You might also like
- Post-Viral Effects of COVID-19 in The Olfactory System and Their ImplicationsDocument9 pagesPost-Viral Effects of COVID-19 in The Olfactory System and Their ImplicationsJorge Augusto Israel 狼No ratings yet
- ANALYSIS AND DESIGN OF Cable Stayed BridgeDocument31 pagesANALYSIS AND DESIGN OF Cable Stayed Bridgeshrikantharle100% (1)
- Pricing 02Document37 pagesPricing 02Rahul AnandNo ratings yet
- Project Management Plan - Security Management PlanDocument10 pagesProject Management Plan - Security Management Planario widjaksonoNo ratings yet
- Small Air Forces Observer: Vol. 24 No. 4Document33 pagesSmall Air Forces Observer: Vol. 24 No. 4Panos ThalassisNo ratings yet
- Idiopathic Pulmonary Fibrosis: Diagnosis, Epidemiology and Natural HistoryDocument11 pagesIdiopathic Pulmonary Fibrosis: Diagnosis, Epidemiology and Natural HistorySuwandi AlghozyNo ratings yet
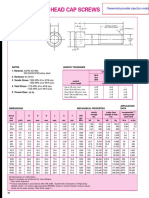
- Metric Socket Head Cap ScrewsDocument2 pagesMetric Socket Head Cap ScrewsImam MulyonoNo ratings yet
- Wiring Fiesta - AP - WD12Document472 pagesWiring Fiesta - AP - WD12Sanun Automatictranmission100% (4)
- COVID-19 LEGACY: SARS-CoV-2 clinical trials, vaccines trials and bioethicsFrom EverandCOVID-19 LEGACY: SARS-CoV-2 clinical trials, vaccines trials and bioethicsNo ratings yet
- Administrative Support UNITSDocument74 pagesAdministrative Support UNITSReina Allyza Pineda100% (1)
- Potential Pathogenesis of Ageusia and Anosmia in COVID-19 PatientsDocument2 pagesPotential Pathogenesis of Ageusia and Anosmia in COVID-19 PatientsCoryza Gabrie tanNo ratings yet
- 17-Neurological Infections in 2020 COVID-1takes Centre StageDocument2 pages17-Neurological Infections in 2020 COVID-1takes Centre StageVerónica GaticaNo ratings yet
- Correspondence: Smell and Taste Dysfunction in Patients With COVID-19Document1 pageCorrespondence: Smell and Taste Dysfunction in Patients With COVID-19Dhyo Asy-shidiq HasNo ratings yet
- Jnma, Apar PokharelDocument6 pagesJnma, Apar PokharelNicca RodilNo ratings yet
- RMV 2107Document6 pagesRMV 2107Ahmed AllamNo ratings yet
- Jurnal AnosmiaDocument5 pagesJurnal Anosmiadhea handyaraNo ratings yet
- Anosmia and Ageusia Associated With Coronavirus Infection (COVID 19) What Is Known?Document4 pagesAnosmia and Ageusia Associated With Coronavirus Infection (COVID 19) What Is Known?Angelita Torres LlacsahuangaNo ratings yet
- Oral Manifestations in Hospitalized COVID PatientsDocument7 pagesOral Manifestations in Hospitalized COVID PatientsEdoardo BiancoNo ratings yet
- Z. Citasi Piis014067362030917xDocument3 pagesZ. Citasi Piis014067362030917xMastifa HanasitaNo ratings yet
- Articulo Fisiopatologia de La Enfermedad 2Document5 pagesArticulo Fisiopatologia de La Enfermedad 2ivanNo ratings yet
- Narrative Reviews: Diarrhea During COVID-19 Infection: Pathogenesis, Epidemiology, Prevention, and ManagementDocument10 pagesNarrative Reviews: Diarrhea During COVID-19 Infection: Pathogenesis, Epidemiology, Prevention, and ManagementWaqasKhanNo ratings yet
- 2781 2783Document3 pages2781 2783Manuel Angel G BNo ratings yet
- Nihms 1664293Document21 pagesNihms 1664293MARIA MONTSERRAT SOMOZA MONCADANo ratings yet
- Amjphnation00492 0044Document6 pagesAmjphnation00492 0044hakmoch hakmNo ratings yet
- Gustatory Dysfunction As An Early Symptom in COVID-19 ScreeningDocument3 pagesGustatory Dysfunction As An Early Symptom in COVID-19 ScreeningAndhika DipaNo ratings yet
- Diarrhea During COVID-19 InfectionDocument11 pagesDiarrhea During COVID-19 InfectionMan'SzAr'diAnSyAhNo ratings yet
- Excellent Paper On Covid 19Document20 pagesExcellent Paper On Covid 19GalenNo ratings yet
- Jurnal 16Document9 pagesJurnal 16Putri Intan SolehahNo ratings yet
- 8 - COVID-19-related Anosmia Is Associated With Viral Persistence and Inflammation in Human Olfactory Epithelium and Brain Infection in HamstersDocument18 pages8 - COVID-19-related Anosmia Is Associated With Viral Persistence and Inflammation in Human Olfactory Epithelium and Brain Infection in HamstersVerónica GaticaNo ratings yet
- 6 Speth OlfactoryDocument7 pages6 Speth OlfactoryLimeysahni NazhoeNo ratings yet
- Epid Pubmed 1 (Bab2) .En - IdDocument11 pagesEpid Pubmed 1 (Bab2) .En - IdSHAFIYA ADELINANo ratings yet
- BiomedPap - Bio 202003 0001Document9 pagesBiomedPap - Bio 202003 0001Edison Chiriboga OrtegaNo ratings yet
- The Immune Response To Sars-Cov-2 and Covid-19 Immunopathology - Current PerspectivesDocument15 pagesThe Immune Response To Sars-Cov-2 and Covid-19 Immunopathology - Current PerspectivesLydie Praxede EkoboNo ratings yet
- Comment: Lancet Infect Dis 2020Document2 pagesComment: Lancet Infect Dis 2020kayegi8666No ratings yet
- Upper Airways SymsDocument8 pagesUpper Airways SymsSekarrini VidyatamiNo ratings yet
- PIIS0168827820336758Document17 pagesPIIS0168827820336758Yusup AhmadiNo ratings yet
- Knowing When and How To Fight: COVID-19 Between Viral Clearance and Immune ToleranceDocument11 pagesKnowing When and How To Fight: COVID-19 Between Viral Clearance and Immune ToleranceAri Trianto WibowoNo ratings yet
- Pas 46 528Document9 pagesPas 46 528maya dwiNo ratings yet
- Difficulties in Diagnosis of Psittacosis or Ornithosis: A Case ReportDocument4 pagesDifficulties in Diagnosis of Psittacosis or Ornithosis: A Case ReportYusrinabillaNo ratings yet
- Pi Is 0749070421000439Document21 pagesPi Is 0749070421000439Vlady78No ratings yet
- Historia de Nuevo CoronavirusDocument6 pagesHistoria de Nuevo CoronavirusGiiszs AlvarezNo ratings yet
- JMV 25815Document2 pagesJMV 25815fadil ahmadiNo ratings yet
- Lesiones Orales Covid19Document7 pagesLesiones Orales Covid19Diana PerezNo ratings yet
- Chary Et Al 2020 Prevalence and Recovery From Olfactory and Gustatory Dysfunctions in Covid 19 Infection A ProspectiveDocument8 pagesChary Et Al 2020 Prevalence and Recovery From Olfactory and Gustatory Dysfunctions in Covid 19 Infection A Prospectiveika nurul shofiyahNo ratings yet
- Innate and Adaptive Immune Responses Against CoronavirusDocument17 pagesInnate and Adaptive Immune Responses Against CoronavirusHARDITA SALSABILA FORTUNA HARDITA SALSABILA FORTUNANo ratings yet
- Tammaro2020 Covid 19Document7 pagesTammaro2020 Covid 19eva yustianaNo ratings yet
- Conjunctivitis and COVID 19: A Meta Analysis: LettertotheeditorDocument2 pagesConjunctivitis and COVID 19: A Meta Analysis: LettertotheeditorAngel LimNo ratings yet
- Medical Hypotheses: Sapideh Gilani, Rachel Roditi, Mohsen Naraghi TDocument3 pagesMedical Hypotheses: Sapideh Gilani, Rachel Roditi, Mohsen Naraghi TDhyo Asy-shidiq HasNo ratings yet
- Anosmia and COVID-19: Perspectives On Its Association and The Pathophysiological Mechanisms InvolvedDocument8 pagesAnosmia and COVID-19: Perspectives On Its Association and The Pathophysiological Mechanisms Involveddhea handyaraNo ratings yet
- COVID-19 and The Gastrointestinal Tract: More Than Meets The EyeDocument2 pagesCOVID-19 and The Gastrointestinal Tract: More Than Meets The EyeRendra SyaniNo ratings yet
- Potential Pathogenesis of Ageusia and Anosmia in COVID-19 PatientsDocument3 pagesPotential Pathogenesis of Ageusia and Anosmia in COVID-19 PatientsJonathan FergusonNo ratings yet
- PIIS0954611120303796Document7 pagesPIIS0954611120303796Cinthia Lisset Natividad PeñaNo ratings yet
- 1 s2.0 S0002944010613296 MainDocument12 pages1 s2.0 S0002944010613296 MainShop from KostNo ratings yet
- The Modelling of COVID19 Pathways Sheds Light On Mechanisms, Opportunities and On Controversial Interpretations of Medical Treatments. v2Document15 pagesThe Modelling of COVID19 Pathways Sheds Light On Mechanisms, Opportunities and On Controversial Interpretations of Medical Treatments. v2ballechaseNo ratings yet
- Histopathological Findings in Fatal COVID-19 Severe Acute Respiratory Syndrome: Preliminary Experience From A Series of 10 Spanish PatientsDocument3 pagesHistopathological Findings in Fatal COVID-19 Severe Acute Respiratory Syndrome: Preliminary Experience From A Series of 10 Spanish PatientsSaray florezNo ratings yet
- Journal of Infection: Letter To The EditorDocument2 pagesJournal of Infection: Letter To The EditorLee제노No ratings yet
- Apparent Crazy Paving "Pulmonary Alveolar Proteinosis Versus Hypersensitivity Pneumonitis"Document4 pagesApparent Crazy Paving "Pulmonary Alveolar Proteinosis Versus Hypersensitivity Pneumonitis"BRNSS Publication Hub InfoNo ratings yet
- Correspondence: Utility of Hyposmia and Hypogeusia For The Diagnosis of COVID-19Document2 pagesCorrespondence: Utility of Hyposmia and Hypogeusia For The Diagnosis of COVID-19Dhyo Asy-shidiq HasNo ratings yet
- New ChallengeDocument3 pagesNew ChallengeEliana TorresNo ratings yet
- COVID-19 and Multi-Organ ResponseDocument31 pagesCOVID-19 and Multi-Organ ResponseArbaz SultanNo ratings yet
- Carvalho Et Al. - 2023 - Presumed Endogenous Fungal Endophthalmitis in A PaDocument2 pagesCarvalho Et Al. - 2023 - Presumed Endogenous Fungal Endophthalmitis in A PaZohra TouatiNo ratings yet
- Gutjnl 2020 321195.full PDFDocument2 pagesGutjnl 2020 321195.full PDFnjwa pdjaNo ratings yet
- A Nicotinic Approach To CovidDocument11 pagesA Nicotinic Approach To Covidraphael.hunzingerNo ratings yet
- Shetty2022 Article InvasiveAspergillosisOfNoseAndDocument6 pagesShetty2022 Article InvasiveAspergillosisOfNoseAndAndreea CiorneaNo ratings yet
- 12 - Evidence of Central Nervous System Infection and Neuroinvasive Routes As WellDocument11 pages12 - Evidence of Central Nervous System Infection and Neuroinvasive Routes As WellVerónica GaticaNo ratings yet
- Anosmia and Ageusia: Common Findings in COVID-19 PatientsDocument1 pageAnosmia and Ageusia: Common Findings in COVID-19 PatientsMahtosurup GodavarthyNo ratings yet
- COVID-19 and Anosmia:: A Review Based On Up-To-Date KnowledgeDocument22 pagesCOVID-19 and Anosmia:: A Review Based On Up-To-Date KnowledgeNovia RNo ratings yet
- Identifikasi Struktur Anatomi Tulang Tengkorak Normal Pada Radiografi Anteroposterior, Lateral, Towne, Dan Vertex SubmentalDocument27 pagesIdentifikasi Struktur Anatomi Tulang Tengkorak Normal Pada Radiografi Anteroposterior, Lateral, Towne, Dan Vertex SubmentalArief PurwoditoNo ratings yet
- Chiu2021 Article COVID 19 InducedAnosmiaAssociaDocument2 pagesChiu2021 Article COVID 19 InducedAnosmiaAssociaArief PurwoditoNo ratings yet
- The New England Journal of MedicineDocument7 pagesThe New England Journal of MedicineArief PurwoditoNo ratings yet
- Safety in The Operating Room: Neurosurgical Perspective: Dattatraya MuzumdarDocument3 pagesSafety in The Operating Room: Neurosurgical Perspective: Dattatraya MuzumdarArief PurwoditoNo ratings yet
- Mastoidectomy and Trans-Corneal Viral TransmissionDocument4 pagesMastoidectomy and Trans-Corneal Viral TransmissionArief PurwoditoNo ratings yet
- Chico Resume 2015 For WebsiteDocument2 pagesChico Resume 2015 For Websiteapi-87866586No ratings yet
- Blue ScreenDocument9 pagesBlue ScreenRafik DjoucampNo ratings yet
- Chapter 1: Introduction To ITIL: Preparatory ExerciseDocument3 pagesChapter 1: Introduction To ITIL: Preparatory ExerciseMohamed AlyNo ratings yet
- 16 PFDocument19 pages16 PFNoureen SattarNo ratings yet
- Snap Inc.-WPS OfficeDocument13 pagesSnap Inc.-WPS OfficeAlvieNo ratings yet
- Lemonade Stall Version 1 - 4Document19 pagesLemonade Stall Version 1 - 4Alan LibertNo ratings yet
- L Series L55 75Document8 pagesL Series L55 75sugengrahayune71No ratings yet
- ResetrefocusrevitalizeDocument40 pagesResetrefocusrevitalizeapi-250396415No ratings yet
- Reading Sketch Up 1 - 이램프 - Page 1 - 106 - Flip PDF Online - PubHTML5Document106 pagesReading Sketch Up 1 - 이램프 - Page 1 - 106 - Flip PDF Online - PubHTML5Maricel MaglahusNo ratings yet
- Understanding ASEAN: Its Systems & StructuresDocument59 pagesUnderstanding ASEAN: Its Systems & StructureskaiaceegeesNo ratings yet
- EMC Part 1a PDFDocument3 pagesEMC Part 1a PDFAlexander OngNo ratings yet
- Anonymous Complaint Says Officer Selling GunsDocument5 pagesAnonymous Complaint Says Officer Selling GunsLas Vegas Review-JournalNo ratings yet
- Product Costing Analyst JD v0.2Document2 pagesProduct Costing Analyst JD v0.2Madhav RajbanshiNo ratings yet
- Group 3 - Ib1604 - Ibc201Document37 pagesGroup 3 - Ib1604 - Ibc201Bao Thanh Truc (FUG CT)No ratings yet
- Tax Invoice Confirm Ticket Online Solutions Private Limited No.410 NR Complex 22nd Cross, 24th Main HSR 2nd Sector Bengaluru, Karnataka-560102Document1 pageTax Invoice Confirm Ticket Online Solutions Private Limited No.410 NR Complex 22nd Cross, 24th Main HSR 2nd Sector Bengaluru, Karnataka-560102Soundarya RajlakshmiNo ratings yet
- Not A Formal Quote: Oracle Investment Proposal (As of 3/22/2021)Document1 pageNot A Formal Quote: Oracle Investment Proposal (As of 3/22/2021)Arsenij KroptyaNo ratings yet
- Decorative Metals (r1)Document23 pagesDecorative Metals (r1)irshad khanNo ratings yet
- Qantas AirwaysDocument3 pagesQantas AirwaysCNo ratings yet
- Barangay Disaster Risk Reduction and Management Investment Plan C.Y. 2018-2022Document1 pageBarangay Disaster Risk Reduction and Management Investment Plan C.Y. 2018-2022Cristina MelloriaNo ratings yet
- Wa0015.Document9 pagesWa0015.Santosh Kumar GuptaNo ratings yet
- WWW - Ajoysingha.info: ISTQB Question Paper - 1Document9 pagesWWW - Ajoysingha.info: ISTQB Question Paper - 1Ramesh AkulaNo ratings yet
- Power DesignerDocument112 pagesPower DesignerLuis Eduardo RivasNo ratings yet
- VTU Exam Question Paper With Solution of 18CS63 Web Technology and Its Applications Aug-2022-Dr. Sudhakar K N & Dr. Ganesh D RDocument36 pagesVTU Exam Question Paper With Solution of 18CS63 Web Technology and Its Applications Aug-2022-Dr. Sudhakar K N & Dr. Ganesh D RSatwik NmNo ratings yet