You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (842)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5806)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Lesson 4-Uniform Hospital Discharge Data SetDocument14 pagesLesson 4-Uniform Hospital Discharge Data SetSwamyNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- IPM in Healthcare & Hospitals: 10 Step Guide To Implementing An Integrated Pest Management ProgramDocument11 pagesIPM in Healthcare & Hospitals: 10 Step Guide To Implementing An Integrated Pest Management Programver_at_workNo ratings yet
- Definition, Goals, Scope, Core Values, Principles of Social WorkDocument42 pagesDefinition, Goals, Scope, Core Values, Principles of Social WorkChristina Bonachita100% (1)
- ERP BROCHURE HealthcareDocument18 pagesERP BROCHURE Healthcareslc lcb100% (1)
- Scholarly Capstone PaperDocument7 pagesScholarly Capstone Paperapi-546216628No ratings yet
- Ashley Dibble - ResumeDocument1 pageAshley Dibble - Resumeapi-546216628No ratings yet
- Boardman High SchoolDocument4 pagesBoardman High Schoolapi-546216628No ratings yet
- Research PosterDocument1 pageResearch Posterapi-546216628No ratings yet
- Ways To Improve Self-Esteem BrochureDocument2 pagesWays To Improve Self-Esteem Brochureapi-546216628No ratings yet
- Cesarean Delivery of The Obese Woman - UpToDateDocument25 pagesCesarean Delivery of The Obese Woman - UpToDateBárbara JunqueiraNo ratings yet
- Radiofrequency Cetap eDocument4 pagesRadiofrequency Cetap ematameaNo ratings yet
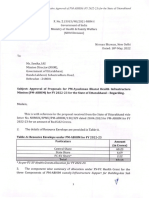
- Uttarakhand Pm-Abhim Rop Fy 2022-23Document8 pagesUttarakhand Pm-Abhim Rop Fy 2022-23Team Frank AmritNo ratings yet
- Session 0 - Cervical Cancer Screening and Treatment - Course Overview-REVIEWEDDocument16 pagesSession 0 - Cervical Cancer Screening and Treatment - Course Overview-REVIEWEDFaraaz SokwalaNo ratings yet
- Chickenpox (Varicella) : What Is Chickenpox? What Are The Symptoms of Chickenpox?Document3 pagesChickenpox (Varicella) : What Is Chickenpox? What Are The Symptoms of Chickenpox?Helga Yoan Ladymeyer TimbayoNo ratings yet
- Alberta Health Act Report 2010Document38 pagesAlberta Health Act Report 2010The Globe and MailNo ratings yet
- Start TriageDocument29 pagesStart TriageSyifa FatiyaNo ratings yet
- A Rare Case of Puerperal Uterine Inversion and Literature ReviewDocument3 pagesA Rare Case of Puerperal Uterine Inversion and Literature ReviewIJAR JOURNALNo ratings yet
- TMP - 12206 AnnualReport14 15 709362705Document213 pagesTMP - 12206 AnnualReport14 15 709362705shakilsaiNo ratings yet
- Upaya Mencegah Malpraktek Dalam Bidang FetomaternalDocument30 pagesUpaya Mencegah Malpraktek Dalam Bidang FetomaternalSurya PratamaNo ratings yet
- Activity HLT EntrepDocument4 pagesActivity HLT EntrepMaria Chrislyn Marcos GenorgaNo ratings yet
- Nursing Theories and TheoristsDocument22 pagesNursing Theories and TheoristsJR Rolf NeuqeletNo ratings yet
- 225 DIV1 5503623 Personal+SpecificationDocument28 pages225 DIV1 5503623 Personal+SpecificationDr Pranesh BalasubramaniamNo ratings yet
- WockhardtDocument22 pagesWockhardtArpit GuptaNo ratings yet
- Who Expert Committe On Drug DependenceDocument266 pagesWho Expert Committe On Drug DependenceAlcione Ferreira SáNo ratings yet
- FORM 2E: Health Plan Implementation For: Maternal Health: Post-Partum CareDocument2 pagesFORM 2E: Health Plan Implementation For: Maternal Health: Post-Partum CarePaul Mark PilarNo ratings yet
- Assignment OverviewThis Assignment Is Intended To Demonstrate Your Comprehension ofDocument2 pagesAssignment OverviewThis Assignment Is Intended To Demonstrate Your Comprehension ofscott harryNo ratings yet
- Thyrocare PrezDocument18 pagesThyrocare PrezDr Amit RangnekarNo ratings yet
- Sri Devaraj Urs Medical CollegeDocument1 pageSri Devaraj Urs Medical CollegeRakeshKumar1987No ratings yet
- SDH Customized NQAS Checklists TN 27.12.2021Document165 pagesSDH Customized NQAS Checklists TN 27.12.2021saravananNo ratings yet
- Caucasus International UniversityDocument10 pagesCaucasus International UniversityRohit SolankiNo ratings yet
- Preoperative FastingDocument5 pagesPreoperative FastingsilviaemohNo ratings yet
- Medi r2 Cutoff GDocument15 pagesMedi r2 Cutoff GSirish S ZakNo ratings yet
- National Healthy Lifestyle Campaign RationaleDocument9 pagesNational Healthy Lifestyle Campaign RationaleLea TanNo ratings yet
- CaNaMed 2022 - Versiunea 04.11.2021Document266 pagesCaNaMed 2022 - Versiunea 04.11.2021Claudia BlmNo ratings yet
- Second Admission List Rematching PG 2024Document17 pagesSecond Admission List Rematching PG 2024amit996No ratings yet