You might also like
- List of Herbs and Magic PropertiesDocument7 pagesList of Herbs and Magic PropertiesAndrew Stueckrad100% (1)
- Basics of Immunity and InflammationDocument6 pagesBasics of Immunity and InflammationNegrus Stefan100% (1)
- Sample Medical Specialty QuestionsDocument58 pagesSample Medical Specialty Questionsplayuhz100% (1)
- 200 Pages of MCQs LJDocument96 pages200 Pages of MCQs LJijojo elizabethNo ratings yet
- Fast F A S T: Recognizing Stroke: Ace Rms Peech ImeDocument25 pagesFast F A S T: Recognizing Stroke: Ace Rms Peech ImeIliescu DenisaNo ratings yet
- Anatomy and Physiology of The BreastDocument42 pagesAnatomy and Physiology of The BreastNicole SooNo ratings yet
- Elaj Al SalikinDocument80 pagesElaj Al SalikinMohammed Abdul Hafeez, B.Com., Hyderabad, India100% (1)
- Anaesthesia MCQDocument10 pagesAnaesthesia MCQshbhumi576100% (1)
- Ten Teacher Multiple AnswerDocument7 pagesTen Teacher Multiple Answerخلدون سليم100% (1)
- BathingDocument53 pagesBathingRandySandovalNo ratings yet
- GP MCQ 3Document4 pagesGP MCQ 3Marta MoreiraNo ratings yet
- Stress Management in BankingDocument45 pagesStress Management in BankingShop987 ssNo ratings yet
- 71 Model Test Paper of Post Basic Nursing Entrance Aiims 2020Document5 pages71 Model Test Paper of Post Basic Nursing Entrance Aiims 2020Your Tech SipNo ratings yet
- Nurse Exam QuestionsDocument3 pagesNurse Exam QuestionsrenjiniNo ratings yet
- Guymer Giant Cell Arteritis Polymyalgia Rheumatica FibromyalgiaDocument93 pagesGuymer Giant Cell Arteritis Polymyalgia Rheumatica FibromyalgiaKe Xu100% (1)
- 200 Pages of McqsDocument112 pages200 Pages of McqsSelim TarekNo ratings yet
- WHO Setting The Standard For A Wireless World of HarmDocument57 pagesWHO Setting The Standard For A Wireless World of HarmNataša AndrićNo ratings yet
- MCQ Anaesthesia QuestionsDocument4 pagesMCQ Anaesthesia Questionsapi-2629165181% (32)
- Primary EDADocument4 pagesPrimary EDADsdNo ratings yet
- MJCQDocument94 pagesMJCQElsayed Ahmed0% (1)
- Farm Animal Anesthesia: Cattle, Small Ruminants, Camelids, and PigsFrom EverandFarm Animal Anesthesia: Cattle, Small Ruminants, Camelids, and PigsHuiChu LinNo ratings yet
- Nursing Test 2 (NP Ii)Document7 pagesNursing Test 2 (NP Ii)Yuxin LiuNo ratings yet
- Multiple Choice Questions: Chronic Obstructive Pulmonary Disease and Anaesthesia Anaesthesia For Awake CraniotomyDocument4 pagesMultiple Choice Questions: Chronic Obstructive Pulmonary Disease and Anaesthesia Anaesthesia For Awake CraniotomyEliza AmandoNo ratings yet
- Multiple Choice Physiology ExamDocument3 pagesMultiple Choice Physiology ExamHusna MorradNo ratings yet
- Multiple Choice QuestionsDocument2 pagesMultiple Choice QuestionsChudaman Mahajan100% (1)
- Multiple Choice Questions: DOI 10.1093/bjacepd/mkg125Document2 pagesMultiple Choice Questions: DOI 10.1093/bjacepd/mkg125Florence BamigbolaNo ratings yet
- Multiple Choice QuestionsDocument3 pagesMultiple Choice QuestionsNoor AhmedNo ratings yet
- Multiple Choice Questions: Preventing Postoperative Infection: The Anaesthetist's RoleDocument4 pagesMultiple Choice Questions: Preventing Postoperative Infection: The Anaesthetist's Roleiqra uroojNo ratings yet
- Umum 2Document22 pagesUmum 2farid akbarNo ratings yet
- Pi Is 1743181617300586Document4 pagesPi Is 1743181617300586Yasmin ElsisiNo ratings yet
- PIIS1743181617306170Document2 pagesPIIS1743181617306170Vikash KushwahaNo ratings yet
- Multiple Choice Questions: Enhanced Recovery For Lower Limb ArthroplastyDocument5 pagesMultiple Choice Questions: Enhanced Recovery For Lower Limb ArthroplastyMaid LampardNo ratings yet
- Multiple-Choice Questionnaire: Functional Pelvic Floor ImagingDocument3 pagesMultiple-Choice Questionnaire: Functional Pelvic Floor Imagingtesfaye mekonnenNo ratings yet
- Piis1743181617301890 PDFDocument4 pagesPiis1743181617301890 PDFZiaur RehmanNo ratings yet
- GP MCQ 1Document4 pagesGP MCQ 1Marta MoreiraNo ratings yet
- Multiple Choice Questions: Never Events: An Anaesthetic PerspectiveDocument4 pagesMultiple Choice Questions: Never Events: An Anaesthetic Perspectiveامین ثانیNo ratings yet
- Multiple Choice Questions: Parenteral Nutrition in Critical CareDocument3 pagesMultiple Choice Questions: Parenteral Nutrition in Critical Careabhisheknrs78No ratings yet
- Multiple Choice Questions on Anaesthesia TopicsDocument3 pagesMultiple Choice Questions on Anaesthesia TopicsAbubakar AbdhooNo ratings yet
- Multiple Choice Questions: Anaesthesia For Major Spinal Surgery Paracetamol - Mechanisms and UpdatesDocument5 pagesMultiple Choice Questions: Anaesthesia For Major Spinal Surgery Paracetamol - Mechanisms and UpdatesFarhana RashenaNo ratings yet
- Multiple Choice QuestionsDocument2 pagesMultiple Choice Questionsabdulahi abdiNo ratings yet
- Multiple Choice QuestionsDocument2 pagesMultiple Choice QuestionsAhmad FarhanNo ratings yet
- Multiple Choice QuestionsDocument3 pagesMultiple Choice QuestionsBiph BiphNo ratings yet
- Multiple Choice Questions: Use of Ultrasound in Chronic Pain Medicine. Part 1: Neuraxial and Sympathetic BlocksDocument4 pagesMultiple Choice Questions: Use of Ultrasound in Chronic Pain Medicine. Part 1: Neuraxial and Sympathetic BlocksTesfa MariayamNo ratings yet
- Multiple Choice Questions: Continuing Education in Anaesthesia, Critical Care & Pain - Volume 6 Number 3 2006Document3 pagesMultiple Choice Questions: Continuing Education in Anaesthesia, Critical Care & Pain - Volume 6 Number 3 2006Maheen XhykhNo ratings yet
- Multiple Choice Questions: Continuing Education in Anaesthesia, Critical Care & Pain - Volume 6 Number 3 2006Document3 pagesMultiple Choice Questions: Continuing Education in Anaesthesia, Critical Care & Pain - Volume 6 Number 3 2006AatekaNo ratings yet
- Multiple Choice QuestionsDocument3 pagesMultiple Choice QuestionsAppu JhaNo ratings yet
- PIIS1743181617301804Document5 pagesPIIS1743181617301804HEALTH TIPSNo ratings yet
- GP MCQ 4Document4 pagesGP MCQ 4Marta MoreiraNo ratings yet
- BJA Education March 2017 CMEDocument5 pagesBJA Education March 2017 CME房MickeyNo ratings yet
- Multiple Choice Questions: Childhood Obesity and The AnaesthetistDocument5 pagesMultiple Choice Questions: Childhood Obesity and The AnaesthetistTanishka GargNo ratings yet
- BJAEd March 2018 MCQs PDFDocument5 pagesBJAEd March 2018 MCQs PDFduncanNo ratings yet
- Multiple Choice Questions: Traumatic Brain Injury: An Evidence-Based Review of ManagementDocument5 pagesMultiple Choice Questions: Traumatic Brain Injury: An Evidence-Based Review of Managementaftab alamNo ratings yet
- Multiple Choice Questions on Abdominal Pain, Awake Intubation, and Airway TrainingDocument7 pagesMultiple Choice Questions on Abdominal Pain, Awake Intubation, and Airway TrainingAhmed Ben BellaNo ratings yet
- GP MCQ 11Document4 pagesGP MCQ 11Marta MoreiraNo ratings yet
- Multiple Choice Questions: Diagnosis of DeathDocument3 pagesMultiple Choice Questions: Diagnosis of DeathFaheem AfridiNo ratings yet
- Multiple Choice Questions: Preoperative Cardiopulmonary Exercise TestingDocument2 pagesMultiple Choice Questions: Preoperative Cardiopulmonary Exercise TestingdeadbysunriseeNo ratings yet
- Answers to Cbt Mock Test 1Document12 pagesAnswers to Cbt Mock Test 1odetundesamuelinoNo ratings yet
- GP MCQ 5Document4 pagesGP MCQ 5Marta MoreiraNo ratings yet
- 1'121Document5 pages1'121rakeeb qadriNo ratings yet
- AIIMS (BIO.) - 2004: 1 Dr. Arvind'S Biology ClassesDocument6 pagesAIIMS (BIO.) - 2004: 1 Dr. Arvind'S Biology ClassesayanavNo ratings yet
- GP MCQ 7Document4 pagesGP MCQ 7Marta MoreiraNo ratings yet
- Guyton 테뱅 (3) jkl PDFDocument1 pageGuyton 테뱅 (3) jkl PDFᄋᄋᄋNo ratings yet
- Mku 006Document5 pagesMku 006Moustafa HammadNo ratings yet
- Multiple Choice QuestionsDocument2 pagesMultiple Choice QuestionsAnil SharmaNo ratings yet
- GP MCQ 8Document4 pagesGP MCQ 8Marta MoreiraNo ratings yet
- Carigie's Neuroanatomy of the RatFrom EverandCarigie's Neuroanatomy of the RatWolfgang ZemanNo ratings yet
- The Following Scenarios Relate To The LNG-IUS. Pick One Option From The Option List. Each Option Can Be Used Once, More Than Once or Not at AllDocument2 pagesThe Following Scenarios Relate To The LNG-IUS. Pick One Option From The Option List. Each Option Can Be Used Once, More Than Once or Not at AllDr.Marva YusafzaiNo ratings yet
- MRCOG Short Answer Questions September 2013Document1 pageMRCOG Short Answer Questions September 2013Dr.Marva YusafzaiNo ratings yet
- Understanding Alloimmune Disorders of PregnancyDocument46 pagesUnderstanding Alloimmune Disorders of PregnancyDr.Marva YusafzaiNo ratings yet
- Clinical management investigations and diagnosesDocument8 pagesClinical management investigations and diagnosesDr.Marva YusafzaiNo ratings yet
- Clinical management investigations and diagnosesDocument8 pagesClinical management investigations and diagnosesDr.Marva YusafzaiNo ratings yet
- RCOG Cardiac Disease and Pregnancy PDFDocument18 pagesRCOG Cardiac Disease and Pregnancy PDFSteven SetioNo ratings yet
- MedHome Medical Disorders MOCKDocument4 pagesMedHome Medical Disorders MOCKDr.Marva YusafzaiNo ratings yet
- Notes From Internet: Interesting ThingsDocument3 pagesNotes From Internet: Interesting ThingsDr.Marva YusafzaiNo ratings yet
- MedHome Medical Disorders MOCKDocument4 pagesMedHome Medical Disorders MOCKDr.Marva YusafzaiNo ratings yet
- Oppenheim J.J., Feldmann M. - Introduction To The Role of Cytokines in Innate Host Defense and Adaptive Immunity (2000) PDFDocument18 pagesOppenheim J.J., Feldmann M. - Introduction To The Role of Cytokines in Innate Host Defense and Adaptive Immunity (2000) PDFHesbon MomanyiNo ratings yet
- Nanotech MedDocument12 pagesNanotech MedDaphane Kate AureadaNo ratings yet
- Penanganan Nyeri Kanker Dengan OksikodonDocument26 pagesPenanganan Nyeri Kanker Dengan OksikodonMuhammad ArifNo ratings yet
- Artificial Pancreas Technology Offers Hope For Childhood DiabetesDocument11 pagesArtificial Pancreas Technology Offers Hope For Childhood DiabetesDiana PeñalozaNo ratings yet
- Graduate School Application Essay ExamplesDocument8 pagesGraduate School Application Essay Examplesafabeaida100% (2)
- Desiree Anggia LAPAKHIR2021 DrDesiree DosenMuda KedokteranDocument48 pagesDesiree Anggia LAPAKHIR2021 DrDesiree DosenMuda KedokteranWahyu IndraNo ratings yet
- Restorative & Alternative Medicine: Gaurang JoshiDocument1 pageRestorative & Alternative Medicine: Gaurang JoshiKhushi PansuriaNo ratings yet
- Ra 6969Document86 pagesRa 6969Kit BontilaoNo ratings yet
- PHD Thesis in Prevalence of AsthmaDocument7 pagesPHD Thesis in Prevalence of Asthmabk3q07k5100% (1)
- Salsify: Scientific Name and IntroductionDocument3 pagesSalsify: Scientific Name and IntroductionLeontin LeonNo ratings yet
- Antihistamine: I. HistoryDocument6 pagesAntihistamine: I. HistoryAnaliza Kitongan LantayanNo ratings yet
- Generador Marcapaso Osypka Pace101h IfuDocument35 pagesGenerador Marcapaso Osypka Pace101h IfuJordan BonnettNo ratings yet
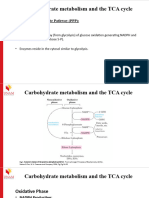
- Carbohydrate Metabolism TCA Cycle - (PPP and Glycogen Metabolism)Document17 pagesCarbohydrate Metabolism TCA Cycle - (PPP and Glycogen Metabolism)Frolian MichaelNo ratings yet
- LILLE FRANCE Trip Report-MajaliwaDocument4 pagesLILLE FRANCE Trip Report-MajaliwaMajaliwa TungarazaNo ratings yet
- Pau Perez - Trauma, Culpa, Duelo - PsicoterapiaDocument18 pagesPau Perez - Trauma, Culpa, Duelo - PsicoterapiaRonaldoCainãNo ratings yet
- ch14 Allostery Problems 6-18-11Document9 pagesch14 Allostery Problems 6-18-11Gary YuNo ratings yet
- Childhood Atopic Dermatitis: Current Developments, Treatment Approaches, and Future ExpectationsDocument22 pagesChildhood Atopic Dermatitis: Current Developments, Treatment Approaches, and Future Expectationsyenny handayani sihiteNo ratings yet
- Kelsey Camangian: August 2019 - PresentDocument1 pageKelsey Camangian: August 2019 - Presentapi-583563266No ratings yet
- Hair NailsDocument4 pagesHair Nailsapi-26570979No ratings yet
- Ravi Home Tutions: 1 Maek Test 1Document22 pagesRavi Home Tutions: 1 Maek Test 1Silva scary svNo ratings yet
- Steps To Take After Receiving Offer LetterDocument5 pagesSteps To Take After Receiving Offer LetterNal ChowdhuryNo ratings yet