneNo ratings yet