You might also like
- Applied Surface Science Advances: Abubakar Musa Yola, Jack Campbell, Dmitry VolodkinDocument17 pagesApplied Surface Science Advances: Abubakar Musa Yola, Jack Campbell, Dmitry VolodkinGeorge LazarNo ratings yet
- Experimental and Numerical Investigation of Evaporating Fuel Films IncombustionDocument30 pagesExperimental and Numerical Investigation of Evaporating Fuel Films IncombustionGeorge LazarNo ratings yet
- Journal Pre-Proof: Advances in Climate Change ResearchDocument32 pagesJournal Pre-Proof: Advances in Climate Change ResearchGeorge LazarNo ratings yet
- Retrospective Diagnosis of Malignant Struma Ovarii After Discovery of PulmonaryDocument17 pagesRetrospective Diagnosis of Malignant Struma Ovarii After Discovery of PulmonaryGeorge LazarNo ratings yet
- Applied Surface Science Advances: Zahra Haydari, Dawood Elhamifar, Masoumeh Shaker, Meysam NorouziDocument8 pagesApplied Surface Science Advances: Zahra Haydari, Dawood Elhamifar, Masoumeh Shaker, Meysam NorouziGeorge LazarNo ratings yet
- 1 s2.0 S207815201630044X MainDocument7 pages1 s2.0 S207815201630044X Mainwidyah ristantiNo ratings yet
- Applied Surface Science Advances: SciencedirectDocument2 pagesApplied Surface Science Advances: SciencedirectGeorge LazarNo ratings yet
- Applied Surface Science Advances: Seema, Pooja Gupta, Dileep Kumar, V.R. Reddy, Mukul GuptaDocument6 pagesApplied Surface Science Advances: Seema, Pooja Gupta, Dileep Kumar, V.R. Reddy, Mukul GuptaGeorge LazarNo ratings yet
- 1 s2.0 S2078152016300724 MainDocument7 pages1 s2.0 S2078152016300724 Mainwidyah ristantiNo ratings yet
- Applied Surface Science Advances: Ioan BâldeaDocument7 pagesApplied Surface Science Advances: Ioan BâldeaGeorge LazarNo ratings yet
- Arsenic and Cadmium Contamination in WaterDocument17 pagesArsenic and Cadmium Contamination in WaterLaura Gomez SanchezNo ratings yet
- The Total Face Irregularity Strength of Some Plane GraphsDocument8 pagesThe Total Face Irregularity Strength of Some Plane GraphsGeorge LazarNo ratings yet
- Structure of Extracellular PolysaccharidesDocument8 pagesStructure of Extracellular PolysaccharidesLaura Gomez SanchezNo ratings yet
- Revealing The Electrocatalytic Behaviour by A Novel Rotating Ring-Disc Elec TrodeDocument16 pagesRevealing The Electrocatalytic Behaviour by A Novel Rotating Ring-Disc Elec TrodeGeorge LazarNo ratings yet
- Achievements in The Life Sciences: Mahmodul Hasan SohelDocument12 pagesAchievements in The Life Sciences: Mahmodul Hasan Sohelsameer sahaanNo ratings yet
- Universal Remote Control Systems For Domestic Devices Using Radio Frequency Waves 2014 AASRI ProcediaDocument4 pagesUniversal Remote Control Systems For Domestic Devices Using Radio Frequency Waves 2014 AASRI ProcediaAnonymous VIHgLt5No ratings yet
- Bleb Formation in Human Fibrosarcoma HT1080 Cancer Cell L 2016 AchievementsDocument11 pagesBleb Formation in Human Fibrosarcoma HT1080 Cancer Cell L 2016 Achievementswidyah ristantiNo ratings yet
- Upgrading of Biomass Fast Pyrolysis Oil Over A Moving Bed of Coal CharDocument30 pagesUpgrading of Biomass Fast Pyrolysis Oil Over A Moving Bed of Coal CharGeorge LazarNo ratings yet
- 1 s2.0 S2212671614001061 MainDocument6 pages1 s2.0 S2212671614001061 MainEnormous BeastNo ratings yet
- Abdkkhdkh FdvevDocument7 pagesAbdkkhdkh FdvevSudipNo ratings yet
- The Specific Nature of Chemical Composition of Water From Volcanic Lakes Based On Bali Case StudyDocument5 pagesThe Specific Nature of Chemical Composition of Water From Volcanic Lakes Based On Bali Case StudyGeorge LazarNo ratings yet
- On The Topological Matrix and Topological IndicesDocument7 pagesOn The Topological Matrix and Topological IndicesGeorge LazarNo ratings yet
- A New Texture Analysis Approach For Iris Recognition 2014 AASRI ProcediaDocument6 pagesA New Texture Analysis Approach For Iris Recognition 2014 AASRI ProcediaAnonymous VIHgLt5No ratings yet
- 1 s2.0 S221267161400105X Main PDFDocument6 pages1 s2.0 S221267161400105X Main PDFEnormous BeastNo ratings yet
- A New Matrix Representation for Multidigraph Spectral AnalysisDocument14 pagesA New Matrix Representation for Multidigraph Spectral AnalysisGeorge LazarNo ratings yet
- Release and Transport of Toxic, Mobile Organic Compounds (Formaldehyde and Phenols) On An Arctic GlacierDocument5 pagesRelease and Transport of Toxic, Mobile Organic Compounds (Formaldehyde and Phenols) On An Arctic GlacierGeorge LazarNo ratings yet
- Journal Pre-Proof: Case Studies in Chemical and Environmental EngineeringDocument26 pagesJournal Pre-Proof: Case Studies in Chemical and Environmental EngineeringGeorge LazarNo ratings yet
- Sorptive Removal of Malachite Green Dye by Activated Charcoal - Process Optimization, Kinetic, and Thermodynamic EvaluationDocument21 pagesSorptive Removal of Malachite Green Dye by Activated Charcoal - Process Optimization, Kinetic, and Thermodynamic EvaluationGeorge LazarNo ratings yet
- On How Mild Oxidation Affects The Structure of Carbons Comparative Analysis by DifferentDocument27 pagesOn How Mild Oxidation Affects The Structure of Carbons Comparative Analysis by DifferentGeorge LazarNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Đề Thi Thử Thptqg Môn Tiếng AnhDocument8 pagesĐề Thi Thử Thptqg Môn Tiếng AnhHổCápNo ratings yet
- CFB Gagetown Agent Orange Information Paper Update 1Document6 pagesCFB Gagetown Agent Orange Information Paper Update 1wcfieldsNo ratings yet
- PSYCH 7 Course OutlineDocument4 pagesPSYCH 7 Course OutlineJM FranciscoNo ratings yet
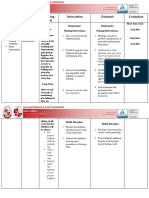
- NCP BathingDocument3 pagesNCP BathingNICOLE TOLENTINONo ratings yet
- Patient Information Guide: AH-QF-FO-07Document35 pagesPatient Information Guide: AH-QF-FO-07jose rajanNo ratings yet
- Shih Tzus: What A Unique Breed!Document5 pagesShih Tzus: What A Unique Breed!Jimmy YauNo ratings yet
- Summary of Consensus Statements On The Diagnosis and Management of COPD in The PhilippinesDocument34 pagesSummary of Consensus Statements On The Diagnosis and Management of COPD in The PhilippinesDivye GuptaNo ratings yet
- How Environment Affects Our HealthDocument4 pagesHow Environment Affects Our HealthMajo PerezNo ratings yet
- Summary of High-Quality CPR Components For BLS ProvidersDocument1 pageSummary of High-Quality CPR Components For BLS ProvidersPhilippe Ceasar C. BascoNo ratings yet
- 265 23686 1 10 20190515 PDFDocument10 pages265 23686 1 10 20190515 PDFanggiliaNo ratings yet
- Stunting in Children Under FiveDocument11 pagesStunting in Children Under FiveIndah Tri AntikaNo ratings yet
- Munjir Abdullah - Project On PBH101Document4 pagesMunjir Abdullah - Project On PBH101Munjir Abdullah 2112217030No ratings yet
- Can Positive or Negative Thoughts and Emotions Affect Your BodyDocument10 pagesCan Positive or Negative Thoughts and Emotions Affect Your BodyAlia MaisarahNo ratings yet
- Medical Treatment of Aortic Stenosis: in DepthDocument19 pagesMedical Treatment of Aortic Stenosis: in DepthAlexandra NalgomNo ratings yet
- The Future of Positive Psychology: A Declaration of IndependenceDocument17 pagesThe Future of Positive Psychology: A Declaration of IndependenceEbonnie DiazNo ratings yet
- First Aid and Water Safety Course PlanDocument2 pagesFirst Aid and Water Safety Course PlanTea AnnNo ratings yet
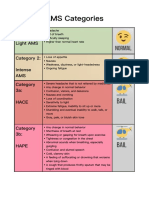
- AMS Symptoms and CategoriesDocument1 pageAMS Symptoms and CategoriesyyggvcNo ratings yet
- NYCOSH Letter To DOB Re: OSHA Card Arrests 10262015Document2 pagesNYCOSH Letter To DOB Re: OSHA Card Arrests 10262015Monica NovoaNo ratings yet
- Mental Health EssayDocument2 pagesMental Health EssayROHITNo ratings yet
- Effect of Custom-Made Footwear On Foot Ulcer Recurrence in DiabetesDocument8 pagesEffect of Custom-Made Footwear On Foot Ulcer Recurrence in DiabetesJosé MorenoNo ratings yet
- Pdoc - Vivicit LeafletDocument1 pagePdoc - Vivicit Leafletahmedrijone2014No ratings yet
- FULL Download Ebook PDF Introduction To One Health An Interdisciplinary Approach To Planetary Health PDF EbookDocument41 pagesFULL Download Ebook PDF Introduction To One Health An Interdisciplinary Approach To Planetary Health PDF Ebookvalerie.iribarren889100% (35)
- Hsg245 - Investigating Accident & IncidentsDocument89 pagesHsg245 - Investigating Accident & IncidentsJohn MaynardNo ratings yet
- Agni Dagdha. Group-T Patients Were Treated With Indigenous Drugs and Group-C PatientsDocument14 pagesAgni Dagdha. Group-T Patients Were Treated With Indigenous Drugs and Group-C PatientsKrishnaNo ratings yet
- With Answers No RationaleDocument41 pagesWith Answers No RationaleronnaxNo ratings yet
- MukokelDocument3 pagesMukokeljulietNo ratings yet
- Bactomin Product MonographDocument43 pagesBactomin Product MonographVivek AlaiNo ratings yet
- LabaidDocument29 pagesLabaidBorhan UddinNo ratings yet
- Easy Read AI Disabilities ReportDocument65 pagesEasy Read AI Disabilities ReportNi Putu Tya SuindrayaniNo ratings yet
- My Courses: Home UGRD-PHYED6101-2113T Week 2: Health-Related Fitness Components Prelim Quiz 1Document4 pagesMy Courses: Home UGRD-PHYED6101-2113T Week 2: Health-Related Fitness Components Prelim Quiz 1Miguel Angelo GarciaNo ratings yet