You might also like
- PALS Fluids and ElectrolytesDocument32 pagesPALS Fluids and ElectrolytesZi SongNo ratings yet
- Critical Care Medicine Tutorials - HyernatremiaDocument4 pagesCritical Care Medicine Tutorials - Hyernatremiamsrapp100% (1)
- Under The Guidance Of: Dr. B.Shashidharan. Professor and Chief Unit-III By, Dr. Henley Punnen AndrewsDocument63 pagesUnder The Guidance Of: Dr. B.Shashidharan. Professor and Chief Unit-III By, Dr. Henley Punnen AndrewsHenley AndrewsNo ratings yet
- Guideline, Management of HypernatremiaDocument9 pagesGuideline, Management of HypernatremiaLia Safitri Leloly100% (1)
- Surgery YbDocument67 pagesSurgery YbTamirat geletaNo ratings yet
- Flluid and ElectDocument107 pagesFlluid and ElectHassan SalamehNo ratings yet
- Case Sharing - Medicine DutyDocument6 pagesCase Sharing - Medicine DutyReihann N. EdresNo ratings yet
- RANASINGHE Fluid Electrolyte and Acid Base PhysiologyDocument45 pagesRANASINGHE Fluid Electrolyte and Acid Base PhysiologyDagimNo ratings yet
- Module 2 Fluid Electrolyte Disorders Acid Base Notes 9th EdDocument15 pagesModule 2 Fluid Electrolyte Disorders Acid Base Notes 9th EdSara FNo ratings yet
- Liquidos IVDocument4 pagesLiquidos IVpaula torresNo ratings yet
- Disturbances in Water, Electrolyte and Acid-Base Balance: Dr. Njau.N.NDocument52 pagesDisturbances in Water, Electrolyte and Acid-Base Balance: Dr. Njau.N.NKeith OmwoyoNo ratings yet
- Hypernatremia Treatment & Management - Medical Care, Surgical Care, ConsultationsDocument3 pagesHypernatremia Treatment & Management - Medical Care, Surgical Care, ConsultationsJorge Luis German BecerraNo ratings yet
- Electrolyte TextDocument16 pagesElectrolyte TextHany ElbarougyNo ratings yet
- IV Infusion SolutionDocument8 pagesIV Infusion SolutionmohammedNo ratings yet
- Hyponatremia: Causes, Evaluation & TreatmentDocument20 pagesHyponatremia: Causes, Evaluation & TreatmentmanjaruNo ratings yet
- HyponatremiaDocument42 pagesHyponatremiaAbdu Raheem100% (1)
- pdfDocument2 pagespdfbebeNo ratings yet
- Guidelines For Management Of: HypernatremiaDocument7 pagesGuidelines For Management Of: HypernatremiaSarly Puspita AriesaNo ratings yet
- M5 - Electrolyte AbnormalitiesDocument44 pagesM5 - Electrolyte AbnormalitiesVishal KumarNo ratings yet
- Electrolyte Imbalance: Sodium: Submitted By: Milosantos, John Francis D. Tuibeo, Ma. Arlyn P. Yu, Aldrin Anthony LDocument6 pagesElectrolyte Imbalance: Sodium: Submitted By: Milosantos, John Francis D. Tuibeo, Ma. Arlyn P. Yu, Aldrin Anthony Lnospekiko21No ratings yet
- Practical Guide to Disorders of Water Balance and Hyponatremia/HypernatremiaDocument22 pagesPractical Guide to Disorders of Water Balance and Hyponatremia/HypernatremiafatmaNo ratings yet
- Disorders of SodiumDocument38 pagesDisorders of SodiumMuhammad FaizanNo ratings yet
- Intravenous Fluid Therapy For 2nd Year ConceptDocument83 pagesIntravenous Fluid Therapy For 2nd Year ConceptMay Chelle ErazoNo ratings yet
- Hypernatremia: Marielle Adey R. Magcawas BSN-3CDocument28 pagesHypernatremia: Marielle Adey R. Magcawas BSN-3CMarielle Adey Magcawas RNNo ratings yet
- Hyponatremia in Neurological Diseases in ICU: Review ArticleDocument5 pagesHyponatremia in Neurological Diseases in ICU: Review ArticlealdiansyahraufNo ratings yet
- 10 CLS 382 443 Electrolytes I Na and Fluid Balance FINALDocument16 pages10 CLS 382 443 Electrolytes I Na and Fluid Balance FINALamalNo ratings yet
- FLUID AND ELECTROLYTE MANAGEMENT OF SURGICAL PATIENTSDocument37 pagesFLUID AND ELECTROLYTE MANAGEMENT OF SURGICAL PATIENTSJie CuetoNo ratings yet
- REGULATION OF FLUID AND ELECTROLYTE BALANCEDocument18 pagesREGULATION OF FLUID AND ELECTROLYTE BALANCEKim RamosNo ratings yet
- SiadhDocument16 pagesSiadhGokul Rajan100% (1)
- Intravenous Fluid Therapy GuideDocument68 pagesIntravenous Fluid Therapy GuideMourian AmanNo ratings yet
- Fluid TherapyDocument36 pagesFluid TherapyAmin MasromNo ratings yet
- How To Respond To Abnormal Serum Sodium LevelsDocument3 pagesHow To Respond To Abnormal Serum Sodium LevelsNixNo ratings yet
- Ivfluidtherapytypesindicationsdosescalculation 130123090523 Phpapp01Document68 pagesIvfluidtherapytypesindicationsdosescalculation 130123090523 Phpapp01rainNo ratings yet
- Hypernatremic DehydrationDocument3 pagesHypernatremic DehydrationVandanaNo ratings yet
- 3 Fluid and ElectrolyteDocument7 pages3 Fluid and ElectrolyteStephen HDNo ratings yet
- XAVIER UNIVERSITY – ATENEO DE CAGAYAN COLLEGE OF NURSING CONCEPT MAP: HYPONATREMIADocument9 pagesXAVIER UNIVERSITY – ATENEO DE CAGAYAN COLLEGE OF NURSING CONCEPT MAP: HYPONATREMIAElleNo ratings yet
- Burn Fluid Resuscitation GuideDocument35 pagesBurn Fluid Resuscitation GuideNur Anniesa100% (2)
- Refreshing " Fluid Therapy"Document28 pagesRefreshing " Fluid Therapy"Bangun Cholifa nusantaraNo ratings yet
- Dr. Tiu - Electrolyte RequirementsDocument64 pagesDr. Tiu - Electrolyte Requirementshippypsyduck mdNo ratings yet
- FiiiiiiixDocument22 pagesFiiiiiiixYeni dwi anggra sudarmajiNo ratings yet
- Fluid Replacement TherapyDocument3 pagesFluid Replacement TherapyJesusreignsNo ratings yet
- Fluid Management in PediatricsDocument3 pagesFluid Management in PediatricsZiyadNo ratings yet
- IV FluidDocument49 pagesIV Fluidibrahimadnan040No ratings yet
- Elektrolit GGNDocument16 pagesElektrolit GGNlianaNo ratings yet
- Hyponatremia (Emphasis On SIADH) : DR Adeyemo A. ODocument57 pagesHyponatremia (Emphasis On SIADH) : DR Adeyemo A. OAdeyemo AyoadeNo ratings yet
- Electrolyte and Acid Base BalanceDocument26 pagesElectrolyte and Acid Base BalanceMysheb SSNo ratings yet
- Fluid Resuscitation NewDocument32 pagesFluid Resuscitation Newffattimu667No ratings yet
- Fluid ManagementDocument10 pagesFluid ManagementdradaadNo ratings yet
- FLUID AND ELECTROLYTE THERAPYDocument47 pagesFLUID AND ELECTROLYTE THERAPYSeblewongel AsemeNo ratings yet
- Hypernatremia: Causes, Symptoms and TreatmentDocument16 pagesHypernatremia: Causes, Symptoms and TreatmentBlessyNo ratings yet
- Pediatric Fluid Therapy GuideDocument27 pagesPediatric Fluid Therapy GuideNanda Cendikia100% (1)
- Medical Surgical Fluid and Electrolytes FVD FVEDocument7 pagesMedical Surgical Fluid and Electrolytes FVD FVEMichaelaKatrinaTrinidadNo ratings yet
- Guidelines For The Management of HyponatraemiaDocument8 pagesGuidelines For The Management of HyponatraemiaMuhammad Amiro RasheeqNo ratings yet
- Electrolyte DisordersDocument10 pagesElectrolyte DisordersSlavicaNo ratings yet
- Pocket Card - IV Fluids - December 2023Document6 pagesPocket Card - IV Fluids - December 2023Evieta CallysthaNo ratings yet
- Pleno Minggu 2 Blok 3.4Document84 pagesPleno Minggu 2 Blok 3.4Devi Yunita PurbaNo ratings yet
- Common Electrolyte Disturbance Their Management and Anesthesia ConsiderationDocument65 pagesCommon Electrolyte Disturbance Their Management and Anesthesia ConsiderationagatakassaNo ratings yet
- NCM 3114 Electrolyte Imbalance-2Document21 pagesNCM 3114 Electrolyte Imbalance-2Nicole Sherry M. CHEENo ratings yet
- Fracture Healing - Basic Science - Orthobullets PDFDocument2 pagesFracture Healing - Basic Science - Orthobullets PDFMelAcostaNo ratings yet
- Med-Surg Exam #2 Study GuideDocument33 pagesMed-Surg Exam #2 Study GuideCaitlyn BilbaoNo ratings yet
- NCM101 TransesDocument6 pagesNCM101 TransesRonel ResurricionNo ratings yet
- Neurocognitive Disorders NotesDocument8 pagesNeurocognitive Disorders NotesJuanchovieldiazNo ratings yet
- MPPC Health Indeminity FormDocument2 pagesMPPC Health Indeminity FormmichaelforkcsNo ratings yet
- This Is What Happens When You're A Couch Potato: Que-Resultan-Insultantes-Para-Los-HombresDocument6 pagesThis Is What Happens When You're A Couch Potato: Que-Resultan-Insultantes-Para-Los-HombresKatarina JovanovićNo ratings yet
- 2019 National Prosthodontic Resident Exam: © 2019 American College of Prosthodontists. All Rights ReservedDocument48 pages2019 National Prosthodontic Resident Exam: © 2019 American College of Prosthodontists. All Rights ReservedAwaisNo ratings yet
- Pedia Prof - OamilDocument147 pagesPedia Prof - OamilOne Click Online ShopNo ratings yet
- Ada 2 2023Document22 pagesAda 2 2023desireth vazquezNo ratings yet
- HIV/Syphilis StudiesDocument2 pagesHIV/Syphilis StudiesYusuf Arif SalamNo ratings yet
- 19 04 2020 Mumbai PDFDocument33 pages19 04 2020 Mumbai PDFShaji VkNo ratings yet
- Head Injuries ( Lesiones de Cabeza)Document5 pagesHead Injuries ( Lesiones de Cabeza)Camila BenitezNo ratings yet
- SHAHMEERDocument29 pagesSHAHMEERMosa AbdullahNo ratings yet
- Chapter 29: Perinatal Disorders Garzon Maaks: Burns' Pediatric Primary Care, 7th EditionDocument2 pagesChapter 29: Perinatal Disorders Garzon Maaks: Burns' Pediatric Primary Care, 7th EditionHelen UgochukwuNo ratings yet
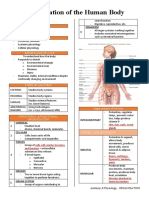
- Organization of the Human BodyDocument8 pagesOrganization of the Human BodyAly HannahNo ratings yet
- GlobalPharma's 2013 Marketing Plan for Omeprazole in UAEDocument38 pagesGlobalPharma's 2013 Marketing Plan for Omeprazole in UAEmaawi2002yahoocomNo ratings yet
- Excess Deaths Involving CVD in England An Anlysis and ExplainerDocument36 pagesExcess Deaths Involving CVD in England An Anlysis and ExplainerJamie White100% (2)
- Gardner 2015Document6 pagesGardner 2015Alvaro Quincho LópezNo ratings yet
- One Shot Revision Patho by DR PraveenDocument19 pagesOne Shot Revision Patho by DR PraveenTauqueer AlamNo ratings yet
- Gastrointestinal Disorders GuideDocument14 pagesGastrointestinal Disorders GuideAnna Sofia Reyes100% (1)
- SunheimerSS Chapter10Document3 pagesSunheimerSS Chapter10Ajien TaiajNo ratings yet
- Daily Lesson Plan in English Grade 7 (Quarter 3-Module 5)Document2 pagesDaily Lesson Plan in English Grade 7 (Quarter 3-Module 5)Ramil60% (5)
- ZOOL 143 Topic 6 Diseases Assosiated With HIV and AIDSDocument9 pagesZOOL 143 Topic 6 Diseases Assosiated With HIV and AIDSnattydreadfathelahNo ratings yet
- Primary Mitochondrial Myopathies in Childhood 2021 Neuromuscular DisordersDocument10 pagesPrimary Mitochondrial Myopathies in Childhood 2021 Neuromuscular DisordersSuzie Simone Mardones SilvaNo ratings yet
- Grandes Desafios para A Prevenção e Reabilitação de Lesões EsportivasDocument5 pagesGrandes Desafios para A Prevenção e Reabilitação de Lesões EsportivasEdilis FlorNo ratings yet
- Factors Affecting Stability of OrthodontDocument7 pagesFactors Affecting Stability of OrthodontSALAHEDDINE BLIZAKNo ratings yet
- Mock Up Test 1Document3 pagesMock Up Test 1Mateusz Radwański100% (1)
- One Health Approach: Saving Lives by Taking ADocument4 pagesOne Health Approach: Saving Lives by Taking AagneselimNo ratings yet
- Effect of Virtual Reality Exercises On BalanceDocument9 pagesEffect of Virtual Reality Exercises On BalanceLuís Otávio S. BarbosaNo ratings yet
- Perioperative nursing considerationsDocument9 pagesPerioperative nursing considerationsKoleen Kirsten100% (1)