You might also like
- Invisible Hands The Businessmen's Crusade Against The New Deal by Kim Phillips-FeinDocument349 pagesInvisible Hands The Businessmen's Crusade Against The New Deal by Kim Phillips-Feinfr33bookspleaseNo ratings yet
- BS 6093: 1993 - Design of Joints and Jointing in Building ConstructionDocument49 pagesBS 6093: 1993 - Design of Joints and Jointing in Building Constructionsathiyan83% (6)
- BSI Training and TroubleshootingDocument45 pagesBSI Training and TroubleshootingSiraj Bendre100% (2)
- Project 2 Ms SQL Dev PDFDocument3 pagesProject 2 Ms SQL Dev PDFNidhi Bansal100% (1)
- Bank and NBFCDocument21 pagesBank and NBFCManika AggarwalNo ratings yet
- Post Acute Coronavirus (COVID-19) Syndrome - StatPearls - NCBI BookshelfDocument13 pagesPost Acute Coronavirus (COVID-19) Syndrome - StatPearls - NCBI BookshelfThành Tài TrầnNo ratings yet
- MAY 2020 SINTOMAS Gastrointestinal Symptoms Associated WithDocument14 pagesMAY 2020 SINTOMAS Gastrointestinal Symptoms Associated WithMayaraNo ratings yet
- Post-COVID Syndrome Incidence, Clinical SpectrumDocument7 pagesPost-COVID Syndrome Incidence, Clinical SpectrumJeane ClaudiaNo ratings yet
- Aspectos Autonómicos Post CovidDocument7 pagesAspectos Autonómicos Post Covidtavo570No ratings yet
- Type 1 Diabetes Triggered by Covid-19 Pandemic A Potential OutbreakDocument3 pagesType 1 Diabetes Triggered by Covid-19 Pandemic A Potential OutbreaksamuelNo ratings yet
- Zhou2020 Article CoronavirusDisease2019COVID-19 PDFDocument10 pagesZhou2020 Article CoronavirusDisease2019COVID-19 PDFElena AlexandraNo ratings yet
- Koc 2022Document14 pagesKoc 2022John GoranitisNo ratings yet
- Sars-Cov-2 and The Brain: What Do We Know About The Causality of Cognitive Covid?Document14 pagesSars-Cov-2 and The Brain: What Do We Know About The Causality of Cognitive Covid?Carlos Eduardo NorteNo ratings yet
- Long Covid 1Document5 pagesLong Covid 1lakshminivas PingaliNo ratings yet
- The Challenge of Long COVID-19 Management From DisDocument18 pagesThe Challenge of Long COVID-19 Management From Disaede747No ratings yet
- Long Term Complications and Rehabilitation of COVID-19 PatientsDocument5 pagesLong Term Complications and Rehabilitation of COVID-19 Patientsmathias kosasihNo ratings yet
- 2020 June JOI COVID-19 As An Acute Inflammatory DiseaseDocument9 pages2020 June JOI COVID-19 As An Acute Inflammatory DiseaseOctavio GamezNo ratings yet
- Cellular and Molecular ImmunologyDocument21 pagesCellular and Molecular ImmunologyMUGDHA MITTALNo ratings yet
- COVID-19 Screening Prognosis and Severity Assessment With Biomarkers HORIBA MedicalDocument14 pagesCOVID-19 Screening Prognosis and Severity Assessment With Biomarkers HORIBA MedicalIrkania PasangkaNo ratings yet
- Bio Investigatory ProjectDocument23 pagesBio Investigatory ProjectPARTHA PRATIM KARNo ratings yet
- The Neurological Manifestations of COVID-19 - NEUROL SCI 2020Document5 pagesThe Neurological Manifestations of COVID-19 - NEUROL SCI 2020Nicole Ferreira PiccoliNo ratings yet
- Main PDFDocument4 pagesMain PDFRSDC Tower 5No ratings yet
- Systemic Involvement of Novel Coronavirus (COVID-19) : A Review of LiteratureDocument5 pagesSystemic Involvement of Novel Coronavirus (COVID-19) : A Review of LiteratureASHIQNo ratings yet
- Case-Control Study of Patient Characteristics, Knowledge of The COVID-19 Disease, Risk Behaviour and Mental State in Patients Visiting An Emergency Room With COVID-19 Symptoms in The NetherlandsDocument13 pagesCase-Control Study of Patient Characteristics, Knowledge of The COVID-19 Disease, Risk Behaviour and Mental State in Patients Visiting An Emergency Room With COVID-19 Symptoms in The NetherlandsRevi RidayantiNo ratings yet
- Vaccine 2021Document17 pagesVaccine 2021cdsaludNo ratings yet
- Can Nanotechnology Help in The Fight Against COVID 19Document17 pagesCan Nanotechnology Help in The Fight Against COVID 19Kishore PaknikarNo ratings yet
- Reviewer Report Covid-19Document11 pagesReviewer Report Covid-19adelaidah sanggacalaNo ratings yet
- Ijerph 19 12422 v4Document12 pagesIjerph 19 12422 v4Thairon HenriqueNo ratings yet
- A Clinic Blueprint For Post-Coronavirus Disease 2019 RECOVERY Learning From The Past, Looking To The FutureDocument11 pagesA Clinic Blueprint For Post-Coronavirus Disease 2019 RECOVERY Learning From The Past, Looking To The FutureCARLA CRISTINA DE ARAUJONo ratings yet
- COVID-19: Pathophysiology of Acute Disease 1: SeriesDocument21 pagesCOVID-19: Pathophysiology of Acute Disease 1: SeriesMyatnoe KhinNo ratings yet
- Clinical Immunology: Review ArticleDocument9 pagesClinical Immunology: Review ArticleSimon Peter SiansakaNo ratings yet
- Emptech Ponferrada 1Document7 pagesEmptech Ponferrada 1Fiel Anthony PonferradaNo ratings yet
- International Immunopharmacology: Mohammad Shah Alam, Daniel M. Czajkowsky, Md. Aminul Islam, Md. Ataur RahmanDocument12 pagesInternational Immunopharmacology: Mohammad Shah Alam, Daniel M. Czajkowsky, Md. Aminul Islam, Md. Ataur RahmanJimena Vásquez RodríguezNo ratings yet
- Immunological Reviews - 2021 - John - COVID 19 and Pulmonary Fibrosis A Potential Role For Lung Epithelial Cells andDocument13 pagesImmunological Reviews - 2021 - John - COVID 19 and Pulmonary Fibrosis A Potential Role For Lung Epithelial Cells andemmanuel AndemNo ratings yet
- Covid-19: Icu Delirium Management During Sars-Cov-2 PandemicDocument10 pagesCovid-19: Icu Delirium Management During Sars-Cov-2 PandemicFadhilahNo ratings yet
- Novel Coronavirus 2019 (2019-Ncov) Infection: Part Ii - Respiratory Support in The Pediatric Intensive Care Unit in Resource-Limited SettingsDocument8 pagesNovel Coronavirus 2019 (2019-Ncov) Infection: Part Ii - Respiratory Support in The Pediatric Intensive Care Unit in Resource-Limited Settingsdiah Bayu siswantiNo ratings yet
- Diagnosis of Sars-Cov-2 Infection in The Setting of The Cytokine Release SyndromeDocument12 pagesDiagnosis of Sars-Cov-2 Infection in The Setting of The Cytokine Release SyndromeTufik NaderNo ratings yet
- Joim 13091Document15 pagesJoim 13091sarabisimonaNo ratings yet
- COVID-19 - Diagnosis - UpToDateDocument34 pagesCOVID-19 - Diagnosis - UpToDateDuy Hùng HoàngNo ratings yet
- The Severity of The Co-Infection of Mycoplasma Pneumoniae in COVID-19 PatientsDocument7 pagesThe Severity of The Co-Infection of Mycoplasma Pneumoniae in COVID-19 Patientsemmanuel AndemNo ratings yet
- Journal of Internal Medicine - 2020 - Pascarella - COVID 19 Diagnosis and Management A Comprehensive ReviewDocument15 pagesJournal of Internal Medicine - 2020 - Pascarella - COVID 19 Diagnosis and Management A Comprehensive ReviewOscar Oswaldo SCNo ratings yet
- Post COVID-19 Coplications During PandemicDocument4 pagesPost COVID-19 Coplications During PandemicInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Biomedicines 10 01952 v2Document13 pagesBiomedicines 10 01952 v2carmen rosa secce pedrazaNo ratings yet
- COVID-19 Vaccines To Prevent SARS-CoV-2 Infection - UpToDateDocument86 pagesCOVID-19 Vaccines To Prevent SARS-CoV-2 Infection - UpToDateXochilt Mejia GarciaNo ratings yet
- COVID 19 and Hemodialysis Anxiety: Letter To EditorDocument2 pagesCOVID 19 and Hemodialysis Anxiety: Letter To EditorBastian AgungNo ratings yet
- An Update On COVID 19 Pandemic The Epidemiology Pathogenesis Prevention and Treatment Strategies (Important)Document13 pagesAn Update On COVID 19 Pandemic The Epidemiology Pathogenesis Prevention and Treatment Strategies (Important)ayoubNo ratings yet
- Novel CoronavirusDocument7 pagesNovel CoronavirusMustafa KhudhairNo ratings yet
- Long-COVID: An Evolving Problem With An Extensive Impact: Clinical UpdateDocument3 pagesLong-COVID: An Evolving Problem With An Extensive Impact: Clinical UpdateArif wicaksonoNo ratings yet
- Nutrients: COVID-19: The Inflammation Link and The Role of Nutrition in Potential MitigationDocument28 pagesNutrients: COVID-19: The Inflammation Link and The Role of Nutrition in Potential MitigationNoviaNo ratings yet
- Corona Virus 2019Document11 pagesCorona Virus 2019Jonille EchevarriaNo ratings yet
- COVID-19 and Tuberculosis: HighlightDocument7 pagesCOVID-19 and Tuberculosis: HighlightMariaNo ratings yet
- Mesenchymal Stem Cell Immunomodulation and Regeneration TherapeuticsDocument13 pagesMesenchymal Stem Cell Immunomodulation and Regeneration TherapeuticswiwiNo ratings yet
- Abstract VaccinesDocument13 pagesAbstract VaccinesmartinscodellerNo ratings yet
- Life Sciences: Rishabh Hirawat, Mohd Aslam Saifi, Chandraiah GoduguDocument14 pagesLife Sciences: Rishabh Hirawat, Mohd Aslam Saifi, Chandraiah GoduguPaoloMafaldoNo ratings yet
- Clinical Outcomes and Immunologic Characteristics of Coronavirus Disease 2019 in People With Human Immunodeficiency VirusDocument6 pagesClinical Outcomes and Immunologic Characteristics of Coronavirus Disease 2019 in People With Human Immunodeficiency VirusanaNo ratings yet
- Journal - SARS in Geriatric - AlbertoDocument5 pagesJournal - SARS in Geriatric - AlbertoalbertoNo ratings yet
- Research Paper 2 ReviewDocument6 pagesResearch Paper 2 ReviewThe Code RunNo ratings yet
- BernasDocument17 pagesBernasYezekael Sebastian QuintinusNo ratings yet
- Corona Virus DiseaseDocument6 pagesCorona Virus DiseaseSAKET MEHTANo ratings yet
- In Late 2019Document5 pagesIn Late 2019GrayNo ratings yet
- Fadiga Crônica Pós-CovidDocument12 pagesFadiga Crônica Pós-CovidJuliana VieiraNo ratings yet
- Diabetes Mellitus in The Context of COVID-19 La Diabetes Mellitus en El Contexto de La COVID-19Document8 pagesDiabetes Mellitus in The Context of COVID-19 La Diabetes Mellitus en El Contexto de La COVID-19Tatiana Belén García MogollónNo ratings yet
- The Epidemiology and Pathogenesis of Coronavirus Disease (COVID-19) OutbreakDocument16 pagesThe Epidemiology and Pathogenesis of Coronavirus Disease (COVID-19) Outbreaksunitha pNo ratings yet
- COVID Diabetes 2Document5 pagesCOVID Diabetes 2htapiamNo ratings yet
- Facing COVID-19 with the benefits of medical cannabisFrom EverandFacing COVID-19 with the benefits of medical cannabisNo ratings yet
- A Study On Utilisation of EEG and Patient Satisfaction in The Neurology Department.Document97 pagesA Study On Utilisation of EEG and Patient Satisfaction in The Neurology Department.pmanojaswinNo ratings yet
- Air of Fredoom - Infinity History of Corruption in BoliviaDocument315 pagesAir of Fredoom - Infinity History of Corruption in BoliviaParavicoNo ratings yet
- Zirconium in The Nuclear IndustryDocument680 pagesZirconium in The Nuclear IndustryWeb devNo ratings yet
- Cable Construction & Cable Selection - Part - 1 - Electrical Notes & ArticlesDocument7 pagesCable Construction & Cable Selection - Part - 1 - Electrical Notes & Articlesscyper89100% (1)
- Insurance Regulatory and Development ActDocument13 pagesInsurance Regulatory and Development ActSai VasudevanNo ratings yet
- Wicked Women - Women & Pre-Code HollywoodDocument6 pagesWicked Women - Women & Pre-Code HollywoodNickyNo ratings yet
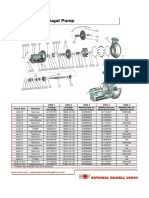
- Mission Magnum I Pump Spare PartsDocument2 pagesMission Magnum I Pump Spare PartsEleazar GallegosNo ratings yet
- Bharat Petroleum Corporation LimitedDocument10 pagesBharat Petroleum Corporation LimitedAshutoshNo ratings yet
- Entrepreneurship SchemesDocument6 pagesEntrepreneurship SchemesSADENT2100% (1)
- Fruit The Art of Pastry PDFDocument1 pageFruit The Art of Pastry PDF5kyx24kzd4No ratings yet
- Maulana Azad National Institute of Technology, BhopalDocument2 pagesMaulana Azad National Institute of Technology, BhopalNiteshNarukaNo ratings yet
- 40 LINQ MethodsDocument12 pages40 LINQ MethodsMustafa GençNo ratings yet
- Ejercicios Cap2 PHDocument7 pagesEjercicios Cap2 PHpolk96No ratings yet
- Hyundai Led4 InstruccionesDocument5 pagesHyundai Led4 InstruccionesEncep ZaenalNo ratings yet
- Comparison Between Old & New Insurance CodeDocument2 pagesComparison Between Old & New Insurance CodemherinrodriguezNo ratings yet
- Health Economics 1St Edition Bhattacharya Solutions Manual Full Chapter PDFDocument36 pagesHealth Economics 1St Edition Bhattacharya Solutions Manual Full Chapter PDFjames.williams932100% (15)
- Different Options That Can Be Used With Sapinst Command LineDocument5 pagesDifferent Options That Can Be Used With Sapinst Command Linesai_balaji_8No ratings yet
- Sample Independent Contractor AgreementDocument5 pagesSample Independent Contractor AgreementRodolfo moo DzulNo ratings yet
- Groovy Tutorial PDFDocument35 pagesGroovy Tutorial PDFPratishta TambeNo ratings yet
- Managerial Accounting 09Document68 pagesManagerial Accounting 09Dheeraj Suntha100% (1)
- Health Promotion UnitDocument121 pagesHealth Promotion UnitsolacespunkyNo ratings yet
- Cryogenic Reactor Cooling Spec SheetDocument2 pagesCryogenic Reactor Cooling Spec SheetLibinNo ratings yet
- Lecture 1 - Information Systems Auditing Overview and MethodologiesDocument65 pagesLecture 1 - Information Systems Auditing Overview and MethodologieskamuturiNo ratings yet
- World SeriesDocument106 pagesWorld SeriesanonymousNo ratings yet
- Audit of Inventories and Cost of Goods SDocument10 pagesAudit of Inventories and Cost of Goods SJessaNo ratings yet