You might also like
- Resuscitation of Patients With Septic Shock PleaseDocument4 pagesResuscitation of Patients With Septic Shock Pleaseabdoel14No ratings yet
- Paper 5Document8 pagesPaper 5Ahmed HamdyNo ratings yet
- Venous-To-Arterial pCO Difference in High-Risk Surgical PatientsDocument7 pagesVenous-To-Arterial pCO Difference in High-Risk Surgical PatientsRuby Valladolid GarcíaNo ratings yet
- The Relationship Between Oxygen Delivery and ConsumptionDocument7 pagesThe Relationship Between Oxygen Delivery and Consumptionjcarl_20063003No ratings yet
- Hartog 2014Document26 pagesHartog 2014mkishore0001No ratings yet
- Relacion Entre SvO y LactatoDocument9 pagesRelacion Entre SvO y LactatoMacros FitNo ratings yet
- Intraoperative Fluid TherapyDocument11 pagesIntraoperative Fluid TherapyArdi FkuiNo ratings yet
- Captura de Ecrã 2024-02-07 À(s) 19.30.27Document19 pagesCaptura de Ecrã 2024-02-07 À(s) 19.30.27yurgan7No ratings yet
- 1 s2.0 S088394411500547X Main PDFDocument6 pages1 s2.0 S088394411500547X Main PDFRomán Jiménez LópezNo ratings yet
- Central Venous-To-Arterial Carbon Dioxide Difference: An Additional Target For Goal-Directed Therapy in Septic Shock?Document8 pagesCentral Venous-To-Arterial Carbon Dioxide Difference: An Additional Target For Goal-Directed Therapy in Septic Shock?rodolfo riosNo ratings yet
- Br. J. Anaesth. 2012 Doherty Bja - Aes171Document11 pagesBr. J. Anaesth. 2012 Doherty Bja - Aes171Ahmad SaifulNo ratings yet
- Continuous - Mixed - Venous - and - Central - Venous - Oxygen Saturation in Cardiac Surgery With Cardiopulmonary BypassDocument5 pagesContinuous - Mixed - Venous - and - Central - Venous - Oxygen Saturation in Cardiac Surgery With Cardiopulmonary Bypassthomas.szapiroNo ratings yet
- Gap Co2 Cocc 2018Document9 pagesGap Co2 Cocc 2018Cesar Rivas CamposNo ratings yet
- 10 1378@chest 09-2690Document9 pages10 1378@chest 09-2690Alvaro Andres Flores JimenezNo ratings yet
- Scvo2 DM Additionalthesis-1Document7 pagesScvo2 DM Additionalthesis-1RonakhNo ratings yet
- UCI Shock Valoracion BuenoDocument7 pagesUCI Shock Valoracion BuenoJuan Camilo Cruz VegaNo ratings yet
- Rheology For CliniciansDocument8 pagesRheology For CliniciansRaluca LNo ratings yet
- The Physiology of VentilationDocument14 pagesThe Physiology of VentilationEva SánchezNo ratings yet
- Using Venous Blood Gas Analysis in The Assessment of COPD Exacerbations A Prospective Cohort StudyDocument7 pagesUsing Venous Blood Gas Analysis in The Assessment of COPD Exacerbations A Prospective Cohort Studynur amaliah idrusNo ratings yet
- De SomerDocument11 pagesDe Somershivalingam20No ratings yet
- Insuf Respiratória Aguda - RevisãoDocument19 pagesInsuf Respiratória Aguda - RevisãoksdposaNo ratings yet
- Capnography: July 2015Document25 pagesCapnography: July 2015Juan Manuel Medina RodriguezNo ratings yet
- Pathophysiology of Oxygen Delivery in Respiratory Failure : Mitchell M. Levy, MD, FCCPDocument7 pagesPathophysiology of Oxygen Delivery in Respiratory Failure : Mitchell M. Levy, MD, FCCPtammy_tataNo ratings yet
- Adequacy of Perfusion During Cardiopulmonary BypassDocument64 pagesAdequacy of Perfusion During Cardiopulmonary BypassBranka Kurtovic50% (2)
- Venous OximetryDocument3 pagesVenous OximetryAndrew MihaiNo ratings yet
- 203 1667 Applications20of20capnographyDocument25 pages203 1667 Applications20of20capnographyLusy Octavia SaputriNo ratings yet
- Saturacion Venosa InglesDocument7 pagesSaturacion Venosa InglesYojhaida Zarate CasachahuaNo ratings yet
- Residents' Resource - ShockDocument21 pagesResidents' Resource - ShockWestleyNo ratings yet
- Evaluation of Respiratory Exchange Ratio (RER) For Predicting Postoperative Outcomes in Elderly PatientsDocument30 pagesEvaluation of Respiratory Exchange Ratio (RER) For Predicting Postoperative Outcomes in Elderly PatientsEshwarNo ratings yet
- HipocalemiaDocument22 pagesHipocalemiaitalofabregaNo ratings yet
- Blood Transfusion in Anaesthesia and Critical Care: Less Is More!Document4 pagesBlood Transfusion in Anaesthesia and Critical Care: Less Is More!Maya_AnggrainiKNo ratings yet
- Ajrccm LactatemiaDocument8 pagesAjrccm LactatemiaGuamata GuamataNo ratings yet
- Oxygen DeliveryDocument11 pagesOxygen DeliveryFatimah Syed OmarNo ratings yet
- Young2022 Article OxygenTargetsDocument4 pagesYoung2022 Article OxygenTargetsBrenda Serrano LaraNo ratings yet
- Intraoperative Fluids: How Much Is Too Much?: Editor's Key PointsDocument11 pagesIntraoperative Fluids: How Much Is Too Much?: Editor's Key PointsRicardoNo ratings yet
- Pathophysiology of Oxygen Delivery in Respiratory Failure : Mitchell M. Levy, MD, FCCPDocument7 pagesPathophysiology of Oxygen Delivery in Respiratory Failure : Mitchell M. Levy, MD, FCCPagiosfilaretosNo ratings yet
- Bakker-2016-Intensive Care MedicineDocument3 pagesBakker-2016-Intensive Care MedicineBiancaPancuNo ratings yet
- Phlebology 2012 Gloviczki 2 9Document9 pagesPhlebology 2012 Gloviczki 2 9Peet UpNo ratings yet
- Journal of Intensive Medicine: Jean-Louis TeboulDocument7 pagesJournal of Intensive Medicine: Jean-Louis TeboulSoilimar QuiñonesNo ratings yet
- 31106572: Deconstructing Hyperlactatemia in Sepsis Using ScvO 2 and Base Deficit PDFDocument9 pages31106572: Deconstructing Hyperlactatemia in Sepsis Using ScvO 2 and Base Deficit PDFLuis Enrique Caceres AlavrezNo ratings yet
- Coagulation Dysfunction in Patients With AECOPD and ItsDocument6 pagesCoagulation Dysfunction in Patients With AECOPD and ItsAndreea MoalesNo ratings yet
- Red Cell Distribution in Critically Ill Patients With Chronic Obstructive Pulmonary DiseaseDocument9 pagesRed Cell Distribution in Critically Ill Patients With Chronic Obstructive Pulmonary Diseaserbatjun576No ratings yet
- Central Venous Pressure and Acute Kidney Injury in Critically Ill Patients With Multiple Comorbidities A Large Retrospective Cohort StudyDocument10 pagesCentral Venous Pressure and Acute Kidney Injury in Critically Ill Patients With Multiple Comorbidities A Large Retrospective Cohort Studyady suciptoNo ratings yet
- Management of Sepsis and Septic ShockDocument29 pagesManagement of Sepsis and Septic ShockWildan Ibnu AdrianNo ratings yet
- Diagnosis of Fluid Overload: From Conventional To Contemporary ConceptsDocument14 pagesDiagnosis of Fluid Overload: From Conventional To Contemporary Conceptsbenitez1228No ratings yet
- Hemodynamic Parameters To Guide Fluid Therapy: Review Open AccessDocument9 pagesHemodynamic Parameters To Guide Fluid Therapy: Review Open AccessClaudioValdiviaNo ratings yet
- Molecular Hydrogen As An Adjuvant Therapy May Be ADocument6 pagesMolecular Hydrogen As An Adjuvant Therapy May Be AM FrederiksenNo ratings yet
- Supplemental Oxygen Administration and Congestive Heart FailureDocument2 pagesSupplemental Oxygen Administration and Congestive Heart FailurejanNo ratings yet
- Jurnal INTER BANTUL DG RIZADocument12 pagesJurnal INTER BANTUL DG RIZAMuhammad Amin KutbiNo ratings yet
- Arterial Blood Gas Analysis - making it easyFrom EverandArterial Blood Gas Analysis - making it easyRating: 4.5 out of 5 stars4.5/5 (4)
- Which Echocardiographic Parameter Is A Better Marker of Volume Status in Hemodialysis PatientsDocument7 pagesWhich Echocardiographic Parameter Is A Better Marker of Volume Status in Hemodialysis PatientsmalisalukmanNo ratings yet
- Any Grade of Relative Overhydration Is Associated With Long-Term Mortality in Patients With Stages 4 and 5 Non-Dialysis Chronic Kidney DiseaseDocument5 pagesAny Grade of Relative Overhydration Is Associated With Long-Term Mortality in Patients With Stages 4 and 5 Non-Dialysis Chronic Kidney DiseaseGiovy SotoNo ratings yet
- Anemia en TceDocument11 pagesAnemia en Tce2133038gNo ratings yet
- Laboratory Risk Factors For Hospital Mortality in AcutelyDocument7 pagesLaboratory Risk Factors For Hospital Mortality in AcutelypmunizNo ratings yet
- Lactato y Perfusion Kattan y GlennDocument5 pagesLactato y Perfusion Kattan y GlennAna Belén Artero CastañoNo ratings yet
- Pi Is 0272638621007721Document12 pagesPi Is 0272638621007721Carlos QuirogaNo ratings yet
- Manual Erythroexchange in Sickle Cell DiseaseDocument10 pagesManual Erythroexchange in Sickle Cell Diseasenigel farageNo ratings yet
- Joosten 2015Document20 pagesJoosten 2015Diego RomeroNo ratings yet
- Fluid Replacement Strategies A171118RQ BLM EditedDocument3 pagesFluid Replacement Strategies A171118RQ BLM EditedJustine ObedNo ratings yet
- Biochemical Markers For Clinical Monitoring of Tissue PerfusionDocument14 pagesBiochemical Markers For Clinical Monitoring of Tissue PerfusionTrọng MPNo ratings yet
- Trend Lab ROIDocument2 pagesTrend Lab ROIaditya brahmantio sujakaNo ratings yet
- Algoritma AB TRANSLATEDocument6 pagesAlgoritma AB TRANSLATEaditya brahmantio sujakaNo ratings yet
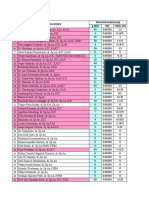
- Penghitungan Total SKS, Sp2 Departemen Anestesi Semester Genap BenarDocument15 pagesPenghitungan Total SKS, Sp2 Departemen Anestesi Semester Genap Benaraditya brahmantio sujakaNo ratings yet
- Npe1 PDFDocument7 pagesNpe1 PDFChavdarNo ratings yet
- Premed ConsiderationDocument9 pagesPremed Considerationaditya brahmantio sujakaNo ratings yet
- TesDocument7 pagesTesaditya brahmantio sujakaNo ratings yet
- 8663 FK UnairDocument2 pages8663 FK Unairaditya brahmantio sujakaNo ratings yet
- Weight-For-Age BOYS: 2 To 5 Years (Z-Scores)Document1 pageWeight-For-Age BOYS: 2 To 5 Years (Z-Scores)d14n4dNo ratings yet
- License PremiumDocument1 pageLicense PremiumNguyen Viet Trung (FPL HCMK13.3)100% (1)
- TesDocument3 pagesTesaditya brahmantio sujakaNo ratings yet
- 5c5791d7a0a80 Early Vs Late RRT 2 PDFDocument25 pages5c5791d7a0a80 Early Vs Late RRT 2 PDFaditya brahmantio sujakaNo ratings yet
- DAS Difficult Intubation Guidelines - Overview: Plan ADocument3 pagesDAS Difficult Intubation Guidelines - Overview: Plan AMaufer AlNo ratings yet
- Judul Acara DLLDocument1 pageJudul Acara DLLaditya brahmantio sujakaNo ratings yet
- 2Document1 page2aditya brahmantio sujakaNo ratings yet
- UNDIANDocument2 pagesUNDIANaditya brahmantio sujakaNo ratings yet
- 04Document12 pages04Zaid AhmadNo ratings yet
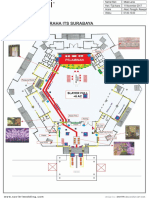
- Peta Graha ItsDocument1 pagePeta Graha Itsaditya brahmantio sujakaNo ratings yet
- Traumatic Hyphema: A Case Series On Admitted Patients in RIMS Hospital, ImphalDocument4 pagesTraumatic Hyphema: A Case Series On Admitted Patients in RIMS Hospital, ImphalheidyNo ratings yet
- RSU Haji Surabaya RSU Haji Surabaya RSU Haji SurabayaDocument1 pageRSU Haji Surabaya RSU Haji Surabaya RSU Haji Surabayaaditya brahmantio sujakaNo ratings yet
- ITS Stage Edit LA 11 NeeeeeDocument1 pageITS Stage Edit LA 11 Neeeeeaditya brahmantio sujakaNo ratings yet
- PTC Course ManualDocument64 pagesPTC Course Manualaditya brahmantio sujakaNo ratings yet
- Traumatic Hyphema: A Case Series On Admitted Patients in RIMS Hospital, ImphalDocument4 pagesTraumatic Hyphema: A Case Series On Admitted Patients in RIMS Hospital, ImphalheidyNo ratings yet
- Slit-Lamp Examination: Key PointsDocument12 pagesSlit-Lamp Examination: Key PointsAndrew Yoshihiro WiryaNo ratings yet
- Trauma OkuliDocument50 pagesTrauma Okuliaditya brahmantio sujakaNo ratings yet
- Analytical Report: Extra-Curricular Activities Name: Tasnuva Radiah Class: Grade 10 Section: 3 Roll No.: 25Document1 pageAnalytical Report: Extra-Curricular Activities Name: Tasnuva Radiah Class: Grade 10 Section: 3 Roll No.: 25Arif AsgarNo ratings yet
- Therapy Is For Everybody: Black Mental HealthDocument22 pagesTherapy Is For Everybody: Black Mental HealthIresha Picot100% (2)
- Glycerol MsdsDocument6 pagesGlycerol MsdsJX Lim0% (1)
- Synthesis EssayDocument8 pagesSynthesis EssayWardah FarukNo ratings yet
- Urgensi Kepemimpinan Transformasional Dan Kecerdasan Emosional Pada Perusahaan Dalam Merespons Pandemi Covid-19Document11 pagesUrgensi Kepemimpinan Transformasional Dan Kecerdasan Emosional Pada Perusahaan Dalam Merespons Pandemi Covid-19Inspektorat KubarNo ratings yet
- PDP2 Heart Healthy LP TDocument24 pagesPDP2 Heart Healthy LP TTisi JhaNo ratings yet
- DrFuhrmans Super Immunity FactsheetDocument2 pagesDrFuhrmans Super Immunity FactsheetPerrela Perrela100% (1)
- DivorceDocument11 pagesDivorceNithesh K MogaveeraNo ratings yet
- Basic Word Structure (MT)Document19 pagesBasic Word Structure (MT)leapphea932No ratings yet
- MMO Chat Filter Bad WordsDocument15 pagesMMO Chat Filter Bad WordsWilliam KravetsNo ratings yet
- 12 2012 TriclabendazoleDocument16 pages12 2012 Triclabendazolenia suwartiningsihNo ratings yet
- The Effect of Narcotic DrugDocument4 pagesThe Effect of Narcotic DrugFasra ChiongNo ratings yet
- No. Kode Dan Nama Kode Diagnosa ICD 10 Nama PenyakitDocument11 pagesNo. Kode Dan Nama Kode Diagnosa ICD 10 Nama PenyakitViki AY15No ratings yet
- Maslow TheoryDocument10 pagesMaslow Theoryraza20100% (1)
- Etp fOR Dasda PDFDocument6 pagesEtp fOR Dasda PDFDesignNo ratings yet
- Book StickerDocument4 pagesBook Stickerilanabiela90No ratings yet
- BDSM Checklist: General InformationDocument6 pagesBDSM Checklist: General Informationmiri100% (1)
- L TyrosineDocument6 pagesL TyrosinecpullerNo ratings yet
- A Quick Trip To 7 Billion Exploring The Timeline PDFDocument9 pagesA Quick Trip To 7 Billion Exploring The Timeline PDFArn Laurence SibagNo ratings yet
- Health 10: 3 Quarter Week 7Document10 pagesHealth 10: 3 Quarter Week 7Maria Rose Tariga Aquino50% (2)
- Hypnotherapy Stress ManagementDocument28 pagesHypnotherapy Stress ManagementSafizi Shahari MizieNo ratings yet
- Maternity Benefit-Employer's ObligationsDocument20 pagesMaternity Benefit-Employer's ObligationsSonika BhatiNo ratings yet
- Causas de Pancitopenia Canina y FelinaDocument12 pagesCausas de Pancitopenia Canina y FelinaMarisol AsakuraNo ratings yet
- WBC DisordersDocument45 pagesWBC DisordersyalahopaNo ratings yet
- Iriga Zone Ibd List: Nabua ADocument20 pagesIriga Zone Ibd List: Nabua AAnonymous dPCnM2a1No ratings yet
- Chevron Phillips Chemical Company Issued Sales SpecificationDocument1 pageChevron Phillips Chemical Company Issued Sales SpecificationSarmiento HerminioNo ratings yet
- Inc Tnai IcnDocument7 pagesInc Tnai IcnDeena MelvinNo ratings yet
- SigmaDur 188-520-550 Msds Hardener PDFDocument17 pagesSigmaDur 188-520-550 Msds Hardener PDFMarcos LaraNo ratings yet
- National Service Training Program 1 Module 10: Drug Abuse and PreventionDocument1 pageNational Service Training Program 1 Module 10: Drug Abuse and PreventionKristine PangahinNo ratings yet
- Weld-On 4 MsdsDocument2 pagesWeld-On 4 MsdsJosué CubilloNo ratings yet