You might also like
- Comparison of Tympanometry Results For Probe Tones of 226 HZ and 1000 HZ in NewbornsDocument40 pagesComparison of Tympanometry Results For Probe Tones of 226 HZ and 1000 HZ in NewbornsEkky Rizky MaulanaNo ratings yet
- 10 Therole 20050598Document4 pages10 Therole 20050598DalRiveraPardoNo ratings yet
- Acoustic Reflex Measurement.8Document5 pagesAcoustic Reflex Measurement.8Mehmet ŞahinNo ratings yet
- Physiology of The Auditory SystemDocument47 pagesPhysiology of The Auditory Systemmkct111No ratings yet
- Stethoscope Acoustics and Cervical Auscultation of SwallowingDocument6 pagesStethoscope Acoustics and Cervical Auscultation of SwallowingAnonymous xvlg4m5xLXNo ratings yet
- 09tympanometry ProtocolDocument5 pages09tympanometry ProtocolDalRiveraPardoNo ratings yet
- Experiment 5. Resonance Tube - ReportDocument4 pagesExperiment 5. Resonance Tube - Reportourdreamsandfuture2004No ratings yet
- Jasa537 12323Document7 pagesJasa537 12323عبدالله عليNo ratings yet
- ApuntesssssDocument36 pagesApuntessssstomkimenNo ratings yet
- Characteristics of The Wideband Absorbance of Aco - 2021 - International JournalDocument7 pagesCharacteristics of The Wideband Absorbance of Aco - 2021 - International JournalHung Son TaNo ratings yet
- Baldwin 2006Document11 pagesBaldwin 2006Francisca MayorgaNo ratings yet
- Audiometría Niños y AdultosDocument7 pagesAudiometría Niños y AdultosgeraldinefonoaudioNo ratings yet
- Ultrasonic properties of palm oil and other vegetable oilsDocument8 pagesUltrasonic properties of palm oil and other vegetable oilsBramJanssen76No ratings yet
- Dapus 11 Referat 2Document3 pagesDapus 11 Referat 2Akramanto RidwanNo ratings yet
- Chapter 10 (1) - 2Document34 pagesChapter 10 (1) - 2mahraNo ratings yet
- Ultrasonic Imaging System GuideDocument12 pagesUltrasonic Imaging System GuideKiran Kumar100% (1)
- Radiophysics 29 38 CompDocument188 pagesRadiophysics 29 38 CompMd shamim rezaNo ratings yet
- Presenter: Nuha Haleema Faculty: Dr. Sreedevi N: Electromagnetic Midsagittal Articulography (EMM A)Document46 pagesPresenter: Nuha Haleema Faculty: Dr. Sreedevi N: Electromagnetic Midsagittal Articulography (EMM A)Nuha HaleemaNo ratings yet
- Ultrasonic Diffraction at Different Multiple Slit SystemsDocument5 pagesUltrasonic Diffraction at Different Multiple Slit SystemsJose GalvanNo ratings yet
- Rehab Tech21Document114 pagesRehab Tech21Appas SahaNo ratings yet
- 04 Accel Incline SVDocument4 pages04 Accel Incline SVJuan Carlos De DiosNo ratings yet
- Reflex Measurements: Quick GuideDocument10 pagesReflex Measurements: Quick GuidefilippobNo ratings yet
- Practical Ent AbridgedDocument17 pagesPractical Ent AbridgedAishaNo ratings yet
- Long Term Effects of Surgically Assisted Rapid Maxillary Expansion Without Performing Osteotomy of The Pterygoid PlatesDocument4 pagesLong Term Effects of Surgically Assisted Rapid Maxillary Expansion Without Performing Osteotomy of The Pterygoid PlatesAngélica Valenzuela AndrighiNo ratings yet
- Tes Garpu TalaDocument13 pagesTes Garpu TalaSamuel ChristianNo ratings yet
- Sentiero Desktop Diagnostic - PATH - MEDICAL - GMBHDocument2 pagesSentiero Desktop Diagnostic - PATH - MEDICAL - GMBHKothapalli ChiranjeeviNo ratings yet
- Enraf-Nonius Sonopuls 490B ENDocument12 pagesEnraf-Nonius Sonopuls 490B ENYussuf MuhammadNo ratings yet
- Tympanometry in Clinical Practice: Janet Shanks and Jack ShohetDocument32 pagesTympanometry in Clinical Practice: Janet Shanks and Jack ShohetDiah HayustiningsihNo ratings yet
- McAulay-Quatieri Technique v1Document11 pagesMcAulay-Quatieri Technique v1Kevin DiazNo ratings yet
- Articulo AudiologicosDocument3 pagesArticulo AudiologicosFabian Camelo OtorrinoNo ratings yet
- Hearing LossDocument29 pagesHearing LossKapitan TutanNo ratings yet
- Reliable Measure of Dysphonia - CPPDocument10 pagesReliable Measure of Dysphonia - CPPNatalia BoccoNo ratings yet
- Glissando MechanismsDocument7 pagesGlissando MechanismsJenith Karem Paredes GonzalezNo ratings yet
- Importance of X-rays in Root Canal TherapyDocument36 pagesImportance of X-rays in Root Canal TherapyMonica AmeliaNo ratings yet
- Time-of-Flight Ultrasonic Displacement Sensor TechniquesDocument23 pagesTime-of-Flight Ultrasonic Displacement Sensor Techniquesigoy saputraNo ratings yet
- Fine Structure of Hearing Threshold andDocument15 pagesFine Structure of Hearing Threshold andJuan Sebas Vizuete100% (1)
- Acoustic and Aerodynamic Assessment of VoiceDocument4 pagesAcoustic and Aerodynamic Assessment of VoicesherinNo ratings yet
- PERAN TES ELEKTROAKUSTIK IMITANS DI BIDANG AUDIOLOGIDocument29 pagesPERAN TES ELEKTROAKUSTIK IMITANS DI BIDANG AUDIOLOGIekaNo ratings yet
- Fast and Reliable: Handheld TympanometerDocument4 pagesFast and Reliable: Handheld TympanometersermedNo ratings yet
- Lab 1 Write UpDocument17 pagesLab 1 Write Upapi-272723910No ratings yet
- Hearing Research: Lingling Cai, Glenna Stomackin, Nicholas M. Perez, Xiaohui Lin, Timothy T. Jung, Wei DongDocument10 pagesHearing Research: Lingling Cai, Glenna Stomackin, Nicholas M. Perez, Xiaohui Lin, Timothy T. Jung, Wei DongJasmy FfNo ratings yet
- Auditory Pattern Perception in 'Split Brain' PatientsDocument3 pagesAuditory Pattern Perception in 'Split Brain' PatientsAnthonyNo ratings yet
- Ultrasonic Diffraction at Different Single and Double Slit SystemsDocument5 pagesUltrasonic Diffraction at Different Single and Double Slit SystemsJose GalvanNo ratings yet
- CP 06 - Determine The Speed of Sound in AirDocument2 pagesCP 06 - Determine The Speed of Sound in AirHsu MonNo ratings yet
- 2931 Montreux 1990 (10 Pages)Document10 pages2931 Montreux 1990 (10 Pages)JulianNo ratings yet
- 10.1097@00129492-200307000-00004Document12 pages10.1097@00129492-200307000-00004hoormohameed2019No ratings yet
- Hearing TestingDocument6 pagesHearing TestingMelody RodriguezNo ratings yet
- Experiment No. 2Document5 pagesExperiment No. 2BE B 39 SURYAPRATAP SINGHNo ratings yet
- TRANS 4 - Audiology 2021 Dr. DalandagDocument9 pagesTRANS 4 - Audiology 2021 Dr. DalandagNestle NgoNo ratings yet
- DHT Sept Wadia 2 PDFDocument3 pagesDHT Sept Wadia 2 PDFsita ameliaNo ratings yet
- DHT Sept Wadia 2 PDFDocument3 pagesDHT Sept Wadia 2 PDFsita ameliaNo ratings yet
- Am J Otolaryngol: Eugene Hung Chih Wong, Aun Wee ChongDocument5 pagesAm J Otolaryngol: Eugene Hung Chih Wong, Aun Wee ChongLee제노No ratings yet
- Sample Experiment Paper 2Document3 pagesSample Experiment Paper 2cnaonwdocnsonkNo ratings yet
- (2003 Bernard) The Anchorage of Brånemark and ITI Implants of Different Lengths. I. An Experimental Study in The Canine MandibleDocument8 pages(2003 Bernard) The Anchorage of Brånemark and ITI Implants of Different Lengths. I. An Experimental Study in The Canine Mandibleyena1010No ratings yet
- 2017-Cai Et Al-An Extended Neck Versus A Spiral Neck of The Helmholtz ResonatorDocument7 pages2017-Cai Et Al-An Extended Neck Versus A Spiral Neck of The Helmholtz ResonatorAndres PalacioNo ratings yet
- Doppler Shift Compensation in South Indian CF-FM BatsDocument8 pagesDoppler Shift Compensation in South Indian CF-FM BatsNikolina NinaNo ratings yet
- CSU07204-Lecture 4.CSU07204-Physical Layer-AnalogDocument46 pagesCSU07204-Lecture 4.CSU07204-Physical Layer-AnalogElikana BarikiNo ratings yet
- Acoustic Reflex Evaluation For Site of Lesion: What Is A Reflex?Document4 pagesAcoustic Reflex Evaluation For Site of Lesion: What Is A Reflex?Estudiantede FonoaudiologíaNo ratings yet
- Hearing Threshold Estimation by Acoustic Reflex Threshold (ART)Document5 pagesHearing Threshold Estimation by Acoustic Reflex Threshold (ART)Estudiantede FonoaudiologíaNo ratings yet
- Acoustic Reflex Evaluation For Site of Lesion: What Is A Reflex?Document4 pagesAcoustic Reflex Evaluation For Site of Lesion: What Is A Reflex?Estudiantede FonoaudiologíaNo ratings yet
- The Efferent Auditory System: Olivocochlear BundleDocument8 pagesThe Efferent Auditory System: Olivocochlear BundleEstudiantede FonoaudiologíaNo ratings yet
- Acoustic Reflex Evaluation For Site of Lesion: What Is A Reflex?Document4 pagesAcoustic Reflex Evaluation For Site of Lesion: What Is A Reflex?Estudiantede FonoaudiologíaNo ratings yet
- Hearing Threshold Estimation by Acoustic Reflex Threshold (ART)Document5 pagesHearing Threshold Estimation by Acoustic Reflex Threshold (ART)Estudiantede FonoaudiologíaNo ratings yet
- Ent Case StudyDocument14 pagesEnt Case StudyAmir Aiman33% (3)
- Difference Between Hearing and Listening 1Document10 pagesDifference Between Hearing and Listening 1walid abdulmonemNo ratings yet
- Noise Control in OC, UG & MPPDocument83 pagesNoise Control in OC, UG & MPPSubhamoy GhoshNo ratings yet
- Building Utilities AcousticsDocument2 pagesBuilding Utilities AcousticsKim SejeongNo ratings yet
- B.ed. Special Education Syllabus NewDocument40 pagesB.ed. Special Education Syllabus Newmalkarpm100% (2)
- Instructions For Use - US: Science Made SmarterDocument55 pagesInstructions For Use - US: Science Made SmarterLili SaquingaNo ratings yet
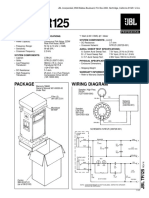
- JBL TR125Document2 pagesJBL TR125Jose Gregorio Ortega CarrilloNo ratings yet
- Cholesteatoma - Diagnosing The Unsafe EarDocument6 pagesCholesteatoma - Diagnosing The Unsafe EarGuillermo StipechNo ratings yet
- Sound Level Meter: Model: SL-4022Document2 pagesSound Level Meter: Model: SL-4022megacobNo ratings yet
- Lesson Plan Science5thDocument9 pagesLesson Plan Science5thapi-284227922No ratings yet
- Ent MCQ 20000Document19 pagesEnt MCQ 20000Dr-Firas Nayf Al-Thawabia82% (33)
- AnsdDocument22 pagesAnsdigorNo ratings yet
- Effective Listening SkillsDocument10 pagesEffective Listening Skillsmba2009-10No ratings yet
- 09 Science Notes ch+12 Sound PDFDocument6 pages09 Science Notes ch+12 Sound PDFafhamNo ratings yet
- Congenital Cholesteatoma TheoriesDocument14 pagesCongenital Cholesteatoma Theoriesapi-19500641No ratings yet
- MH 31a8j Technical Supplement PDFDocument1 pageMH 31a8j Technical Supplement PDFVitaliy OnyshchenkoNo ratings yet
- Profile of Detection and Intervention in Children With Congenital Deafness in Audiology Clinic Dr. Soetomo HospitalDocument1 pageProfile of Detection and Intervention in Children With Congenital Deafness in Audiology Clinic Dr. Soetomo Hospitalelman jokoNo ratings yet
- P A ReferencemanualDocument87 pagesP A ReferencemanualGanesha NayakNo ratings yet
- Sensory Organs: EYE EAR Tongue Skin NoseDocument101 pagesSensory Organs: EYE EAR Tongue Skin NoseSaba PathyNo ratings yet
- Batson2017 OtosclerosisDocument6 pagesBatson2017 OtosclerosisnuhajazminNo ratings yet
- First Periodical Test Science and Health 3Document4 pagesFirst Periodical Test Science and Health 3Bianca Camille Quiazon AguilusNo ratings yet
- Perfect Pitch For YouDocument126 pagesPerfect Pitch For YouDana Wright100% (7)
- Ear DisordersDocument5 pagesEar DisordersClara De Guzman100% (2)
- Nursing student reviews client with presbycusis hearing lossDocument5 pagesNursing student reviews client with presbycusis hearing lossFaisal IzharNo ratings yet
- Anatomy and Physiology of Hearing SystemDocument63 pagesAnatomy and Physiology of Hearing SystemKharenza Vania Azarine Bachtiar100% (1)
- Building Utilities Definition of TermsDocument8 pagesBuilding Utilities Definition of TermsVienci Haya AlbaNo ratings yet
- ch36 PDFDocument2 pagesch36 PDFbest badmintonNo ratings yet
- P-Audio - Preturi Difuzoare - WWW - PoweraudioDocument2 pagesP-Audio - Preturi Difuzoare - WWW - PoweraudioANDREI25111988No ratings yet
- Plowshares #23: Farming With A Hearing ImpairmentDocument10 pagesPlowshares #23: Farming With A Hearing ImpairmentSooraj Kannan, P.V.No ratings yet
- Tone - YZ ChinDocument5 pagesTone - YZ ChinTeacherAmeeNo ratings yet