You might also like
- A Study On Management of Bothbones Forearm Fractures With Dynamic Compression PlateDocument5 pagesA Study On Management of Bothbones Forearm Fractures With Dynamic Compression PlateIOSRjournalNo ratings yet
- Brief Resume of Intended WorkDocument7 pagesBrief Resume of Intended WorkNavin ChandarNo ratings yet
- Catastrophic Talar Bone Loss From High Velocity Trauma Treated With Structural Tricorticate Fibula Autograft Compression Frame and Midfoot Distraction ArthroplastyDocument9 pagesCatastrophic Talar Bone Loss From High Velocity Trauma Treated With Structural Tricorticate Fibula Autograft Compression Frame and Midfoot Distraction ArthroplastyAthenaeum Scientific PublishersNo ratings yet
- Distal Tibia Paper 2Document6 pagesDistal Tibia Paper 2Rajib DebnathNo ratings yet
- Intra-Articular Fractures of Distal Humerus Managed With Anatomic Pre-Contoured Plates Via Olecranon Osteotomy ApproachDocument7 pagesIntra-Articular Fractures of Distal Humerus Managed With Anatomic Pre-Contoured Plates Via Olecranon Osteotomy ApproachIJAR JOURNALNo ratings yet
- Ligamentotaxis in The Intraarticular and Juxta Articular Fracture of WristDocument3 pagesLigamentotaxis in The Intraarticular and Juxta Articular Fracture of WristIOSRjournalNo ratings yet
- Clinical Analysis of The Frosch Approach in The Treatment of Posterolateral Tibial Plateau Fractures Combined With Lateral Tibial Plateau FracturesDocument11 pagesClinical Analysis of The Frosch Approach in The Treatment of Posterolateral Tibial Plateau Fractures Combined With Lateral Tibial Plateau FracturesraynaldidjohariofcNo ratings yet
- Distal Humeral Fractures-Current Concepts PDFDocument11 pagesDistal Humeral Fractures-Current Concepts PDFRina AlvionitaNo ratings yet
- Comparative Outcome of Short Proximal Femoral Nail Versus Proximal Femoral Locking Compression Plate in The Management of Unstable Trochanteric FracturesDocument8 pagesComparative Outcome of Short Proximal Femoral Nail Versus Proximal Femoral Locking Compression Plate in The Management of Unstable Trochanteric FracturesAthenaeum Scientific PublishersNo ratings yet
- Stabilization of Distal Humerus Fractures by Precontoured Bi-Condylar Plating in A 90-90 PatternDocument5 pagesStabilization of Distal Humerus Fractures by Precontoured Bi-Condylar Plating in A 90-90 PatternmayNo ratings yet
- Case Series of All-Arthroscopic Treatment For Terrible Triad of The Elbow: Indications and Clinical OutcomesDocument10 pagesCase Series of All-Arthroscopic Treatment For Terrible Triad of The Elbow: Indications and Clinical OutcomesdorfynatorNo ratings yet
- Abstracts de Publicaciones Sobre Pilón TibialDocument15 pagesAbstracts de Publicaciones Sobre Pilón TibialAyler AguilarNo ratings yet
- Kulkarni2012 PDFDocument7 pagesKulkarni2012 PDFAby SuryaNo ratings yet
- Assesment of Functional Outcome of Dual Plating For Comminuted Distal Femur FractureDocument13 pagesAssesment of Functional Outcome of Dual Plating For Comminuted Distal Femur FractureIJAR JOURNALNo ratings yet
- Analysis of Surgical Management of Proximal Humeral FracturesDocument5 pagesAnalysis of Surgical Management of Proximal Humeral FracturesRhizka djitmauNo ratings yet
- Operative Treatment of Peritrochanteric Osteoporotic Fractures With Proximal Femur Locking Compression Plate A Consecutive StudyDocument6 pagesOperative Treatment of Peritrochanteric Osteoporotic Fractures With Proximal Femur Locking Compression Plate A Consecutive StudyAthenaeum Scientific PublishersNo ratings yet
- Cas Repot DruDocument8 pagesCas Repot DruKrishna CaitanyaNo ratings yet
- Paper 1 Vinothkumar-1Document5 pagesPaper 1 Vinothkumar-1SK BONE & JOINT CARE DPINo ratings yet
- Treatment of Periprosthetic Knee Fractures With Plate and Screws and With Retrograde Intramedullary Nail Indications Limits and Medium Term Follow UpDocument22 pagesTreatment of Periprosthetic Knee Fractures With Plate and Screws and With Retrograde Intramedullary Nail Indications Limits and Medium Term Follow UpAthenaeum Scientific PublishersNo ratings yet
- Utility and Outcomes of Locking Compression Plates in Distal Femoral FracturesDocument7 pagesUtility and Outcomes of Locking Compression Plates in Distal Femoral FractureskhusnulNo ratings yet
- Treatment Distal Radius Fracture With Volar Buttre PDFDocument5 pagesTreatment Distal Radius Fracture With Volar Buttre PDFZia Ur RehmanNo ratings yet
- Paper 38Document6 pagesPaper 38Dr Vineet KumarNo ratings yet
- Thesis Umesh A2z.doc Final Thesis CorrectionDocument79 pagesThesis Umesh A2z.doc Final Thesis CorrectionRakesh JhaNo ratings yet
- Ma 2021Document6 pagesMa 2021bigben9262No ratings yet
- Review of Intramedullary Interlocked Nailing in Closed & Grade I Open Tibial FracturesDocument4 pagesReview of Intramedullary Interlocked Nailing in Closed & Grade I Open Tibial FracturesInternational Organization of Scientific Research (IOSR)No ratings yet
- Com Minuted Patellar FractureDocument3 pagesCom Minuted Patellar FractureAhmet EkinciNo ratings yet
- Osteochondral Multiple Autograft Transfer (OMAT) For The Treatment of Cartilage Defects in The Knee JointDocument4 pagesOsteochondral Multiple Autograft Transfer (OMAT) For The Treatment of Cartilage Defects in The Knee JointAnil SoodNo ratings yet
- Marcheggianimuccioli 2019Document12 pagesMarcheggianimuccioli 2019Ghusun MadaniNo ratings yet
- Aps 39 345Document9 pagesAps 39 345isabelNo ratings yet
- He 2019Document10 pagesHe 2019Rashif AkmalNo ratings yet
- Anterior Tibial Spine ACL Avulsion Fracture TreateDocument5 pagesAnterior Tibial Spine ACL Avulsion Fracture TreateDyah PurwitaNo ratings yet
- Li 2018Document6 pagesLi 2018Lorena ValderramaNo ratings yet
- Complications and Outcomes of The Transfibular Approach For Posterolateral Fractures of The Tibial Plateau PDFDocument19 pagesComplications and Outcomes of The Transfibular Approach For Posterolateral Fractures of The Tibial Plateau PDFSergio Tomas Cortés MoralesNo ratings yet
- J Clin Orthop Trauma 2021 20 101480Document8 pagesJ Clin Orthop Trauma 2021 20 101480Lucas SanchezNo ratings yet
- 02 - Krishna ReddyDocument7 pages02 - Krishna ReddyAnonymous ygv5h1MRNo ratings yet
- Anehosur Et Al 2020 Concepts and Challenges in The Surgical Management of Edentulous Mandible Fractures A Case SeriesDocument7 pagesAnehosur Et Al 2020 Concepts and Challenges in The Surgical Management of Edentulous Mandible Fractures A Case SeriesHenry Adhy SantosoNo ratings yet
- 1005-04eDocument6 pages1005-04eHitham El ShahatNo ratings yet
- Treatment of AO/OTA 31-A3 Intertrochanteric Femoral Fractures With A Percutaneous Compression PlateDocument7 pagesTreatment of AO/OTA 31-A3 Intertrochanteric Femoral Fractures With A Percutaneous Compression PlateNurul AiniNo ratings yet
- Fsurg 10 1085636Document7 pagesFsurg 10 1085636zxiaoxing087No ratings yet
- Xray vs CT for Elbow FracturesDocument5 pagesXray vs CT for Elbow FracturesICNo ratings yet
- Distal Femur Fractures Fixation by Locking Compression Plate-Assessment of Outcome by Rasmussens Functional Knee ScoreDocument7 pagesDistal Femur Fractures Fixation by Locking Compression Plate-Assessment of Outcome by Rasmussens Functional Knee ScoreIJAR JOURNALNo ratings yet
- Closed Intra - Articular Fractures of The Distal End of Humerus Surgically Treated by Trans - Olecranon Approach Using The Chevron OsteotomyDocument4 pagesClosed Intra - Articular Fractures of The Distal End of Humerus Surgically Treated by Trans - Olecranon Approach Using The Chevron OsteotomyIJAR JOURNALNo ratings yet
- EgyptOrthopJ50145-8454425 232904tgtDocument6 pagesEgyptOrthopJ50145-8454425 232904tgtAzmi FarhadiNo ratings yet
- Ipsilateral Fracture of Femur and Tibia, Treatment and Functional OutcomeDocument3 pagesIpsilateral Fracture of Femur and Tibia, Treatment and Functional OutcomeichkhuyNo ratings yet
- 97-506-1 Segundo CynDocument6 pages97-506-1 Segundo CynGalletita De JengibreNo ratings yet
- Conservative Treatment of Medial Shaft Clavicle Fracture With Borderline Criteria A Case ReportDocument9 pagesConservative Treatment of Medial Shaft Clavicle Fracture With Borderline Criteria A Case ReportAthenaeum Scientific PublishersNo ratings yet
- Flexible 3D Laparoscopic Assisted Reduction andDocument9 pagesFlexible 3D Laparoscopic Assisted Reduction andgevowo3277No ratings yet
- Ankle Arthrodesis For Pilon FractureDocument12 pagesAnkle Arthrodesis For Pilon FracturestudmmaNo ratings yet
- Mallet Finger Suturing TechniqueDocument5 pagesMallet Finger Suturing TechniqueSivaprasath JaganathanNo ratings yet
- Sliding Bone Graft JournalDocument3 pagesSliding Bone Graft Journalapi-310305222No ratings yet
- Acl Bone Graft With Mini ArthrotomyDocument9 pagesAcl Bone Graft With Mini Arthrotomypaper coe medanNo ratings yet
- Surgical Outcomes After Traumatic Open Knee Dislocation: Ó Springer-Verlag 2009Document6 pagesSurgical Outcomes After Traumatic Open Knee Dislocation: Ó Springer-Verlag 2009agus sukarnaNo ratings yet
- Bahan Jurnal Neglected Fractures of FemurDocument5 pagesBahan Jurnal Neglected Fractures of Femurgulamg21No ratings yet
- Ortho ArticleDocument2 pagesOrtho ArticleSamantha Dela Paz100% (1)
- An Acetabular Fracture With A Series of Complications and Their Solutions A Notable Case ReportDocument6 pagesAn Acetabular Fracture With A Series of Complications and Their Solutions A Notable Case ReportAthenaeum Scientific PublishersNo ratings yet
- Morbidity and Total Knee Arthroplasty As A Long Term Sequela of Tibial Plateau FracturesDocument8 pagesMorbidity and Total Knee Arthroplasty As A Long Term Sequela of Tibial Plateau FracturesAthenaeum Scientific PublishersNo ratings yet
- Kim 2019Document5 pagesKim 2019Krishna CaitanyaNo ratings yet
- Cartilage Injury of the Knee: State-of-the-Art Treatment and ControversiesFrom EverandCartilage Injury of the Knee: State-of-the-Art Treatment and ControversiesAaron J. KrychNo ratings yet
- Unicompartmental Knee Arthroplasty: Indications, Surgical Techniques and ComplicationsFrom EverandUnicompartmental Knee Arthroplasty: Indications, Surgical Techniques and ComplicationsTad L. GerlingerNo ratings yet
- Acetabular Fractures in Older Patients: Assessment and ManagementFrom EverandAcetabular Fractures in Older Patients: Assessment and ManagementTheodore T. MansonNo ratings yet
- Understanding Doctoral Nursing Students' Experiences of Blended LearningDocument8 pagesUnderstanding Doctoral Nursing Students' Experiences of Blended LearningZilbran BerontaxNo ratings yet
- Self-Directed Learning Methods On Nursing Education: A Literature ReviewDocument8 pagesSelf-Directed Learning Methods On Nursing Education: A Literature ReviewZilbran BerontaxNo ratings yet
- Geriatric Anxiety Scale v2.0 FINALDocument2 pagesGeriatric Anxiety Scale v2.0 FINALpujipurwaningsih67% (3)
- Self-directed Learning Skills in Honduras Compared to the United StatesDocument19 pagesSelf-directed Learning Skills in Honduras Compared to the United StatesZilbran BerontaxNo ratings yet
- Role of Bacterial Infections in Pancreatic Cancer: ReviewDocument5 pagesRole of Bacterial Infections in Pancreatic Cancer: ReviewZilbran BerontaxNo ratings yet
- Validation of Self-Directed LearningDocument11 pagesValidation of Self-Directed LearningZilbran BerontaxNo ratings yet
- Bencana 1Document14 pagesBencana 1Andhi SNo ratings yet
- Speech and Language Therapy For Aphasia Following Subacute StrokeDocument6 pagesSpeech and Language Therapy For Aphasia Following Subacute StrokeZilbran BerontaxNo ratings yet
- Bates-Jensen Wound Assessment Tool (BWAT)Document4 pagesBates-Jensen Wound Assessment Tool (BWAT)Jamie OngNo ratings yet
- LR SDL - 7. OutDocument7 pagesLR SDL - 7. OutAnggita Nandya ArdiatiNo ratings yet
- Transtition To Blended LearningDocument17 pagesTranstition To Blended LearningZilbran BerontaxNo ratings yet
- The Impact of The Learning Contract On Self-Directed LearningDocument5 pagesThe Impact of The Learning Contract On Self-Directed LearningZilbran BerontaxNo ratings yet
- The Self-Directed Learning Readiness Level of The Undergraduate Students of Midwife and Nurse in Terms of Sustainability in Nursing and Midwifery EducationDocument14 pagesThe Self-Directed Learning Readiness Level of The Undergraduate Students of Midwife and Nurse in Terms of Sustainability in Nursing and Midwifery EducationZilbran BerontaxNo ratings yet
- The Impact of Blended Teaching On Knowledge, Satisfaction, and Self-Directed Learning in Nursing Undergraduates: A Randomized, Controlled TrialDocument7 pagesThe Impact of Blended Teaching On Knowledge, Satisfaction, and Self-Directed Learning in Nursing Undergraduates: A Randomized, Controlled TrialJefry ArieNo ratings yet
- Blended Learning (Research Article)Document12 pagesBlended Learning (Research Article)Andrés Espinoza100% (1)
- The Effects of Blended Learning On Knowledge, Skills, and Satisfaction Innursing Students A Meta-AnalysisDocument7 pagesThe Effects of Blended Learning On Knowledge, Skills, and Satisfaction Innursing Students A Meta-AnalysisZilbran BerontaxNo ratings yet
- Simulation Videos Presented in A Blended Learning Platform ToDocument27 pagesSimulation Videos Presented in A Blended Learning Platform ToZilbran BerontaxNo ratings yet
- Measure Nursing Student Self-Directed Learning AbilitiesDocument8 pagesMeasure Nursing Student Self-Directed Learning AbilitiesZilbran BerontaxNo ratings yet
- Self-Directed Learning A Tool For Lifelong LearningDocument15 pagesSelf-Directed Learning A Tool For Lifelong LearningZilbran BerontaxNo ratings yet
- Effect of Self-Directed Learning On Nursing Students' Readiness, Perception and Performance in SudanDocument10 pagesEffect of Self-Directed Learning On Nursing Students' Readiness, Perception and Performance in SudanZilbran BerontaxNo ratings yet
- Effect of Self-Directed Learning On Nursing Students' Readiness, Perception and Performance in SudanDocument10 pagesEffect of Self-Directed Learning On Nursing Students' Readiness, Perception and Performance in SudanZilbran BerontaxNo ratings yet
- Effectiveness of A Self-Directed LearningDocument8 pagesEffectiveness of A Self-Directed LearningZilbran BerontaxNo ratings yet
- Scientific Information System: Network of Scientific Journals From Latin America, The Caribbean, Spain and PortugalDocument12 pagesScientific Information System: Network of Scientific Journals From Latin America, The Caribbean, Spain and PortugalZilbran BerontaxNo ratings yet
- Effect of Blended Learning On Newly Nursing Student's Outcomes Regarding New Trends in Nursing Subject at Ain Shams UniversityDocument9 pagesEffect of Blended Learning On Newly Nursing Student's Outcomes Regarding New Trends in Nursing Subject at Ain Shams UniversityZilbran BerontaxNo ratings yet
- Exploratory Study of The Relationship Between Self-Directed Learning and Academic Performance in A Web - Based Learning EnvironmentDocument11 pagesExploratory Study of The Relationship Between Self-Directed Learning and Academic Performance in A Web - Based Learning EnvironmentZilbran BerontaxNo ratings yet
- Concurrent Validity of Self-Rating Scale ofDocument11 pagesConcurrent Validity of Self-Rating Scale ofZilbran BerontaxNo ratings yet
- Effect of Blended Learning On Newly Nursing Student's Outcomes Regarding New Trends in Nursing Subject at Ain Shams UniversityDocument9 pagesEffect of Blended Learning On Newly Nursing Student's Outcomes Regarding New Trends in Nursing Subject at Ain Shams UniversityZilbran BerontaxNo ratings yet
- Blended Versus Lecture LearningDocument5 pagesBlended Versus Lecture LearningZilbran BerontaxNo ratings yet
- Blended Learning The New Normal and Emerging Technologies PDFDocument16 pagesBlended Learning The New Normal and Emerging Technologies PDFBagas Annas UtomoNo ratings yet
- Blended Learning in High School Chemistry ToDocument11 pagesBlended Learning in High School Chemistry ToZilbran BerontaxNo ratings yet
- Medigrip Sizing ChartDocument1 pageMedigrip Sizing ChartKelly HuntNo ratings yet
- 3E - Agustin, Anne Julia - Group 1 - Case 7,8Document5 pages3E - Agustin, Anne Julia - Group 1 - Case 7,8Anne Julia AgustinNo ratings yet
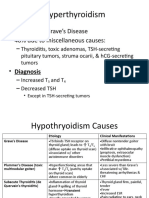
- Graves Disease and Hyperthyroidism Causes 60% of CasesDocument6 pagesGraves Disease and Hyperthyroidism Causes 60% of CasesLeitavia D.No ratings yet
- Addictions: Psychology Assignment Name: Jigyasa Dhingra Class: Xi-FDocument10 pagesAddictions: Psychology Assignment Name: Jigyasa Dhingra Class: Xi-FAN - 11ZZ 963416 Chinguacousy SSNo ratings yet
- Athlete - Rosauro James Rock 2002Document9 pagesAthlete - Rosauro James Rock 2002Avi Auerbach AvilaNo ratings yet
- Nursing Care Analysis of Christopher Hammitt CaseDocument8 pagesNursing Care Analysis of Christopher Hammitt CaseKelly J Wilson0% (1)
- CORDERO Performance Task 5Document1 pageCORDERO Performance Task 5Maria Hilda Vicio AragonNo ratings yet
- The 10 Most Addictive Pain MedicationsDocument17 pagesThe 10 Most Addictive Pain MedicationslabendetNo ratings yet
- NardilDocument4 pagesNardilTemerNo ratings yet
- First Generation Anti-Depressants: TCAs and MAOIsDocument54 pagesFirst Generation Anti-Depressants: TCAs and MAOIssangha_mitra_2No ratings yet
- Injectable Bone Graft and Allograft Bone Chips in The Treatment of Benign Bone LesionDocument8 pagesInjectable Bone Graft and Allograft Bone Chips in The Treatment of Benign Bone LesionIJAR JOURNALNo ratings yet
- PNLMCN Nursing Skills Lab NG/NI Tube Insertion GuideDocument19 pagesPNLMCN Nursing Skills Lab NG/NI Tube Insertion GuideKlare MontefalcoNo ratings yet
- Drug StudyDocument6 pagesDrug StudyIrveen Joy RamirezNo ratings yet
- Program Book11Document1,124 pagesProgram Book11heocon857351No ratings yet
- Health and Disease Status of Thai Pangas, Bangladesh: Pangasius Hypophthalmus Cultured in Rural Ponds of MymensinghDocument3 pagesHealth and Disease Status of Thai Pangas, Bangladesh: Pangasius Hypophthalmus Cultured in Rural Ponds of MymensinghgooedliaNo ratings yet
- Dengue Shock SyndromeDocument17 pagesDengue Shock SyndromehwelpNo ratings yet
- ACETAMINOPHEN DrugStudyDocument2 pagesACETAMINOPHEN DrugStudyERAN MARK ROJASNo ratings yet
- The Child With A Fluid and Electrolyte Alteration: Body Water Is Located in Two Major CompartmentsDocument19 pagesThe Child With A Fluid and Electrolyte Alteration: Body Water Is Located in Two Major CompartmentsAyeza DuaNo ratings yet
- Tumors of The Jaw and Oral MucosaDocument18 pagesTumors of The Jaw and Oral MucosaDaniela LeonteNo ratings yet
- Contemporary PracticesDocument20 pagesContemporary PracticesMichels Garments S.H Nawaz HosieryNo ratings yet
- Wender Utah PDFDocument3 pagesWender Utah PDFFco CanaleNo ratings yet
- Fogsi ChecklistDocument131 pagesFogsi ChecklistParimi VinodNo ratings yet
- DISORDERDocument3 pagesDISORDERMia Grace GarciaNo ratings yet
- 16 Natural Ways To Manage Meniere's Disease SymptomsDocument16 pages16 Natural Ways To Manage Meniere's Disease SymptomsMeseret NegashNo ratings yet
- 1 thePoisonedNeedle PDFDocument432 pages1 thePoisonedNeedle PDFcas100% (4)
- Segaletal 2019GeriatricAnxietyScaleDocument8 pagesSegaletal 2019GeriatricAnxietyScaleMapodettNo ratings yet
- Uterine Rupture and Cervical TearDocument16 pagesUterine Rupture and Cervical Tearsangita patil0% (1)
- Acute GastroenteritisDocument28 pagesAcute GastroenteritisSiergs Smith GervacioNo ratings yet
- Approach To Patient With Endocrine DisordersDocument2 pagesApproach To Patient With Endocrine DisordersSeff CausapinNo ratings yet
- MID Bacteria Charts JkuoDocument17 pagesMID Bacteria Charts Jkuotsukino143100% (2)