You might also like
- Medicine: The Effectiveness of Acupuncture For Chronic Pain With DepressionDocument6 pagesMedicine: The Effectiveness of Acupuncture For Chronic Pain With DepressionRatrika SariNo ratings yet
- The Efficacy of Acupuncture For The Treatment of Sciatica - A Systematic Review and Meta-AnalysisDocument13 pagesThe Efficacy of Acupuncture For The Treatment of Sciatica - A Systematic Review and Meta-AnalysisDan CarcamoNo ratings yet
- 2020 Article 2955Document11 pages2020 Article 2955yakiniku10eNo ratings yet
- TTH KronisDocument8 pagesTTH KronisseruniallisaaslimNo ratings yet
- Complementary Therapies in Clinical PracticeDocument18 pagesComplementary Therapies in Clinical PracticeNgaWa ChowNo ratings yet
- Therapeutic Use of Low-Dose Local AnestheticsDocument16 pagesTherapeutic Use of Low-Dose Local AnestheticsXavierLuqueNo ratings yet
- Review Article: Clinical Efficacy of Acupuncture On Rheumatoid Arthritis and Associated Mechanisms: A Systemic ReviewDocument22 pagesReview Article: Clinical Efficacy of Acupuncture On Rheumatoid Arthritis and Associated Mechanisms: A Systemic Reviewdeepa rNo ratings yet
- 1.METAANALISISDocument7 pages1.METAANALISISflorecitaballeutica992No ratings yet
- Review ArticleDocument15 pagesReview ArticleAugustinNo ratings yet
- Clinical Model For Pattern Recognition in Pain AssessmentDocument8 pagesClinical Model For Pattern Recognition in Pain AssessmentSteffani PinheiroNo ratings yet
- A Meta-Analysis of The Effect of Nape Acupuncture Combined With Rehabilitation Training in The Treatment of Dysphagia After StrokeDocument8 pagesA Meta-Analysis of The Effect of Nape Acupuncture Combined With Rehabilitation Training in The Treatment of Dysphagia After Strokep.chenestNo ratings yet
- Review Article: Acupoints For Tension-Type Headache: A Literature Study Based On Data Mining TechnologyDocument10 pagesReview Article: Acupoints For Tension-Type Headache: A Literature Study Based On Data Mining TechnologyHenrique MartinsNo ratings yet
- AComprehensive Algorithm For Management of Neuropathic Pain PDFDocument15 pagesAComprehensive Algorithm For Management of Neuropathic Pain PDFSussan AguedoNo ratings yet
- PDF AlgologiaDocument11 pagesPDF AlgologiaThamires BritoNo ratings yet
- Acupuncture - A National Heritage of China To TheDocument9 pagesAcupuncture - A National Heritage of China To TheOSMAR FAVIO FERNANDEZ SOLARNo ratings yet
- Fpain 02 765921Document14 pagesFpain 02 765921xbeligNo ratings yet
- Complementary Therapies in Clinical PracticeDocument7 pagesComplementary Therapies in Clinical PracticeBkash ShahNo ratings yet
- Review Article: Efficacy of Acupuncture in Reducing Preoperative Anxiety: A Meta-AnalysisDocument13 pagesReview Article: Efficacy of Acupuncture in Reducing Preoperative Anxiety: A Meta-AnalysisDyan TonyNo ratings yet
- Ughreja Myofascial ReleaseDocument9 pagesUghreja Myofascial Releasecris.endo.ceNo ratings yet
- Conservative Management of Mechanical NeDocument20 pagesConservative Management of Mechanical NeVladislav KotovNo ratings yet
- 2017 PNF and Manual Therapy Treatment Results of Cervical OADocument7 pages2017 PNF and Manual Therapy Treatment Results of Cervical OApainfree888100% (1)
- Adult Sedation and Analgesia in A Resource Limited Intensive Care Unit - ADocument11 pagesAdult Sedation and Analgesia in A Resource Limited Intensive Care Unit - APutra SetiawanNo ratings yet
- Review Article Acupuncture For Spasticity After Stroke: A Systematic Review and Meta-Analysis of Randomized Controlled TrialsDocument26 pagesReview Article Acupuncture For Spasticity After Stroke: A Systematic Review and Meta-Analysis of Randomized Controlled TrialsYUTRILIANo ratings yet
- Role of Craniosacral Therapy For Chronic PainDocument32 pagesRole of Craniosacral Therapy For Chronic PainTrusha Vora100% (1)
- McKenzie Mechanical Syndromes Coincide With Biopsychosocial InfluencesDocument14 pagesMcKenzie Mechanical Syndromes Coincide With Biopsychosocial InfluencesTomáš KrajíčekNo ratings yet
- Apm 22145Document12 pagesApm 22145dramaholic842No ratings yet
- (Jiancheng 2021) Medical Devices For Tremur Suppression, Current Status and Future DirectionsDocument22 pages(Jiancheng 2021) Medical Devices For Tremur Suppression, Current Status and Future DirectionsCarlos Gianpaul Rincón RuizNo ratings yet
- Review Article Extracorporeal Shock Wave Therapy For The Treatment of Osteoarthritis: A Systematic Review and Meta-AnalysisDocument15 pagesReview Article Extracorporeal Shock Wave Therapy For The Treatment of Osteoarthritis: A Systematic Review and Meta-Analysissymbiosis.ikfrNo ratings yet
- Manual Therapy Versus Therapeutic Exercise in Non-Specific Chronic Neck Pain: A Randomized Controlled TrialDocument10 pagesManual Therapy Versus Therapeutic Exercise in Non-Specific Chronic Neck Pain: A Randomized Controlled TrialMichele MarengoNo ratings yet
- Medicine: The Effectiveness and Safety of Electroacupuncture For Nonspecific Chronic Low Back PainDocument4 pagesMedicine: The Effectiveness and Safety of Electroacupuncture For Nonspecific Chronic Low Back PainMohammad Rafi NampiraNo ratings yet
- Acupuncture For Primary Fibromyalgia: Study Protocol of A Randomized Controlled TrialDocument9 pagesAcupuncture For Primary Fibromyalgia: Study Protocol of A Randomized Controlled TrialSILVIA ROSARIO CHALCO MENDOZANo ratings yet
- Recommendations For Physiotherapy Intervention After Stroke 5712Document9 pagesRecommendations For Physiotherapy Intervention After Stroke 5712Anonymous Ezsgg0VSENo ratings yet
- JCM 10 00086 v2Document19 pagesJCM 10 00086 v2Dana DumitruNo ratings yet
- Efficacy and Safety of Electroacupuncture For Post Stroke Depression: Study Protocol For A Randomized Controlled TrialDocument8 pagesEfficacy and Safety of Electroacupuncture For Post Stroke Depression: Study Protocol For A Randomized Controlled TrialwindapuspitasalimNo ratings yet
- Acupuncture Is My WorkDocument13 pagesAcupuncture Is My WorkDe BaronNo ratings yet
- Ecam2015 870398Document12 pagesEcam2015 870398YUTRILIANo ratings yet
- Eye Acupuncture For Pain Conditions: A Scoping Review of Clinical StudiesDocument10 pagesEye Acupuncture For Pain Conditions: A Scoping Review of Clinical StudiesIngdrawati TjiangNo ratings yet
- Manejo Dolor RTMSDocument32 pagesManejo Dolor RTMSenviosmentalmedNo ratings yet
- Zhangxinof Acupuncture For Stroke Rehabilitation Recommendations Based On High-Quality EvidenceDocument12 pagesZhangxinof Acupuncture For Stroke Rehabilitation Recommendations Based On High-Quality EvidenceAnna AzizahNo ratings yet
- Body Acupuncture For Nicotine Withdrawal Symptoms: A Randomized Placebo-Controlled TrialDocument6 pagesBody Acupuncture For Nicotine Withdrawal Symptoms: A Randomized Placebo-Controlled TrialGraziele GuimaraesNo ratings yet
- Does Auriculotherapy Have Therapeutic E EctivenessDocument10 pagesDoes Auriculotherapy Have Therapeutic E EctivenessprdpjbNo ratings yet
- Effectiveness of Shock Wave Therapy As A Treatment For Spasticity A Systematic ReviewDocument18 pagesEffectiveness of Shock Wave Therapy As A Treatment For Spasticity A Systematic ReviewMandy BoylettNo ratings yet
- Meta-analysis- Hypnosis for painDocument17 pagesMeta-analysis- Hypnosis for painmalwinatmdNo ratings yet
- TENS Literature - Review - and - Meta - Analysis - Of.99266Document9 pagesTENS Literature - Review - and - Meta - Analysis - Of.99266Adam ForshawNo ratings yet
- Critical AppraisalDocument12 pagesCritical Appraisalderrick owinoNo ratings yet
- 1 - 2017 - Tuina para Prob Musculo-Esqueléticos - Rev SistDocument22 pages1 - 2017 - Tuina para Prob Musculo-Esqueléticos - Rev SistLuis Miguel MartinsNo ratings yet
- Auriculotherapy For Pain Management: A Systematic Review and Meta-Analysis of Randomized Controlled TrialsDocument12 pagesAuriculotherapy For Pain Management: A Systematic Review and Meta-Analysis of Randomized Controlled TrialsSol Instituto TerapêuticoNo ratings yet
- Acupuncture Treatment On The Motor Area of The Sca PDFDocument12 pagesAcupuncture Treatment On The Motor Area of The Sca PDFSANGGA BUWANANo ratings yet
- Medicine: Treatment of Lateral Epicondylitis With Acupuncture and GlucocorticoidDocument3 pagesMedicine: Treatment of Lateral Epicondylitis With Acupuncture and Glucocorticoidindra coolNo ratings yet
- 2022 Article 456Document21 pages2022 Article 456Zu TranNo ratings yet
- Oamjms 11f 180Document16 pagesOamjms 11f 180clinichafshahNo ratings yet
- Acupuncture For Balance Dysfunction in Patients With StrokeDocument5 pagesAcupuncture For Balance Dysfunction in Patients With StrokeTinnitus Man IndonesiaNo ratings yet
- Auricular Acupuncture For Pain PDFDocument14 pagesAuricular Acupuncture For Pain PDFDerek Doran100% (1)
- Kiiko Matsumotos Clinical StrategiesDocument1 pageKiiko Matsumotos Clinical Strategiestiera0% (1)
- Contemporary Clinical Trials CommunicationsDocument11 pagesContemporary Clinical Trials CommunicationsElizabeth Mautino CaceresNo ratings yet
- Medi 102 E33939Document10 pagesMedi 102 E33939Ivan HartantoNo ratings yet
- DikonversiDocument17 pagesDikonversiAkbar FitryansyahNo ratings yet
- Torticolis OdtDocument25 pagesTorticolis OdtAndreea CimpoiNo ratings yet
- University of Cambridge Local Examinations Syndicate Biomedical Admissions TestDocument20 pagesUniversity of Cambridge Local Examinations Syndicate Biomedical Admissions TestNeil SahooNo ratings yet
- Miracles of Mind BodyDocument5 pagesMiracles of Mind BodyAdam DeeveenoNo ratings yet
- Cervicogenic Headache Diagnosis and Symptoms Compared to Migraine and Tension HeadachesDocument10 pagesCervicogenic Headache Diagnosis and Symptoms Compared to Migraine and Tension Headachespuchio100% (1)
- Frontal Impact EURO NCAP PDFDocument52 pagesFrontal Impact EURO NCAP PDFMihalcea Ghe Ovidiu100% (1)
- Carhs 2019 Safety Companion PDFDocument180 pagesCarhs 2019 Safety Companion PDFvish_537756528100% (1)
- TMJDocument11 pagesTMJsetiaganshaNo ratings yet
- Medical ReportDocument5 pagesMedical ReportRuthdel KazumiNo ratings yet
- Putnam PressDocument24 pagesPutnam PressAndrew GoldstonNo ratings yet
- Understanding Rearend CollisionsDocument21 pagesUnderstanding Rearend CollisionsMark Hefter100% (1)
- Working With Whiplash, Part I (Myofascial Techniques)Document5 pagesWorking With Whiplash, Part I (Myofascial Techniques)Advanced-Trainings.com100% (4)
- Spinal Cord Injury: Presented By: Feliciano, Jenard R. Flores, Arliah Q. Gaspar, Danica VDocument79 pagesSpinal Cord Injury: Presented By: Feliciano, Jenard R. Flores, Arliah Q. Gaspar, Danica VPam RomeroNo ratings yet
- NUR 115 - LAB ACTIVITY # 1bDocument3 pagesNUR 115 - LAB ACTIVITY # 1bMoira Julianne Serognas BrigoliNo ratings yet
- Whiplash Injury Recovery: A Self-Help GuideDocument44 pagesWhiplash Injury Recovery: A Self-Help GuideIfigeneia AslanidouNo ratings yet
- Office OrthopaedicsDocument308 pagesOffice OrthopaedicsJohn Reynolds100% (10)
- Rule: Motor Vehicle Safety Standards: Head Restraints For Passenger Cars and Light Multipurpose Vehicles, Trucks, and BusesDocument42 pagesRule: Motor Vehicle Safety Standards: Head Restraints For Passenger Cars and Light Multipurpose Vehicles, Trucks, and BusesJustia.comNo ratings yet
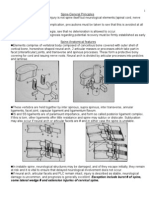
- Exception Include Burst # of Spine, Some Lateral Wedge # and Extension Injuries of Cervical SpineDocument29 pagesException Include Burst # of Spine, Some Lateral Wedge # and Extension Injuries of Cervical Spinebhavesh jain100% (2)
- Orthopaedic Physical AssessmentDocument2 pagesOrthopaedic Physical AssessmentvaishnaviNo ratings yet
- Medical Legal Report ExampleDocument8 pagesMedical Legal Report ExampleYujilin Yamashita MotoNo ratings yet
- Effectiveness of Small Daily Amounts of Progressive Resistance Training For Frequent Neck/shoulder Pain: Randomised Controlled TrialDocument7 pagesEffectiveness of Small Daily Amounts of Progressive Resistance Training For Frequent Neck/shoulder Pain: Randomised Controlled TrialkineluzaNo ratings yet
- SS - GEN-12-Final Road Safety Standard Rev 03Document22 pagesSS - GEN-12-Final Road Safety Standard Rev 03madhulikaNo ratings yet
- Whiplash Practice Guidelines 2003Document30 pagesWhiplash Practice Guidelines 2003silkofosNo ratings yet
- Chronic WhiplashDocument7 pagesChronic WhiplashsoylahijadeunvampiroNo ratings yet
- 045 Dy Teban Trading V ChingDocument6 pages045 Dy Teban Trading V ChingArnel MangilimanNo ratings yet
- Validity of The Neck Disability Index and Neck Pain and Disability Scale For Measuring Disability Associated With Chronic, Non-Traumatic Neck PainDocument12 pagesValidity of The Neck Disability Index and Neck Pain and Disability Scale For Measuring Disability Associated With Chronic, Non-Traumatic Neck PainDESY NATALIANA PUTRINo ratings yet
- S80Document70 pagesS80api-3718946100% (2)
- 2000 NASS Injury Coding Manual (From Docket)Document202 pages2000 NASS Injury Coding Manual (From Docket)Barbara Moroski-BrowneNo ratings yet
- Euro Ncap Whiplash Test Protocol v3 1Document70 pagesEuro Ncap Whiplash Test Protocol v3 1Marius TancaNo ratings yet
- Cervicogenic Headache PDFDocument13 pagesCervicogenic Headache PDFSuganya Balachandran100% (2)
- Cymat AluminiumDocument10 pagesCymat AluminiumnguyenvannganpcNo ratings yet