You might also like
- Management of Acute Meningitis - PMCDocument1 pageManagement of Acute Meningitis - PMCswr88kv5p2No ratings yet
- AdultOI CryptococcosisDocument18 pagesAdultOI CryptococcosisricardoatejassNo ratings yet
- Meningitis Workup - Approach Considerations, Blood Studies, Cultures and Bacterial Antigen TestingDocument14 pagesMeningitis Workup - Approach Considerations, Blood Studies, Cultures and Bacterial Antigen TestingdilaNo ratings yet
- Diagnostic Tests: Neisseria Meningitidis CapsularDocument2 pagesDiagnostic Tests: Neisseria Meningitidis CapsularCherry Mae JasoNo ratings yet
- Neurology NotesDocument87 pagesNeurology NotesKeval Shah100% (1)
- Meningitis PDFDocument8 pagesMeningitis PDFrizeviNo ratings yet
- Serum Procalcitonin Levels in Bacterial and Abacterial MeningitisDocument5 pagesSerum Procalcitonin Levels in Bacterial and Abacterial MeningitisSaul Gonzalez HernandezNo ratings yet
- CSF and Synovial FluidDocument12 pagesCSF and Synovial Fluidquerokeropi100% (1)
- Diagnosis and Treatment of Bacterial Meningitis: Arch. Dis. ChildDocument7 pagesDiagnosis and Treatment of Bacterial Meningitis: Arch. Dis. Childapi-214563632No ratings yet
- TB MeningitisDocument10 pagesTB Meningitisrizky ramadhanNo ratings yet
- Viral Inf of CNSDocument42 pagesViral Inf of CNSTarik100% (1)
- Bab I Pendahuluan Tuberculous Meningitis: Diagnosis and Treatment OverviewDocument14 pagesBab I Pendahuluan Tuberculous Meningitis: Diagnosis and Treatment OverviewInalNo ratings yet
- Diagnostic and Prognostic Role of Procalcitonin in CAPDocument5 pagesDiagnostic and Prognostic Role of Procalcitonin in CAPKarito FloresNo ratings yet
- Imp bn1Document5 pagesImp bn1Karito FloresNo ratings yet
- Neurology NotesDocument82 pagesNeurology NotesIulia TemuscoNo ratings yet
- Monocytogenes May Have Normal CSF WBC Results - Listeria May AlsoDocument4 pagesMonocytogenes May Have Normal CSF WBC Results - Listeria May AlsoAlfrien Ivanovich LarchsonNo ratings yet
- Tubercular MeningitisDocument60 pagesTubercular MeningitisVRUSHAB PARAPPANAVARNo ratings yet
- TBR PCPDocument28 pagesTBR PCPAyahnya Rafli100% (1)
- Cerebrospinal Fluid AnalysisDocument6 pagesCerebrospinal Fluid AnalysisAgustinus BethaNo ratings yet
- Ijpedi2021 1544553Document6 pagesIjpedi2021 1544553Naresh ReddyNo ratings yet
- CNS InfectionsDocument3 pagesCNS InfectionsStefy BarranoNo ratings yet
- CP Final KeynoteDocument20 pagesCP Final KeynoteLiana Ysabelle CasusiNo ratings yet
- 2017 Sept ReviewDocument7 pages2017 Sept ReviewJem QuintoNo ratings yet
- Aubf EeDocument26 pagesAubf EeAlleah MancillaNo ratings yet
- Meningitis, AAFPDocument8 pagesMeningitis, AAFPCarlos Danilo Noroña CNo ratings yet
- Delta Neutrophil Index As An Early MDocument9 pagesDelta Neutrophil Index As An Early MFariz NurNo ratings yet
- Bacterial Meningitis ThesisDocument8 pagesBacterial Meningitis ThesisRick Vogel100% (2)
- Q&A Oslo Revisi 61023Document10 pagesQ&A Oslo Revisi 61023syukriNo ratings yet
- Subacute and Chronic MeningitisDocument8 pagesSubacute and Chronic MeningitisLucky PuspitasariNo ratings yet
- Referat SepsisDocument18 pagesReferat SepsisImelva GirsangNo ratings yet
- Rheumatology LastDocument54 pagesRheumatology LastAbdallah K. RamadanNo ratings yet
- Dxto de Infecciones en El SNCDocument17 pagesDxto de Infecciones en El SNCcarlos ballestasNo ratings yet
- CNSinfectionsDocument79 pagesCNSinfectionsMatusala BafaNo ratings yet
- Sepsis in The Newborn - Latest NewsDocument13 pagesSepsis in The Newborn - Latest NewsBrunaNo ratings yet
- 24 - Liquor AnaliseDocument6 pages24 - Liquor AnaliseomboNo ratings yet
- Lumbar Puncture: Bagasin, Nester James S. Rodriguez, Lourdes Erika ADocument32 pagesLumbar Puncture: Bagasin, Nester James S. Rodriguez, Lourdes Erika ANdor BariboloNo ratings yet
- CMS Neuro 4 AnswersDocument20 pagesCMS Neuro 4 AnswersUsm Lee69% (16)
- Sepsis Diagnosis and Monitoring: Fast Early ReliableDocument24 pagesSepsis Diagnosis and Monitoring: Fast Early ReliableI Nyoman Gede Semarajana100% (1)
- Jurnal AsliDocument8 pagesJurnal AsliDwi PurwantiNo ratings yet
- Meningitis and Encephalitis: Samantha Noll June 11, 2015Document45 pagesMeningitis and Encephalitis: Samantha Noll June 11, 2015galihNo ratings yet
- Background: Mycobacterium Avium Complex (MAC) Consists of 2Document14 pagesBackground: Mycobacterium Avium Complex (MAC) Consists of 2readyboy89No ratings yet
- TB MeningitisDocument18 pagesTB Meningitisjesa34No ratings yet
- Cerebrospinal FluidDocument32 pagesCerebrospinal FluidRabbya Nasir 5No ratings yet
- Glchunk 321Document19 pagesGlchunk 321Hai SheikhNo ratings yet
- CNS Infections 2013 - MKDocument54 pagesCNS Infections 2013 - MKmicroperadeniyaNo ratings yet
- Harrison 164 - MeningitisDocument2 pagesHarrison 164 - MeningitisChristel GarciaNo ratings yet
- Meningitistb Journal 1Document15 pagesMeningitistb Journal 1RambuNo ratings yet
- Sepsis: Definition, Epidemiology, and Diagnosis: Clinical ReviewDocument5 pagesSepsis: Definition, Epidemiology, and Diagnosis: Clinical ReviewhfathiardiNo ratings yet
- (Methods in Molecular Medicine) Andrew J. Pollard, Martin C.J. Maiden - Meningococcal Disease (2001, Humana Press)Document662 pages(Methods in Molecular Medicine) Andrew J. Pollard, Martin C.J. Maiden - Meningococcal Disease (2001, Humana Press)gnkgbjkgjkNo ratings yet
- Nelson Textbook of Pediatrics, 19th Editon - KliegmanDocument1 pageNelson Textbook of Pediatrics, 19th Editon - KliegmanAgilan Nadarajan0% (1)
- Diagnosis, Treatment, and Prevention of Adenovirus Infection - UpToDateDocument28 pagesDiagnosis, Treatment, and Prevention of Adenovirus Infection - UpToDateMisael TaverasNo ratings yet
- 05 Investigations For PneumoniaDocument4 pages05 Investigations For Pneumoniause4meNo ratings yet
- Q&A OsloDocument9 pagesQ&A OslosyukriNo ratings yet
- Meningitis: By-Dr Nimco A. MDDocument31 pagesMeningitis: By-Dr Nimco A. MDgibreilNo ratings yet
- Case Study of Neurological DisordersDocument9 pagesCase Study of Neurological DisordersSkyerexNo ratings yet
- Nonimaging Diagnostic Tests For Pneumonia: Anupama Gupta Brixey,, Raju Reddy,, Shewit P. GiovanniDocument14 pagesNonimaging Diagnostic Tests For Pneumonia: Anupama Gupta Brixey,, Raju Reddy,, Shewit P. GiovannikaeranNo ratings yet
- Meningitis in Adults: Diagnosis and Management: PembimbingDocument45 pagesMeningitis in Adults: Diagnosis and Management: PembimbingNeny Mathilda UniplaitaNo ratings yet
- Diagnostics: CBC, CRP, UA, PCR, LAT, Blood Cultures CSF: With Opening Pressure, Procalcitonin and SerologyDocument4 pagesDiagnostics: CBC, CRP, UA, PCR, LAT, Blood Cultures CSF: With Opening Pressure, Procalcitonin and SerologyChoi SpeaksNo ratings yet
- Chronic Lymphocytic LeukemiaFrom EverandChronic Lymphocytic LeukemiaMichael HallekNo ratings yet
- Nursing Care Plan: University of Tabuk Faculty of Applied Medical Science Department of NursingDocument2 pagesNursing Care Plan: University of Tabuk Faculty of Applied Medical Science Department of Nursingعبداللة العمراني الحويطيNo ratings yet
- Drug StudyDocument2 pagesDrug Studyعبداللة العمراني الحويطيNo ratings yet
- Drug Study MatrixDocument2 pagesDrug Study Matrixعبداللة العمراني الحويطيNo ratings yet
- Case Study FormatDocument13 pagesCase Study Formatعبداللة العمراني الحويطيNo ratings yet
- Nursing Care Plan: University of Tabuk Faculty of Applied Medical Science Department of NursingDocument3 pagesNursing Care Plan: University of Tabuk Faculty of Applied Medical Science Department of Nursingعبداللة العمراني الحويطيNo ratings yet
- Nursing Care Plan: Acute Pain Related To Reduced Coronary Blood FlowDocument2 pagesNursing Care Plan: Acute Pain Related To Reduced Coronary Blood Flowعبداللة العمراني الحويطيNo ratings yet
- Adult Health ProjectDocument4 pagesAdult Health Projectعبداللة العمراني الحويطيNo ratings yet
- 5 Drug Study TEMPLATEDocument2 pages5 Drug Study TEMPLATEعبداللة العمراني الحويطيNo ratings yet
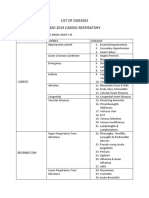
- List of Diseases Imo 2019 Cardio-RespiratoryDocument2 pagesList of Diseases Imo 2019 Cardio-RespiratoryDimas Adjie Yuda MahendraNo ratings yet
- Tertiary SyphilisDocument19 pagesTertiary SyphilisLakshya J BasumataryNo ratings yet
- Laban Movement Analysis Using KinectDocument11 pagesLaban Movement Analysis Using KinectRodrigo Balthar FurmanNo ratings yet
- Pemicu 4 GIT DevinDocument94 pagesPemicu 4 GIT DevinDevin AlexanderNo ratings yet
- GliomasDocument35 pagesGliomasRabbya Nasir 5No ratings yet
- UVA Family QuestionsDocument30 pagesUVA Family QuestionsSamuel RothschildNo ratings yet
- Disentri AmoebaDocument9 pagesDisentri AmoebaNur Fatimah MaharaniNo ratings yet
- Science 9 - 1ST Monthly TestDocument2 pagesScience 9 - 1ST Monthly TestMaria JocosaNo ratings yet
- 10 Diagnosa TerbanyakDocument6 pages10 Diagnosa TerbanyakErnyNo ratings yet
- Malignant Myopericytoma: Report of A New Case and Review of The LiteratureDocument6 pagesMalignant Myopericytoma: Report of A New Case and Review of The LiteratureRachel AutranNo ratings yet
- Association of Vaginal Infections in Preterm Labour: Srilakshmi Yarlagadda, Sajana G., Prasuna J. L. NarraDocument6 pagesAssociation of Vaginal Infections in Preterm Labour: Srilakshmi Yarlagadda, Sajana G., Prasuna J. L. NarraNurRahMatNo ratings yet
- Soal Science - Digestive System & Respirotary SystemDocument3 pagesSoal Science - Digestive System & Respirotary SystemEMIL SALNo ratings yet
- Cytodiagnosis in DermatologyDocument5 pagesCytodiagnosis in DermatologyDipti MathiasNo ratings yet
- 1.neofax - Maged ZakariaDocument128 pages1.neofax - Maged Zakariaengy6nagy0% (1)
- HypoparathyroidismDocument2 pagesHypoparathyroidismLorelyn Santos CorpuzNo ratings yet
- Deep-Brain Stimulation For Parkinson's Disease: Clinical TherapeuticsDocument10 pagesDeep-Brain Stimulation For Parkinson's Disease: Clinical TherapeuticsanonimoNo ratings yet
- Amyotrophic Lateral SclerosisDocument23 pagesAmyotrophic Lateral SclerosisAfshan Pt T100% (1)
- Folic AcidDocument5 pagesFolic Acidjyoti singhNo ratings yet
- Hermansky Pudlak Syndrome Report of A Case and Review of The LiteratureDocument5 pagesHermansky Pudlak Syndrome Report of A Case and Review of The LiteraturepushkaradmaneNo ratings yet
- Congestive Heart FailureDocument5 pagesCongestive Heart FailureKaren PanganibanNo ratings yet
- Funda SL FinalsDocument3 pagesFunda SL FinalsKarylle Joy ValenciaNo ratings yet
- Cardiopulmonary System: Relevant Anatomy & Physiology: HeartDocument12 pagesCardiopulmonary System: Relevant Anatomy & Physiology: HeartJulia SalvioNo ratings yet
- Generic Name (Brand Name) Classification Dosage Indication/ Contraindication Nursing ResponsibilitiesDocument3 pagesGeneric Name (Brand Name) Classification Dosage Indication/ Contraindication Nursing ResponsibilitiesJoe Anne Maniulit, MSN, RNNo ratings yet
- Siegelman Online Advantage 1.1 PDFDocument39 pagesSiegelman Online Advantage 1.1 PDFDana Ysabelle Ibarra100% (1)
- Stroke Reports Following Covid VaccineDocument9 pagesStroke Reports Following Covid VaccineJosh Singer100% (2)
- Topnotch Ent Supplement Handout Updated April 2016pdf PDFDocument15 pagesTopnotch Ent Supplement Handout Updated April 2016pdf PDFKenneth NuñezNo ratings yet
- (CC1) LEC-W12-Nonprotein Nitrogen CompoundsDocument10 pages(CC1) LEC-W12-Nonprotein Nitrogen CompoundsAira UsiNo ratings yet
- DELIRIUMDocument68 pagesDELIRIUMVarada PanikkathNo ratings yet
- Practical PerformaDocument4 pagesPractical PerformaVijay Pradeep100% (3)
- Neutrophilia: Nonmalignant Leukocyte DisordersDocument19 pagesNeutrophilia: Nonmalignant Leukocyte DisordersRachel PlanillaNo ratings yet