You might also like
- Cross-Training: The Medical Assistant WorkbookFrom EverandCross-Training: The Medical Assistant WorkbookNo ratings yet
- Nursing the Feline PatientFrom EverandNursing the Feline PatientLinda E. SchmeltzerNo ratings yet
- Intern Survival Guide 2011-2012: Office Number: 828-5163, Chief Resident On Call Pager #1709Document10 pagesIntern Survival Guide 2011-2012: Office Number: 828-5163, Chief Resident On Call Pager #1709lkdjsfalNo ratings yet
- QURHRUVTaHNVM3kyS0YtRElWazdCenJ1N3hLVUhTQTl1dm92bWQ4Sk8tOXlxZmNTOW5RNzNNSEJwOXVfa3J0RGQ2ZjR3Y3JpR1dMVFlQTGlmVnFQTTRpbWRFUjljMy1fUmVZSFcxRnYzSlhxeFpmcEJ1SzRuOVA1X1V1WjI2MExQYUc2dzlDTk91aG4=Document10 pagesQURHRUVTaHNVM3kyS0YtRElWazdCenJ1N3hLVUhTQTl1dm92bWQ4Sk8tOXlxZmNTOW5RNzNNSEJwOXVfa3J0RGQ2ZjR3Y3JpR1dMVFlQTGlmVnFQTTRpbWRFUjljMy1fUmVZSFcxRnYzSlhxeFpmcEJ1SzRuOVA1X1V1WjI2MExQYUc2dzlDTk91aG4=Sherif MakarNo ratings yet
- InternDocument19 pagesInternmorasaki003No ratings yet
- On Call Survival Guide PDFDocument78 pagesOn Call Survival Guide PDFMuhammad Nasir AwaisNo ratings yet
- PICU NICU OrientationDocument8 pagesPICU NICU OrientationSony PrabowoNo ratings yet
- Intern Survival Guide Ward 2Document44 pagesIntern Survival Guide Ward 2Keith Swait Zin50% (2)
- Stroger Hospital Intern GuideDocument43 pagesStroger Hospital Intern Guidesgod34No ratings yet
- JMO ED Survival GuideDocument16 pagesJMO ED Survival GuideCrystal ZawNo ratings yet
- MS3 Student Survival GuideDocument18 pagesMS3 Student Survival GuideNoah ThomasNo ratings yet
- ER Tips and Tricks 2017 FINALforPDFDocument23 pagesER Tips and Tricks 2017 FINALforPDFmohamed zeegoNo ratings yet
- Intern Survival Guide The UNC Department of MedicineDocument22 pagesIntern Survival Guide The UNC Department of MedicinecmirceaNo ratings yet
- RMOIH Clinical Handbook Revised JT - 03012022 - Inc Appendix 1 - 2Document114 pagesRMOIH Clinical Handbook Revised JT - 03012022 - Inc Appendix 1 - 2EmeseAgostonNo ratings yet
- Internal Medicine Housestaff Survival GuideDocument61 pagesInternal Medicine Housestaff Survival Guidesgod34No ratings yet
- ATSP Booklet 2023Document26 pagesATSP Booklet 2023Savanthi Carmaline de SilvaNo ratings yet
- Nursing Induction PPT 2Document114 pagesNursing Induction PPT 2Mukesh Choudhary Jat100% (3)
- Orientation ResidenecyDocument18 pagesOrientation ResidenecyReeMii AngeLa100% (1)
- Internal Medicine Clerkship Orientation PackageDocument23 pagesInternal Medicine Clerkship Orientation Packagexjoedu100% (1)
- Survival GuideDocument54 pagesSurvival Guidejoeyblowey88No ratings yet
- Getting Emergency Care Fs EnglishDocument3 pagesGetting Emergency Care Fs EnglishNadir KhanNo ratings yet
- CALLED.TO.SEE.PATIENT v1.1 survival guideDocument111 pagesCALLED.TO.SEE.PATIENT v1.1 survival guideGlen OngNo ratings yet
- Sops Medical OPDDocument6 pagesSops Medical OPDdrisrarz0% (1)
- JFK Muhlenberg Nursing OrientationDocument3 pagesJFK Muhlenberg Nursing OrientationBen HarropNo ratings yet
- House OfficerDocument32 pagesHouse Officerapi-3705046100% (1)
- Antrim Handbook-2018Document223 pagesAntrim Handbook-2018Beaulah HunidzariraNo ratings yet
- Standard Operating ProceduresDocument73 pagesStandard Operating Procedureshailutadeg8798100% (1)
- LBS CV Format 2014Document7 pagesLBS CV Format 2014Jonalyn Almuete RamosoNo ratings yet
- Wm. Jennings Bryan Dorn VAMC Patient Safety TrainingDocument39 pagesWm. Jennings Bryan Dorn VAMC Patient Safety Trainingkamnasharma0907No ratings yet
- Answer For HMIS Exercise Revised Feb, 2010Document30 pagesAnswer For HMIS Exercise Revised Feb, 2010Zerihun BekeleNo ratings yet
- Patient Information Sheet Upper Gastrointerstinal Endoscopy (Egd)Document7 pagesPatient Information Sheet Upper Gastrointerstinal Endoscopy (Egd)monir61No ratings yet
- documentation and common casesDocument26 pagesdocumentation and common casesch wNo ratings yet
- Nursing InductionDocument114 pagesNursing InductionMichael Long92% (26)
- Assess limb weakness and headacheDocument5 pagesAssess limb weakness and headachezhichee91No ratings yet
- Surgeryintern PDFDocument35 pagesSurgeryintern PDFsgod34No ratings yet
- Him Work ExamplesDocument10 pagesHim Work Examplesapi-252670617No ratings yet
- Survival Guide - FY2: Updated by TSZ Lam, Li (Josephine)Document17 pagesSurvival Guide - FY2: Updated by TSZ Lam, Li (Josephine)Anonymous YqCxXQ6wF5No ratings yet
- Lo6 FeedbackDocument2 pagesLo6 Feedbackapi-244230664No ratings yet
- ATI END COMP ReviewDocument19 pagesATI END COMP ReviewTori Roland100% (1)
- ATI 4th Quarter Review - Judith Miller VideosDocument19 pagesATI 4th Quarter Review - Judith Miller VideosTori RolandNo ratings yet
- RMO International Clinical Handbook Revised 05 03 2013Document85 pagesRMO International Clinical Handbook Revised 05 03 2013dragoschrNo ratings yet
- 3638 Scut SheetDocument2 pages3638 Scut Sheetjesse_szymanski3978No ratings yet
- Miccu Intern Survival Guide 2017-2018Document7 pagesMiccu Intern Survival Guide 2017-2018Abdulelah MurshidNo ratings yet
- The Ukfpo Clinical Assessment Examination Guide by Sarishka Singh Plab ResourcesDocument112 pagesThe Ukfpo Clinical Assessment Examination Guide by Sarishka Singh Plab ResourcesWonjoo LeeNo ratings yet
- The AOA Guide:: How To Succeed in The Third-Year ClerkshipsDocument25 pagesThe AOA Guide:: How To Succeed in The Third-Year Clerkshipshector100% (1)
- Intern Ward Survival Guide 2009Document5 pagesIntern Ward Survival Guide 2009mediquest100% (1)
- Manage skin conditions from home with PIFU dermatology appointmentsDocument4 pagesManage skin conditions from home with PIFU dermatology appointmentsGabriela ChiritoiuNo ratings yet
- S Ward Rotation Manual May 2011Document41 pagesS Ward Rotation Manual May 2011nsomenNo ratings yet
- AOA Survival Guide To The 2nd YearDocument18 pagesAOA Survival Guide To The 2nd Yearmediquest100% (1)
- Essential Guide to Surviving Third Year ClerkshipsDocument68 pagesEssential Guide to Surviving Third Year Clerkshipssgod34No ratings yet
- Clerking PatientsDocument7 pagesClerking PatientsJx ChamNo ratings yet
- A Guide To ConsultsDocument36 pagesA Guide To ConsultsspamvarunNo ratings yet
- Report FormattingDocument17 pagesReport FormattingJason LeonaNo ratings yet
- Reference Guide for First Year ResidentsDocument5 pagesReference Guide for First Year Residentsapa0013No ratings yet
- Retractile Testis PDFDocument5 pagesRetractile Testis PDFYuda Saidillah RitongaNo ratings yet
- Specialty Doctor Role in Anaesthetics and ICMDocument17 pagesSpecialty Doctor Role in Anaesthetics and ICMDaniyal AzmatNo ratings yet
- Angiogram Recovery TimeDocument18 pagesAngiogram Recovery TimeDrBertram ForerNo ratings yet
- FistulogramDocument5 pagesFistulogrambshashankkumar123No ratings yet
- The Code Stroke Handbook: Approach to the Acute Stroke PatientFrom EverandThe Code Stroke Handbook: Approach to the Acute Stroke PatientNo ratings yet
- Emergency Medicine Survival Guide: Emergency Medicine Survival Guide for New DoctorsFrom EverandEmergency Medicine Survival Guide: Emergency Medicine Survival Guide for New DoctorsNo ratings yet
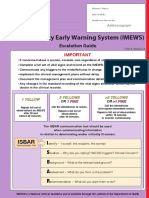
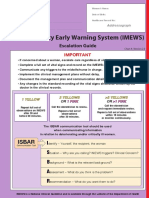
- Imews v2 0 Chart A GenericDocument2 pagesImews v2 0 Chart A GenericdoodrillNo ratings yet
- CV Pack FacDocument53 pagesCV Pack FacdoodrillNo ratings yet
- Ireland VAC checklist for family reunificationDocument4 pagesIreland VAC checklist for family reunificationTushar NairNo ratings yet
- Strong Letter RecommendationDocument2 pagesStrong Letter RecommendationJorge Luis Sánchez Alarcón100% (1)
- Medication Guidelines Vol 1 Antimicrobial Prescribing v1.1 1Document77 pagesMedication Guidelines Vol 1 Antimicrobial Prescribing v1.1 1doodrillNo ratings yet
- NUI Galway Undergraduate Prospectus 2021Document194 pagesNUI Galway Undergraduate Prospectus 2021doodrillNo ratings yet
- Fy1 Survival Guide: Blackpool Teaching Hospitals NHS Foundation TrustDocument38 pagesFy1 Survival Guide: Blackpool Teaching Hospitals NHS Foundation TrustdoodrillNo ratings yet
- National Standards Maternity ServicesDocument188 pagesNational Standards Maternity ServicesdoodrillNo ratings yet
- Fee Collection Information Leaflet Sept 2020 Payment Plans 2020 2021Document1 pageFee Collection Information Leaflet Sept 2020 Payment Plans 2020 2021doodrillNo ratings yet
- Fee Collection Information Leaflet Sept 2020 Payment Plans 2020 2021Document1 pageFee Collection Information Leaflet Sept 2020 Payment Plans 2020 2021doodrillNo ratings yet
- Imews v2 0 Chart A GenericDocument2 pagesImews v2 0 Chart A GenericdoodrillNo ratings yet
- NHO Medical Abbreviations BookletDocument54 pagesNHO Medical Abbreviations BookletffsdfsfdftrertNo ratings yet
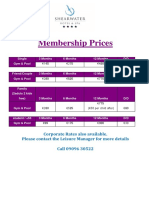
- Membership Prices: Corporate Rates Also Available. Please Contact The Leisure Manager For More Details Call 09096 30522Document1 pageMembership Prices: Corporate Rates Also Available. Please Contact The Leisure Manager For More Details Call 09096 30522doodrillNo ratings yet
- 1 January 2020 Consolidated PayscalesDocument100 pages1 January 2020 Consolidated PayscalesdoodrillNo ratings yet
- National Standards Maternity ServicesDocument188 pagesNational Standards Maternity ServicesdoodrillNo ratings yet
- My Payslip AccessDocument4 pagesMy Payslip AccessdoodrillNo ratings yet
- HBDocument100 pagesHBdoodrillNo ratings yet
- IV to PO Antimicrobial ConversionDocument6 pagesIV to PO Antimicrobial ConversiondoodrillNo ratings yet
- NUI Galway Undergraduate Prospectus 2021Document194 pagesNUI Galway Undergraduate Prospectus 2021doodrillNo ratings yet
- v4 Fee Schedule 2020 2021 002Document9 pagesv4 Fee Schedule 2020 2021 002doodrillNo ratings yet
- Regulations and Information For Candidates MRCPI Obstetrics & GynaecologyDocument21 pagesRegulations and Information For Candidates MRCPI Obstetrics & GynaecologydoodrillNo ratings yet
- Mrcog Part1Document7 pagesMrcog Part1Yogeshwari Pardeshi100% (3)
- Sepsis and Catheter Infections: Early Conversion From IV To Oral AntibioticsDocument4 pagesSepsis and Catheter Infections: Early Conversion From IV To Oral AntibioticsChaim HerreraNo ratings yet
- October 2020 Consolidated Pay ScalesDocument91 pagesOctober 2020 Consolidated Pay ScalesdoodrillNo ratings yet
- Recommended Treatments for Chlamydia and GonorrheaDocument1 pageRecommended Treatments for Chlamydia and GonorrheadoodrillNo ratings yet
- Details, IELTS Academic - 23 January 2021 - Bucharest - Batch 4-1Document4 pagesDetails, IELTS Academic - 23 January 2021 - Bucharest - Batch 4-1doodrillNo ratings yet
- Intermountain IV PO Quick GuideDocument3 pagesIntermountain IV PO Quick GuidedoodrillNo ratings yet
- Sepsis and Catheter Infections: Early Conversion From IV To Oral AntibioticsDocument4 pagesSepsis and Catheter Infections: Early Conversion From IV To Oral AntibioticsChaim HerreraNo ratings yet
- New Zealand Data Sheet for Amoxiclav Multichem Powder InjectionDocument17 pagesNew Zealand Data Sheet for Amoxiclav Multichem Powder InjectiondoodrillNo ratings yet
- Antimicrobial Route of Administration (IV To PO) Therapeutic ConversionDocument1 pageAntimicrobial Route of Administration (IV To PO) Therapeutic ConversiondoodrillNo ratings yet
- Professional Hypnotherapist Diploma For Stress CourseDocument53 pagesProfessional Hypnotherapist Diploma For Stress CourseLuis Del Valle Torregrosa100% (1)
- Presentation 1Document6 pagesPresentation 1Joarlin BianesNo ratings yet
- Vocab 2Document2 pagesVocab 2api-245567970No ratings yet
- Post-Test Sas 13, 14 & 15 Nur 151 Cooa A4: Questions 1 To 10Document2 pagesPost-Test Sas 13, 14 & 15 Nur 151 Cooa A4: Questions 1 To 10Sistine Rose LabajoNo ratings yet
- Leon Guinto Memorial College, Inc.: SCOREDocument4 pagesLeon Guinto Memorial College, Inc.: SCOREPaula Almeyda100% (1)
- Decision Making and Situational Awareness in Neonatal Resuscitation in Low Resource SettingsDocument8 pagesDecision Making and Situational Awareness in Neonatal Resuscitation in Low Resource SettingsJessica MatosNo ratings yet
- Planning ProcessDocument9 pagesPlanning ProcessSimran JosanNo ratings yet
- Case ReportDocument13 pagesCase ReportZaryab Waheed0% (1)
- Exercise 5 Characteristics of Soil ColloidsDocument4 pagesExercise 5 Characteristics of Soil ColloidslexiclesmcgeeNo ratings yet
- Grade 11 - Final Exam PDDocument3 pagesGrade 11 - Final Exam PDGomez Agustin LeslieNo ratings yet
- Photob 2022 0067Document10 pagesPhotob 2022 0067Marilene da Conceicao Felix da SilvaNo ratings yet
- Culture's Influence on Ethics in BusinessDocument4 pagesCulture's Influence on Ethics in Businesssotiredofrepeating0% (2)
- House Democratic Caucus Task Force On Aging and Families LTR To Biden Harris Transition - Geriatrician To COVID Advisory BoardDocument2 pagesHouse Democratic Caucus Task Force On Aging and Families LTR To Biden Harris Transition - Geriatrician To COVID Advisory BoardPeter SullivanNo ratings yet
- Unit 6 Progress Test - Key Vocabulary and Grammar ConceptsDocument2 pagesUnit 6 Progress Test - Key Vocabulary and Grammar ConceptsKatren OrobchukNo ratings yet
- Biodata Peneliti Utama: Rumah Sakit Umum Pusat Dr. Hasan Sadikin BandungDocument2 pagesBiodata Peneliti Utama: Rumah Sakit Umum Pusat Dr. Hasan Sadikin BandungAdriel BenedictNo ratings yet
- Guard RailDocument24 pagesGuard RailRESHMANo ratings yet
- Aromasin 25 MG Coated Tablets SMPCDocument9 pagesAromasin 25 MG Coated Tablets SMPCpedjaljubaNo ratings yet
- Ayurvedic Health & Wellness Center - Divyarishi Arogyam SansthanDocument3 pagesAyurvedic Health & Wellness Center - Divyarishi Arogyam SansthandivyarishiNo ratings yet
- Conduct Disorder and Somatic Health in ChildrenDocument3 pagesConduct Disorder and Somatic Health in ChildrenJeric C. ManaliliNo ratings yet
- Expected Coding and Decoding Questions For Ibps Po MainsDocument11 pagesExpected Coding and Decoding Questions For Ibps Po Mainsvirat kohli86% (7)
- End of Life Care GuideDocument79 pagesEnd of Life Care GuideAbcd TolibasNo ratings yet
- Annual Record of Homœopathic Literature.1875Document395 pagesAnnual Record of Homœopathic Literature.1875GustavoMarceloDareNo ratings yet
- HOPE 1 Module 8Document2 pagesHOPE 1 Module 8Kevin Viernes Garais100% (2)
- HS ConsultantDocument2 pagesHS Consultantdeeman4yahNo ratings yet
- Decision MakingDocument19 pagesDecision MakingJeph ToholNo ratings yet
- The Big Five Personality TestDocument9 pagesThe Big Five Personality TestEVA Rental AdminNo ratings yet
- Abstract of ThesisDocument2 pagesAbstract of ThesisdrkartikeytyagiNo ratings yet
- JIDMR SCOPUS Ke 4 Anwar MallongiDocument4 pagesJIDMR SCOPUS Ke 4 Anwar Mallongiadhe yuniarNo ratings yet
- 4.1.10 Practice Grammar FeedbackDocument10 pages4.1.10 Practice Grammar FeedbackbaileyNo ratings yet
- Pharmacoepidemiology: Origin & EvolutionDocument5 pagesPharmacoepidemiology: Origin & EvolutiongowthamNo ratings yet