You might also like
- Acid-Base and Electrolyte Handbook for Veterinary TechniciansFrom EverandAcid-Base and Electrolyte Handbook for Veterinary TechniciansAngela Randels-ThorpNo ratings yet
- Metabolic Disorders and Critically Ill Patients: From Pathophysiology to TreatmentFrom EverandMetabolic Disorders and Critically Ill Patients: From Pathophysiology to TreatmentCarole IchaiNo ratings yet
- IV Infusion SolutionDocument8 pagesIV Infusion SolutionmohammedNo ratings yet
- Ringer's Lactate - StatPearls - NCBI BookshelfDocument4 pagesRinger's Lactate - StatPearls - NCBI BookshelfMarfu'ah Mar'ahNo ratings yet
- Pediatric Sodium GuidelineDocument6 pagesPediatric Sodium GuidelineNisa Fithria LathifahNo ratings yet
- Ringer's Lactate: Indications, Mechanism, Administration & MonitoringDocument5 pagesRinger's Lactate: Indications, Mechanism, Administration & MonitoringagusNo ratings yet
- Intravenous Fluid Therapy For 2nd Year ConceptDocument83 pagesIntravenous Fluid Therapy For 2nd Year ConceptMay Chelle ErazoNo ratings yet
- Under The Guidance Of: Dr. B.Shashidharan. Professor and Chief Unit-III By, Dr. Henley Punnen AndrewsDocument63 pagesUnder The Guidance Of: Dr. B.Shashidharan. Professor and Chief Unit-III By, Dr. Henley Punnen AndrewsHenley AndrewsNo ratings yet
- pdfDocument2 pagespdfbebeNo ratings yet
- Fluid Therapy For Critically Ill Dogs and Cats - WSAVA2005 - VINDocument14 pagesFluid Therapy For Critically Ill Dogs and Cats - WSAVA2005 - VINHament KumarNo ratings yet
- IV FluidDocument49 pagesIV Fluidibrahimadnan040No ratings yet
- Fluidoterapia em Pequenos AnimaisDocument14 pagesFluidoterapia em Pequenos AnimaisClarice GonringNo ratings yet
- Pocket Card - IV Fluids - December 2023Document6 pagesPocket Card - IV Fluids - December 2023Evieta CallysthaNo ratings yet
- Refreshing " Fluid Therapy"Document28 pagesRefreshing " Fluid Therapy"Bangun Cholifa nusantaraNo ratings yet
- Intravenous Fluid Therapy GuideDocument68 pagesIntravenous Fluid Therapy GuideMourian AmanNo ratings yet
- Iv FluidsDocument92 pagesIv Fluidsakish4u86% (7)
- Ivfluidtherapytypesindicationsdosescalculation 130123090523 Phpapp01Document68 pagesIvfluidtherapytypesindicationsdosescalculation 130123090523 Phpapp01rainNo ratings yet
- Nursing Programs: Lactated Ringers (Also Known As LR, Ringers Lactate, or RL)Document5 pagesNursing Programs: Lactated Ringers (Also Known As LR, Ringers Lactate, or RL)KiaBlancheTahud100% (1)
- Flluid and ElectDocument107 pagesFlluid and ElectHassan SalamehNo ratings yet
- Smith L (2017) Nursing Times 113: 12, 20-23Document59 pagesSmith L (2017) Nursing Times 113: 12, 20-23Derick RanaNo ratings yet
- LEV IntraoperatoriosDocument11 pagesLEV IntraoperatoriosCasual CasualNo ratings yet
- PALS Fluids and ElectrolytesDocument32 pagesPALS Fluids and ElectrolytesZi SongNo ratings yet
- College of Health Sciences: Urdaneta City UniversityDocument5 pagesCollege of Health Sciences: Urdaneta City UniversityDan Dan ManaoisNo ratings yet
- Fluid Resuscitation NewDocument32 pagesFluid Resuscitation Newffattimu667No ratings yet
- Intravenous Fluids: Composition & UsesDocument41 pagesIntravenous Fluids: Composition & UsesFathima BanuzNo ratings yet
- Post Operative Intravenous Fluids: Supervised By: DR Dilan ZakariaDocument49 pagesPost Operative Intravenous Fluids: Supervised By: DR Dilan Zakariamuhammed barznjiNo ratings yet
- Fluid Therapy Selection Guide for Medical DisordersDocument4 pagesFluid Therapy Selection Guide for Medical DisordersSandip PatilNo ratings yet
- Maintenance and Replacement Therapy: Fluids and Electrolytes (Part 2)Document6 pagesMaintenance and Replacement Therapy: Fluids and Electrolytes (Part 2)Maikka IlaganNo ratings yet
- Fluid & Electrolyte TherapyDocument33 pagesFluid & Electrolyte Therapyhendra_darmawan_4No ratings yet
- Perioperative Fluid Management: Presented by Murad Satary Moderator:Dr - Ibrahim QudaisatDocument80 pagesPerioperative Fluid Management: Presented by Murad Satary Moderator:Dr - Ibrahim QudaisatMorad SatariNo ratings yet
- Fluid ManagementDocument11 pagesFluid ManagementAtzi FNo ratings yet
- IV Fluids TheoryDocument13 pagesIV Fluids TheoryFRESY TRI SUGIANTONo ratings yet
- Hypernatremia Treatment & Management - Medical Care, Surgical Care, ConsultationsDocument3 pagesHypernatremia Treatment & Management - Medical Care, Surgical Care, ConsultationsJorge Luis German BecerraNo ratings yet
- Critical Care Medicine Tutorials - HyernatremiaDocument4 pagesCritical Care Medicine Tutorials - Hyernatremiamsrapp100% (1)
- IV Fluid Lecturette for Nursing StudentsDocument16 pagesIV Fluid Lecturette for Nursing StudentsbabiNo ratings yet
- Maintenance & Replacement Fluid Therapy: Moderated by DR - Madhuri EngadeDocument43 pagesMaintenance & Replacement Fluid Therapy: Moderated by DR - Madhuri EngadeTonny ChenNo ratings yet
- Disturbances in Water, Electrolyte and Acid-Base Balance: Dr. Njau.N.NDocument52 pagesDisturbances in Water, Electrolyte and Acid-Base Balance: Dr. Njau.N.NKeith OmwoyoNo ratings yet
- IV Fluid/Solution Quick Reference GuideDocument2 pagesIV Fluid/Solution Quick Reference GuideCin DyNo ratings yet
- RingersLactate StatPearls NCBIBookshelfDocument4 pagesRingersLactate StatPearls NCBIBookshelfTommy AreanNo ratings yet
- Normal Saline - StatPearls - NCBI BookshelfDocument8 pagesNormal Saline - StatPearls - NCBI BookshelfHakam LababnehNo ratings yet
- Seminar - Fluids and Electrolytes 09-12-2019Document59 pagesSeminar - Fluids and Electrolytes 09-12-2019Chandra dimpleNo ratings yet
- Fluid & Electrolyte TherapyDocument38 pagesFluid & Electrolyte Therapyharjuna100% (1)
- Surgery YbDocument67 pagesSurgery YbTamirat geletaNo ratings yet
- Different Iv FluidsDocument2 pagesDifferent Iv FluidsBeverly DatuNo ratings yet
- Fluid and ElectrolyteDocument71 pagesFluid and ElectrolytePratishtha SinghNo ratings yet
- IV Fluids: CrystalloidsDocument6 pagesIV Fluids: CrystalloidsGlaiza BartolomeNo ratings yet
- IV Fluid CommonDocument1 pageIV Fluid CommonmydewyboyNo ratings yet
- Clinical Skills: Intravenous Fluid and Setting Up A DripDocument30 pagesClinical Skills: Intravenous Fluid and Setting Up A DripNabhan MohamedNo ratings yet
- 10 CLS 382 443 Electrolytes I Na and Fluid Balance FINALDocument16 pages10 CLS 382 443 Electrolytes I Na and Fluid Balance FINALamalNo ratings yet
- Fluid Therapy: Presenter: Chew Zi Qi Supervisor: Dr. Tan KWDocument43 pagesFluid Therapy: Presenter: Chew Zi Qi Supervisor: Dr. Tan KWaslanNo ratings yet
- Intravenous Fluid (6th. 7th. Weeks)Document20 pagesIntravenous Fluid (6th. 7th. Weeks)Samer AlBaghdadiNo ratings yet
- 1.1a Fluid Management 6th Seminar GRP AaDocument40 pages1.1a Fluid Management 6th Seminar GRP AahalearnNo ratings yet
- IV Fluids ExplainedDocument5 pagesIV Fluids ExplainedRegine Mae Encinada100% (1)
- Smith L (2017) Nursing Times 113: 12, 20-23Document59 pagesSmith L (2017) Nursing Times 113: 12, 20-23Derick RanaNo ratings yet
- Intravenous fluid therapy monitoring for pharmacistsDocument4 pagesIntravenous fluid therapy monitoring for pharmacistsjorge zuñigaNo ratings yet
- IV Fluid Types and Nursing ConsiderationsDocument6 pagesIV Fluid Types and Nursing ConsiderationsnicoleNo ratings yet
- SAS 9 Parenteral TherapyDocument41 pagesSAS 9 Parenteral Therapyjenet soleilNo ratings yet
- Intravenous FluidsDocument19 pagesIntravenous Fluidsnicolinna2000yahoo.comNo ratings yet
- Dehydration 4Document73 pagesDehydration 4Ali YousefNo ratings yet
- Equine Fluid TherapyFrom EverandEquine Fluid TherapyC. Langdon FieldingNo ratings yet
- Presentation 1Document20 pagesPresentation 1nikitakhanduja1304No ratings yet
- SMEs, Trade Finance and New TechnologyDocument34 pagesSMEs, Trade Finance and New TechnologyADBI EventsNo ratings yet
- Load Frequency Control of Hydro and Nuclear Power System by PI & GA ControllerDocument6 pagesLoad Frequency Control of Hydro and Nuclear Power System by PI & GA Controllerijsret100% (1)
- Design & Construction of Substation 16P Painting System ComplianceDocument103 pagesDesign & Construction of Substation 16P Painting System ComplianceRamil LazNo ratings yet
- Mechanical Engineer with Experience in Heavy Mining Machinery MaintenanceDocument1 pageMechanical Engineer with Experience in Heavy Mining Machinery MaintenanceCertified Rabbits LoverNo ratings yet
- A61C00100 Communication and Employee Engagement by Mary Welsh 2Document19 pagesA61C00100 Communication and Employee Engagement by Mary Welsh 2Moeshfieq WilliamsNo ratings yet
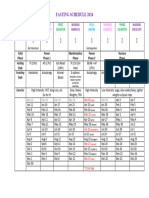
- Moon Fast Schedule 2024Document1 pageMoon Fast Schedule 2024mimiemendoza18No ratings yet
- Project Report On AdidasDocument33 pagesProject Report On Adidassanyam73% (37)
- Clarinet Lecture Recital - Jude StefanikDocument35 pagesClarinet Lecture Recital - Jude Stefanikapi-584164068No ratings yet
- Medicinal PlantDocument13 pagesMedicinal PlantNeelum iqbalNo ratings yet
- InteliLite AMF20-25Document2 pagesInteliLite AMF20-25albertooliveira100% (2)
- History and Development of the Foodservice IndustryDocument23 pagesHistory and Development of the Foodservice IndustryMaria Athenna MallariNo ratings yet
- ElectricalDocument30 pagesElectricalketerNo ratings yet
- Oracle® E-Business Suite: Integrated SOA Gateway Implementation Guide Release 12.2Document202 pagesOracle® E-Business Suite: Integrated SOA Gateway Implementation Guide Release 12.2yadavdevenderNo ratings yet
- The Mars ForceDocument249 pagesThe Mars Forceridikitty100% (2)
- Organizational Behaviour Group Assignment-2Document4 pagesOrganizational Behaviour Group Assignment-2Prateek KurupNo ratings yet
- Inspection and Acceptance Report: Stock No. Unit Description QuantityDocument6 pagesInspection and Acceptance Report: Stock No. Unit Description QuantityAnj LeeNo ratings yet
- Hanwha Engineering & Construction - Brochure - enDocument48 pagesHanwha Engineering & Construction - Brochure - enAnthony GeorgeNo ratings yet
- Casestudy3 Hbo MaDocument2 pagesCasestudy3 Hbo Ma132345usdfghjNo ratings yet
- Ketchikan Shipyard Improvements Plan CompleteDocument230 pagesKetchikan Shipyard Improvements Plan CompleteOpó Ishak Bawias Adare100% (1)
- MATHEMATICAL ECONOMICSDocument54 pagesMATHEMATICAL ECONOMICSCities Normah0% (1)
- NSX 100-630 User ManualDocument152 pagesNSX 100-630 User Manualagra04100% (1)
- Getting the Most from Cattle Manure: Proper Application Rates and PracticesDocument4 pagesGetting the Most from Cattle Manure: Proper Application Rates and PracticesRamNocturnalNo ratings yet
- JTP Brochure - 2Document6 pagesJTP Brochure - 2YAKOVNo ratings yet
- Siga-Cc1 12-22-2010Document6 pagesSiga-Cc1 12-22-2010Felipe LozanoNo ratings yet
- Plastic Welding: We Know HowDocument125 pagesPlastic Welding: We Know Howprabal rayNo ratings yet
- ProjectDocument86 pagesProjectrajuNo ratings yet
- Lesson Plan 2 Revised - Morgan LegrandDocument19 pagesLesson Plan 2 Revised - Morgan Legrandapi-540805523No ratings yet
- City MSJDocument50 pagesCity MSJHilary LedwellNo ratings yet
- Advanced Presentation Skills: Creating Effective Presentations with Visuals, Simplicity and ClarityDocument15 pagesAdvanced Presentation Skills: Creating Effective Presentations with Visuals, Simplicity and ClarityGilbert TamayoNo ratings yet