You might also like
- Hunger: Mentalization-based Treatments for Eating DisordersFrom EverandHunger: Mentalization-based Treatments for Eating DisordersRating: 1 out of 5 stars1/5 (1)
- Cusi 2010Document5 pagesCusi 2010Πέγκυ ΠρεσβέλουNo ratings yet
- 10 1016@j Jad 2014 10 055Document8 pages10 1016@j Jad 2014 10 055Diana ParraNo ratings yet
- Social Anxiety and Social CognitionDocument14 pagesSocial Anxiety and Social CognitionDaniela Alvarez ForeroNo ratings yet
- Mental HealthDocument16 pagesMental HealthYessa CaesarNo ratings yet
- 1 s2.0 S0165178122003468 MainDocument11 pages1 s2.0 S0165178122003468 MainDaniela Alvarez ForeroNo ratings yet
- Cole2018 Article AbilitiesToExplicitlyAndImplicDocument15 pagesCole2018 Article AbilitiesToExplicitlyAndImplicenrique.navaNo ratings yet
- Psychiatry Research: Felice Loi, Jatin G. Vaidya, Sergio ParadisoDocument10 pagesPsychiatry Research: Felice Loi, Jatin G. Vaidya, Sergio ParadisoCaduRodriguesNo ratings yet
- Meta-Analysis of The Moral Brain: Patterns of Neural Engagement Assessed Using Multilevel Kernel Density AnalysisDocument14 pagesMeta-Analysis of The Moral Brain: Patterns of Neural Engagement Assessed Using Multilevel Kernel Density Analysissucca07No ratings yet
- XVFDocument16 pagesXVFJoaquín OlivaresNo ratings yet
- Bell 2010Document8 pagesBell 2010RosarioBengocheaSecoNo ratings yet
- NIH Public Access: Author ManuscriptDocument17 pagesNIH Public Access: Author ManuscriptRosarioBengocheaSecoNo ratings yet
- Neural Bases of Antisocial Behavior: A Voxel-Based Meta-AnalysisDocument9 pagesNeural Bases of Antisocial Behavior: A Voxel-Based Meta-AnalysisYeremias EdwinNo ratings yet
- Comportamiento SuicidaDocument15 pagesComportamiento SuicidaFregoso Robledo Amayrani EstefaniaNo ratings yet
- Brewer2022 Article AQuickMeasureOfTheoryOfMindInADocument18 pagesBrewer2022 Article AQuickMeasureOfTheoryOfMindInAFlori MNo ratings yet
- kalket and wilson-milestone 3 literature review-Document13 pageskalket and wilson-milestone 3 literature review-api-704711481No ratings yet
- 1 SchizoneurocognsocialcognDocument7 pages1 SchizoneurocognsocialcognAguelito AlbertNo ratings yet
- Aregentinian Version of IHS Del PretteDocument11 pagesAregentinian Version of IHS Del PretteNicole TroncosoNo ratings yet
- A Developmental Mentalization-Based Approach To THDocument28 pagesA Developmental Mentalization-Based Approach To THcristina campoy lacasaNo ratings yet
- I. Background/Objectives and GoalsDocument2 pagesI. Background/Objectives and GoalsJilmilyn MolenoNo ratings yet
- Nihms 375958Document67 pagesNihms 375958Alexandra Ioana MiclausNo ratings yet
- Cognitive Difficulties Scale CDS - Psychometric PropertiesDocument14 pagesCognitive Difficulties Scale CDS - Psychometric PropertiesRafael MartinsNo ratings yet
- Defning and Measuring Indices of Happiness and Unhappiness in Children Diagnosed With Autism Spectrum DisorderDocument17 pagesDefning and Measuring Indices of Happiness and Unhappiness in Children Diagnosed With Autism Spectrum DisorderVini PezzinNo ratings yet
- TOM and SADDocument3 pagesTOM and SADLENIN JEAN MARTIN BENDEZU ZARATENo ratings yet
- Theory of mind, empathy and moral emotions in patients with affective disordersDocument8 pagesTheory of mind, empathy and moral emotions in patients with affective disordersTasos TravasarosNo ratings yet
- Specific Learning Disorders in Young Adults Investigating Pramactic Abilities and Their Relationship With Theory o MindDocument10 pagesSpecific Learning Disorders in Young Adults Investigating Pramactic Abilities and Their Relationship With Theory o MindGisella BonillaNo ratings yet
- Lack of Emotional Gaze Preferences Using Eye-Tracking in Remitted Bipolar I DisorderDocument10 pagesLack of Emotional Gaze Preferences Using Eye-Tracking in Remitted Bipolar I DisorderfahmilNo ratings yet
- Affective and cognitive theory of mind abilities inDocument32 pagesAffective and cognitive theory of mind abilities inSophieBerrettaNo ratings yet
- Personality and Individual Differences: M . Inmaculada L Opez-Nú Nez, Juan F. Díaz-Morales, Marta E. Aparicio-GarcíaDocument6 pagesPersonality and Individual Differences: M . Inmaculada L Opez-Nú Nez, Juan F. Díaz-Morales, Marta E. Aparicio-Garcíacute dollNo ratings yet
- The Contributions of Attachment Styles, Irrational Beliefs and Psychological Symptoms To The Prediction of Cognitive FlexibilityDocument8 pagesThe Contributions of Attachment Styles, Irrational Beliefs and Psychological Symptoms To The Prediction of Cognitive FlexibilityAlex de LisNo ratings yet
- Good Things Better, Reappraisal and Discrete EmotionsDocument30 pagesGood Things Better, Reappraisal and Discrete EmotionsÁngel CamachoNo ratings yet
- Kenworthy Et Al. - 2014 - Randomized Controlled Effectiveness Trial of Execu PDFDocument19 pagesKenworthy Et Al. - 2014 - Randomized Controlled Effectiveness Trial of Execu PDFJeune WillNo ratings yet
- Journal of Behavior Therapy and Experimental Psychiatry: Kristine Kahr NilssonDocument5 pagesJournal of Behavior Therapy and Experimental Psychiatry: Kristine Kahr NilssonlucianaeuNo ratings yet
- Social Cognition in Paediatric Traumatic Brain Injury: A Systematic Review and Meta AnalysisDocument22 pagesSocial Cognition in Paediatric Traumatic Brain Injury: A Systematic Review and Meta Analysisgeorgia santosNo ratings yet
- Conway 08 Integrating Anxiety SNDocument8 pagesConway 08 Integrating Anxiety SNGeorge BaciuNo ratings yet
- Achim 2012 PR (MTZ-FEP)Document7 pagesAchim 2012 PR (MTZ-FEP)richard LemieuxNo ratings yet
- 1 s2.0 S2212144718301066 MainDocument11 pages1 s2.0 S2212144718301066 MainAdriana fernandesNo ratings yet
- Guimond 2021Document9 pagesGuimond 2021Diego Librenza GarciaNo ratings yet
- Boada2020 Article SocialCognitionInAutismAndSchiDocument14 pagesBoada2020 Article SocialCognitionInAutismAndSchiSara BenitoNo ratings yet
- A Developmental Mentalization Based Approach To The Understanding and Treatment of Borderline Personality DisorderDocument27 pagesA Developmental Mentalization Based Approach To The Understanding and Treatment of Borderline Personality Disordertatiana martinezNo ratings yet
- Zdravlja I Nega Za ZenuDocument14 pagesZdravlja I Nega Za ZenuRita LorikaNo ratings yet
- Practical 2 UdpdDocument11 pagesPractical 2 Udpdidonttttknowww1234567890No ratings yet
- TCE Cognición Social en Niños REVISION SISTEMATICA Y METAANALISISDocument22 pagesTCE Cognición Social en Niños REVISION SISTEMATICA Y METAANALISISmaría del pinoNo ratings yet
- Lecce 2015Document7 pagesLecce 2015Isaac Daniel Carrero RoseroNo ratings yet
- Emotional Intelligence and Its Relation With Hedonic and Eudaimonic Well-Being: A Prospective StudyDocument6 pagesEmotional Intelligence and Its Relation With Hedonic and Eudaimonic Well-Being: A Prospective StudyJoBPNo ratings yet
- Pujals 2015Document6 pagesPujals 2015Arturo GaytánNo ratings yet
- Pineda 2009Document9 pagesPineda 2009yma ymiiNo ratings yet
- 2006 Improved Quality of Life and Cognitive Stimulation Therapy in DementiaDocument9 pages2006 Improved Quality of Life and Cognitive Stimulation Therapy in DementiaAndreaSantosNo ratings yet
- Vandevelde Morisse Et Al IJDD 2014 - SED-R-with-cover-page-v2Document14 pagesVandevelde Morisse Et Al IJDD 2014 - SED-R-with-cover-page-v2Martina GuzmanNo ratings yet
- Lloyd Et Al 2021 Brain ImpairmentDocument21 pagesLloyd Et Al 2021 Brain ImpairmentBeth LloydNo ratings yet
- s43076-022-00145-yDocument26 pagess43076-022-00145-yedgardo.etchezaharNo ratings yet
- Cap 2015 0100Document9 pagesCap 2015 0100Rafael MartinsNo ratings yet
- Killian 2011Document13 pagesKillian 2011Luna MoonNo ratings yet
- TMP DE4 DDocument11 pagesTMP DE4 DFrontiersNo ratings yet
- A DevelopmentalDocument27 pagesA DevelopmentalElena AlonsoNo ratings yet
- Ibanez 2013Document30 pagesIbanez 2013LUIS FELIPE CHAGAS CALDEIRA CATAONo ratings yet
- The Missinig LinkDocument16 pagesThe Missinig LinkAleix Armengol SánchezNo ratings yet
- Enanpad Kovik5zb Why We Imagine Our Future Introducing The Functions of 4yk8uf4bqaDocument34 pagesEnanpad Kovik5zb Why We Imagine Our Future Introducing The Functions of 4yk8uf4bqaMéroli Saccardo dos SantosNo ratings yet
- 02bfe50d98359a7de3000000 PDFDocument6 pages02bfe50d98359a7de3000000 PDFomkarenatorNo ratings yet
- Exploring The Role of Age As A Moderator of Cognitive Remediation SchizophreniaDocument7 pagesExploring The Role of Age As A Moderator of Cognitive Remediation SchizophreniammimcNo ratings yet
- 2015 - Head-to-Head Comparison of The Neuropsychiatric Effect of Dopamine Agonists in Parkinson's Disease - A Prospective, Cross-Sectional Study in Non-Demented PatientsDocument7 pages2015 - Head-to-Head Comparison of The Neuropsychiatric Effect of Dopamine Agonists in Parkinson's Disease - A Prospective, Cross-Sectional Study in Non-Demented PatientsRaúl VerdugoNo ratings yet
- 2014 - Apathy in Parkinson's Disease - Neurophysiological Evidence of Impaired Incentive ProcessingDocument9 pages2014 - Apathy in Parkinson's Disease - Neurophysiological Evidence of Impaired Incentive ProcessingRaúl VerdugoNo ratings yet
- 2011 - Subtypes of Developmental Coordination Disorder - Research On Their Nature and EtiologyDocument31 pages2011 - Subtypes of Developmental Coordination Disorder - Research On Their Nature and EtiologyRaúl VerdugoNo ratings yet
- Huntington NatDocument21 pagesHuntington NatplutopolloNo ratings yet
- 2019 - Evolution of Prodromal Parkinson's Disease and Dementia With Lewy Bodies - A Prospective StudyDocument17 pages2019 - Evolution of Prodromal Parkinson's Disease and Dementia With Lewy Bodies - A Prospective StudyRaúl VerdugoNo ratings yet
- 2020 - Sluggish Cognitive Tempo in Adolescents With and Without ADHD - Differentiation From Adolescent-Reported ADHD Inattention and Unique Associations With Internalizing DomainsDocument16 pages2020 - Sluggish Cognitive Tempo in Adolescents With and Without ADHD - Differentiation From Adolescent-Reported ADHD Inattention and Unique Associations With Internalizing DomainsRaúl VerdugoNo ratings yet
- 2016 - The Representation of Objects in Apraxia - From Action Execution To Error AwarenessDocument14 pages2016 - The Representation of Objects in Apraxia - From Action Execution To Error AwarenessRaúl VerdugoNo ratings yet
- 2016 - Neuropsychiatric Symptoms Are Very Common in Premanifest and Early Stage HDDocument7 pages2016 - Neuropsychiatric Symptoms Are Very Common in Premanifest and Early Stage HDRaúl VerdugoNo ratings yet
- 2019 - Sluggish Cognitive Tempo and Behavioral Difficulties in Children With ADHD - Associations With Internalizing and Externalizing SymptomsDocument8 pages2019 - Sluggish Cognitive Tempo and Behavioral Difficulties in Children With ADHD - Associations With Internalizing and Externalizing SymptomsRaúl VerdugoNo ratings yet
- 2019 - Magnetic Resonance Imaging-Visible Perivascular Spaces in Basal Ganglia Predict Cognitive Decline in Parkinson's DiseaseDocument8 pages2019 - Magnetic Resonance Imaging-Visible Perivascular Spaces in Basal Ganglia Predict Cognitive Decline in Parkinson's DiseaseRaúl VerdugoNo ratings yet
- Abordaje Pedagógico para El TDAHDocument7 pagesAbordaje Pedagógico para El TDAHKatherine Cuadra BravoNo ratings yet
- 2019 - The Relationship Between Cognitive Functions and Sport-Specific Motor Skills in Elite Youth Soccer PlayersDocument10 pages2019 - The Relationship Between Cognitive Functions and Sport-Specific Motor Skills in Elite Youth Soccer PlayersRaúl VerdugoNo ratings yet
- 2019 - Slow Processing Speed and Sluggish Cognitive Tempo in Pediatric Attention Deficit - Hyperactivity Disorder - Evidence For Differentiation of Functional CorrelatesDocument9 pages2019 - Slow Processing Speed and Sluggish Cognitive Tempo in Pediatric Attention Deficit - Hyperactivity Disorder - Evidence For Differentiation of Functional CorrelatesRaúl VerdugoNo ratings yet
- 2016 - Non-Demented Parkinson's Disease Patients With Apathy Show Decreased Grey Matter Volume in Key Executive and Reward-Related NodesDocument9 pages2016 - Non-Demented Parkinson's Disease Patients With Apathy Show Decreased Grey Matter Volume in Key Executive and Reward-Related NodesRaúl VerdugoNo ratings yet
- 2001 - Symptom Properties As A Function of ADHD Type - An Argument For Continued Study of Sluggish Cognitive TempoDocument7 pages2001 - Symptom Properties As A Function of ADHD Type - An Argument For Continued Study of Sluggish Cognitive TempoRaúl VerdugoNo ratings yet
- 2014 - Sluggish Cognitive Tempo and Its Neurocognitive, Social and Emotive Correlates - A Systematic Review of The Current LiteratureDocument13 pages2014 - Sluggish Cognitive Tempo and Its Neurocognitive, Social and Emotive Correlates - A Systematic Review of The Current LiteratureRaúl VerdugoNo ratings yet
- 2013 - Distinguishing Sluggish Cognitive Tempo From ADHD in Children and Adolescents - Executive Functioning, Impairment, and ComorbidityDocument14 pages2013 - Distinguishing Sluggish Cognitive Tempo From ADHD in Children and Adolescents - Executive Functioning, Impairment, and ComorbidityRaúl VerdugoNo ratings yet
- 2019 - The Role of Neuropsychology in The Evaluation of ConcussionDocument13 pages2019 - The Role of Neuropsychology in The Evaluation of ConcussionRaúl VerdugoNo ratings yet
- Learning Style 'Neuromyth'Document3 pagesLearning Style 'Neuromyth'Raúl VerdugoNo ratings yet
- 2012 - Factor Structure of A Sluggish Cognitive Tempo Scale in Clinically-Referred ChildrenDocument11 pages2012 - Factor Structure of A Sluggish Cognitive Tempo Scale in Clinically-Referred ChildrenRaúl VerdugoNo ratings yet
- 2001 - A Dose-Response Relation of Headers and Concussions With Cognitive Impairment in Professional Soccer PlayersDocument7 pages2001 - A Dose-Response Relation of Headers and Concussions With Cognitive Impairment in Professional Soccer PlayersRaúl VerdugoNo ratings yet
- 2017 - Measuring Cognitive Change With ImPACT - The Aggregate Baseline ApproachDocument13 pages2017 - Measuring Cognitive Change With ImPACT - The Aggregate Baseline ApproachRaúl VerdugoNo ratings yet
- 2018 - Studying Brain Activity in Sports Performance - Contributions and IssuesDocument21 pages2018 - Studying Brain Activity in Sports Performance - Contributions and IssuesRaúl VerdugoNo ratings yet
- Attention-Deficit/Hyperactivity Disorder and Sluggish Cognitive Tempo Dimensions in Relation To Executive Functioning in Adolescents With ADHDDocument11 pagesAttention-Deficit/Hyperactivity Disorder and Sluggish Cognitive Tempo Dimensions in Relation To Executive Functioning in Adolescents With ADHDRaúl VerdugoNo ratings yet
- 2016 - Are There Subconcussive Neuropsychological Effects in Youth Sports? An Exploratory Study of High - and Low-Contact SportsDocument8 pages2016 - Are There Subconcussive Neuropsychological Effects in Youth Sports? An Exploratory Study of High - and Low-Contact SportsRaúl VerdugoNo ratings yet
- Immediate Post-Concussion Assessment and Cognitive Testing (ImPACT) Practices of Sports Medicine ProfessionalsDocument6 pagesImmediate Post-Concussion Assessment and Cognitive Testing (ImPACT) Practices of Sports Medicine Professionalsijambrović_1No ratings yet
- 2016 - Applications of Transcranial Direct Current Stimulation in Children and PediatricsDocument12 pages2016 - Applications of Transcranial Direct Current Stimulation in Children and PediatricsRaúl VerdugoNo ratings yet
- 2019 - Anodal TDCS Over Wernicke's Area Improves Verbal Memory and Prevents The Interference Effect During Words LearningDocument12 pages2019 - Anodal TDCS Over Wernicke's Area Improves Verbal Memory and Prevents The Interference Effect During Words LearningRaúl VerdugoNo ratings yet
- 2015 - Two Baselines Are Better Than One - Improving The Reliability of Computerized Testing in Sports NeuropsychologyDocument8 pages2015 - Two Baselines Are Better Than One - Improving The Reliability of Computerized Testing in Sports NeuropsychologyRaúl VerdugoNo ratings yet
- The Brain's Role in Noncontact Anterior Cruciate Ligament InjuriesDocument3 pagesThe Brain's Role in Noncontact Anterior Cruciate Ligament InjuriesRaúl VerdugoNo ratings yet
- Pate, M. B., Evaporators and Condensers For Refrigeration and Air-Conditioning Systems, in Boilers, Evaporators andDocument1 pagePate, M. B., Evaporators and Condensers For Refrigeration and Air-Conditioning Systems, in Boilers, Evaporators andpete pansNo ratings yet
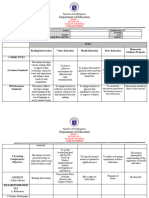
- DLL Catch Up Friday Grade 4 Jan 19Document7 pagesDLL Catch Up Friday Grade 4 Jan 19reyannmolinacruz21100% (30)
- Prince George's County Afro-American Newspaper, January 22, 2011Document16 pagesPrince George's County Afro-American Newspaper, January 22, 2011The AFRO-American NewspapersNo ratings yet
- Standards and Their ClassificationsDocument3 pagesStandards and Their ClassificationsJoecelle AbleginaNo ratings yet
- (Earth and Space Science (Science Readers) ) Greg Young-Alfred Wegener. Uncovering Plate Tectonics-Shell Education - Teacher Created Materials (2008)Document35 pages(Earth and Space Science (Science Readers) ) Greg Young-Alfred Wegener. Uncovering Plate Tectonics-Shell Education - Teacher Created Materials (2008)Peter GonzálezNo ratings yet
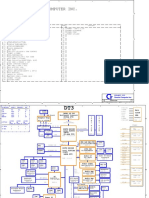
- Acer Aspire 1710 (Quanta DT3) PDFDocument35 pagesAcer Aspire 1710 (Quanta DT3) PDFMustafa AkanNo ratings yet
- Crane Company Within SingaporeDocument4 pagesCrane Company Within SingaporeRash AcidNo ratings yet
- Technical Service Information: Ford/Lincoln/Mercury 6F50NDocument18 pagesTechnical Service Information: Ford/Lincoln/Mercury 6F50NPlanta Damiana2No ratings yet
- Revison 5 - Adverbs of TimeDocument50 pagesRevison 5 - Adverbs of Timeluis fernandoNo ratings yet
- Z22 Double-Suction Axially-Split Single-Stage Centrifugal PumpDocument2 pagesZ22 Double-Suction Axially-Split Single-Stage Centrifugal Pumpmartín_suárez_110% (1)
- Surveyquestionnaire 1Document6 pagesSurveyquestionnaire 1Almira IbarraNo ratings yet
- Design Approval Checklist 2nd Rev.Document3 pagesDesign Approval Checklist 2nd Rev.Daric Tesfaye0% (1)
- Human Persons Are Oriented Toward Their Impending DeathDocument40 pagesHuman Persons Are Oriented Toward Their Impending DeathNaddy Retxed100% (1)
- Assignment 5: Engineering Utilities IiDocument4 pagesAssignment 5: Engineering Utilities IiRex SabersonNo ratings yet
- IdkDocument2 pagesIdkKyle FikaniNo ratings yet
- Casey Cannon: EducationDocument1 pageCasey Cannon: Educationapi-355305449No ratings yet
- Technical Card: Information OnlyDocument1 pageTechnical Card: Information OnlyBhuvnesh VermaNo ratings yet
- Einas Mansour - Curriculum VitaeDocument3 pagesEinas Mansour - Curriculum VitaeEinas MansourNo ratings yet
- Manual Completo Sinovo SD600Document221 pagesManual Completo Sinovo SD600Felipe de PaulaNo ratings yet
- Management Quality ManagementDocument7 pagesManagement Quality ManagementJasmine LimNo ratings yet
- YASHICA MAT-124 User's ManualDocument34 pagesYASHICA MAT-124 User's Manuallegrandew100% (1)
- Cost-Time-Resource Sheet for Rumaila Oil Field Engineering ServicesDocument13 pagesCost-Time-Resource Sheet for Rumaila Oil Field Engineering ServicesonlyikramNo ratings yet
- Ds 311 2 General Pre-Start Check List (B)Document4 pagesDs 311 2 General Pre-Start Check List (B)Miguel RomoNo ratings yet
- Troubleshooting Edge Quality: Mild SteelDocument14 pagesTroubleshooting Edge Quality: Mild SteelAnonymous U6yVe8YYCNo ratings yet
- Did You Ever Meet Shattered Illusions?Document5 pagesDid You Ever Meet Shattered Illusions?Junjie HuangNo ratings yet
- 1.finite Impulse Response (FIR) FiltersDocument16 pages1.finite Impulse Response (FIR) FiltersSamet YılmazNo ratings yet
- Krish Kumar 13 Activity 5 SolutionDocument39 pagesKrish Kumar 13 Activity 5 SolutionkrishNo ratings yet
- Role of Digital Infrastructure in The Post Pandemic World: Preparing For Civil Services Interview-The Right PerspectiveDocument40 pagesRole of Digital Infrastructure in The Post Pandemic World: Preparing For Civil Services Interview-The Right PerspectiveshekhardfcNo ratings yet
- Sub Net Questions With AnsDocument5 pagesSub Net Questions With AnsSavior Wai Hung WongNo ratings yet
- Ddec IV Application and InstallationDocument148 pagesDdec IV Application and Installationsptecnico8292% (36)