You might also like
- Prism MerchandiserTraining Manual - 2Document35 pagesPrism MerchandiserTraining Manual - 2Divya ManivannanNo ratings yet
- Service Agreement TemplateDocument3 pagesService Agreement TemplateSheine Girao-SaponNo ratings yet
- High Yield PediatricsDocument78 pagesHigh Yield Pediatricsjose100% (1)
- Oral Ulcer Diseases DDDocument7 pagesOral Ulcer Diseases DDAmbar ZenNo ratings yet
- How To Track Macros in 3 Simple Steps - EditedDocument21 pagesHow To Track Macros in 3 Simple Steps - EditedTilak Raj100% (1)
- Nullity of MarriageDocument34 pagesNullity of MarriageKhairul Idzwan100% (10)
- Example of Fraudulent MachinationsDocument2 pagesExample of Fraudulent MachinationsJvnRodz P Gmlm100% (4)
- Urine AnalysisDocument69 pagesUrine AnalysisAffan ElahiNo ratings yet
- Chemistry ProjectDocument10 pagesChemistry ProjectVineet Agarwal50% (4)
- UCSP Q1 Lesson 5Document21 pagesUCSP Q1 Lesson 5Isay September50% (2)
- Erythema Multiforme-Oral Variant: Case Report and Review of LiteratureDocument4 pagesErythema Multiforme-Oral Variant: Case Report and Review of LiteratureMarniati JohanNo ratings yet
- Cryogenics Handbook PDFDocument227 pagesCryogenics Handbook PDFmangyanNo ratings yet
- Erosive Lichen Planus of The Oral Cavity: A CaseDocument5 pagesErosive Lichen Planus of The Oral Cavity: A CaseFuad HasanNo ratings yet
- EARC Reportedecaso PDFDocument4 pagesEARC Reportedecaso PDFFed Espiritu Santo GNo ratings yet
- Mouth Ulcers and Diseases of The Oral Cavity: Key PointsDocument7 pagesMouth Ulcers and Diseases of The Oral Cavity: Key PointsAimen ZahidNo ratings yet
- Etiological Factors of Recurrent Aphthous Stomatitis: A Common PerplexityDocument5 pagesEtiological Factors of Recurrent Aphthous Stomatitis: A Common PerplexityRebin AliNo ratings yet
- Oral Manifestations of Behcet's Syndrome: Case ReportDocument6 pagesOral Manifestations of Behcet's Syndrome: Case Report24 februaryNo ratings yet
- Is 20 It 20 Herpes 20 OR20 AphthousDocument11 pagesIs 20 It 20 Herpes 20 OR20 AphthousNindy PutriNo ratings yet
- Oral Ulcers 1Document6 pagesOral Ulcers 1Khushbu MehtaNo ratings yet
- 22-Submission File-35-1-10-20190811Document3 pages22-Submission File-35-1-10-20190811DhevNo ratings yet
- Behçet's Disease: V Kontogiannis, R J PowellDocument9 pagesBehçet's Disease: V Kontogiannis, R J PowellsalclNo ratings yet
- Oral Ulcerative LesionsDocument34 pagesOral Ulcerative LesionsAhmed NajmNo ratings yet
- Bagian Penyakit Mulut FKG Universitas Jember Corresponding Author's EmailDocument5 pagesBagian Penyakit Mulut FKG Universitas Jember Corresponding Author's Emailalya adhanaNo ratings yet
- Minor Case RASDocument41 pagesMinor Case RASNurul SufianNo ratings yet
- Oral Manifestations of Systemic Disease: Autoimmune DiseasesDocument7 pagesOral Manifestations of Systemic Disease: Autoimmune DiseaseshussainNo ratings yet
- Oral UlcerationDocument29 pagesOral UlcerationMINI DHABANo ratings yet
- Oral Ulceration: GP Guide To Diagnosis and Treatment: Stephen Flint Ma, PHD, MB BS, BDS, FDSRCS, Ffdrcsi, FicdDocument9 pagesOral Ulceration: GP Guide To Diagnosis and Treatment: Stephen Flint Ma, PHD, MB BS, BDS, FDSRCS, Ffdrcsi, FicdEstuNo ratings yet
- DE1 RA AbdulrehmanDocument9 pagesDE1 RA Abdulrehmanzuhai martinusNo ratings yet
- Clinical Practice Guidelines For Management of Recurrent Aphthous StomatitisDocument9 pagesClinical Practice Guidelines For Management of Recurrent Aphthous Stomatitislauren pangestuNo ratings yet
- Erythema Multiforme Major: Case Report and Review of LiteratureDocument6 pagesErythema Multiforme Major: Case Report and Review of LiteratureSasa AprilaNo ratings yet
- Lupus ErythematosusDocument3 pagesLupus ErythematosusNoviantiNo ratings yet
- Etiology and Pathophysiology of Recurrent Aphthous Stomatitis: A ReviewDocument7 pagesEtiology and Pathophysiology of Recurrent Aphthous Stomatitis: A ReviewRebin AliNo ratings yet
- Muco-Cutaneous & Aphthous UlcerDocument7 pagesMuco-Cutaneous & Aphthous Ulcerربيد احمد مثنى يحيى كلية طب الاسنان - جامعة عدنNo ratings yet
- Anxiety and Clenching As Contributing Factors of Recurrent Aphthous StomatitisDocument5 pagesAnxiety and Clenching As Contributing Factors of Recurrent Aphthous StomatitisDhevNo ratings yet
- Role of DentistDocument5 pagesRole of Dentisteppy syafriNo ratings yet
- TreatmentDocument5 pagesTreatmentMeva AfinsaNo ratings yet
- Karan Synopsis CLG Apt - UlcDocument23 pagesKaran Synopsis CLG Apt - UlcAnil Subhash RathodNo ratings yet
- Austin: An Unusual Manifestation of Cutaneous Sarcoidosis in The Oral CavityDocument2 pagesAustin: An Unusual Manifestation of Cutaneous Sarcoidosis in The Oral CavityRENITA USWATUN HASANAH 1No ratings yet
- Ulserasi Vesikobulosa Sederhana-Blok 11 FK 3Document229 pagesUlserasi Vesikobulosa Sederhana-Blok 11 FK 3sitiumaiyahNo ratings yet
- T SridharDocument7 pagesT SridharmutiaNo ratings yet
- Case Report: Oral White Sponge Nevus: An Exceptional Differential Diagnosis in ChildhoodDocument3 pagesCase Report: Oral White Sponge Nevus: An Exceptional Differential Diagnosis in ChildhoodAjengRamadhantyNo ratings yet
- Cirugía Oral y Maxilofacial: The Treatment of Oral Lesions in Behc Et's Syndrome: CaseDocument4 pagesCirugía Oral y Maxilofacial: The Treatment of Oral Lesions in Behc Et's Syndrome: Caseandrianiputri916No ratings yet
- Comparing The Effect of Injectable Vitamin B WithDocument6 pagesComparing The Effect of Injectable Vitamin B WithRisa SasmitaNo ratings yet
- Pemphigus VulgarisDocument3 pagesPemphigus VulgarisAdib MuntasirNo ratings yet
- Oral Medicine - Update For The Dental Practitioner.: Mouth Ulcers of More Serious ConnotationDocument5 pagesOral Medicine - Update For The Dental Practitioner.: Mouth Ulcers of More Serious ConnotationGowriNo ratings yet
- Management of Herpes Labialis Triggered by Emotion PDFDocument5 pagesManagement of Herpes Labialis Triggered by Emotion PDFUmmiNo ratings yet
- Herpes Zoster: A Case ReportDocument3 pagesHerpes Zoster: A Case ReportAhmad HaikalNo ratings yet
- Oropharyngeal Candidosis in The Older PatientDocument8 pagesOropharyngeal Candidosis in The Older Patientnugraheni.riniNo ratings yet
- Section Slides 2Document52 pagesSection Slides 2drsafwatismailNo ratings yet
- Surgical Management of Mucocele by Using Diode Laser: Two Case ReportsDocument3 pagesSurgical Management of Mucocele by Using Diode Laser: Two Case ReportsxxxNo ratings yet
- Oral UlcerationDocument10 pagesOral Ulcerationمحمد حسنNo ratings yet
- Endodontic DiagnosisDocument7 pagesEndodontic Diagnosisاحمد عبد الحسن حمود عليNo ratings yet
- White Sponge NevusDocument2 pagesWhite Sponge Nevusbundahara zoomNo ratings yet
- Dentistry: Gardener Syndrome: A Rare Case ReportDocument3 pagesDentistry: Gardener Syndrome: A Rare Case ReportromyNo ratings yet
- Medip,+692 2728 1 CEDocument2 pagesMedip,+692 2728 1 CElaluli lilulaNo ratings yet
- SCMS V34i4 White Lesions in The Oral CavityDocument10 pagesSCMS V34i4 White Lesions in The Oral CavityTasneem Hussiny AbdallahNo ratings yet
- Eosinophilic Ulcer Wiley 2020Document4 pagesEosinophilic Ulcer Wiley 2020Ghea AlmadeaNo ratings yet
- +3a Lamyae Jaich HOPMDocument11 pages+3a Lamyae Jaich HOPMghitakabbageNo ratings yet
- Major Recurrent Aphthous Stomatitis in Mother and Son With Hiv/Aids Infection - CaseDocument4 pagesMajor Recurrent Aphthous Stomatitis in Mother and Son With Hiv/Aids Infection - CaseZita AprilliaNo ratings yet
- K - Wan Hurhazirah Wa Kamil Dsss B 19Document3 pagesK - Wan Hurhazirah Wa Kamil Dsss B 19keshikaNo ratings yet
- Cinnamon Contact StomatitisDocument2 pagesCinnamon Contact StomatitisDwiNo ratings yet
- Syndromes Associated With Aphthous UlcersDocument5 pagesSyndromes Associated With Aphthous UlcersGeorgi GugicevNo ratings yet
- Sar DDDocument5 pagesSar DD26 ThufailNo ratings yet
- Is Caviar Disease (Sublingual Varices) Associated With Trauma?Document2 pagesIs Caviar Disease (Sublingual Varices) Associated With Trauma?Mardiyah PratiwiNo ratings yet
- Acrodermatitis Enteropathica - A Case Report: Rashmi Mittal, Sudha R, Murugan S, Adikrishnan, Shobana S, Anandan SDocument3 pagesAcrodermatitis Enteropathica - A Case Report: Rashmi Mittal, Sudha R, Murugan S, Adikrishnan, Shobana S, Anandan SMarcelitaTaliaDuwiriNo ratings yet
- Erosive Lichen Planus: A Case ReportDocument4 pagesErosive Lichen Planus: A Case ReportNuningK93No ratings yet
- A Brief Review On Classification of Oral Ulcerative LesionsDocument7 pagesA Brief Review On Classification of Oral Ulcerative Lesionsbackup apinNo ratings yet
- Review Article: Oral Ulceration - Aetiopathogenesis, Clinical Diagnosis and Management in The Gastrointestinal ClinicDocument14 pagesReview Article: Oral Ulceration - Aetiopathogenesis, Clinical Diagnosis and Management in The Gastrointestinal ClinicAmira KaddouNo ratings yet
- Oral Medicine: (I. Penyakit Mulut)Document178 pagesOral Medicine: (I. Penyakit Mulut)claudiaciwiNo ratings yet
- Dimensions and Terminal (Unit: MM (Inches) )Document2 pagesDimensions and Terminal (Unit: MM (Inches) )cojoncioNo ratings yet
- English Education Tasks Exclusive BreastfeedingDocument6 pagesEnglish Education Tasks Exclusive BreastfeedingRisa Q. AmaliaNo ratings yet
- Phonic PA450 PDFDocument16 pagesPhonic PA450 PDFhplzNo ratings yet
- The Status Quo of Children On The Global SceneDocument8 pagesThe Status Quo of Children On The Global SceneAruuka SerikbayNo ratings yet
- Ed 1 XAS H 150-175JD 2001-02Document39 pagesEd 1 XAS H 150-175JD 2001-02Victor Ortega SamNo ratings yet
- 2 Infectious Disease EpidemiologyDocument62 pages2 Infectious Disease Epidemiologykindness jawoNo ratings yet
- 40 Days Hypertrophy MesocycleDocument27 pages40 Days Hypertrophy MesocycleAhmed AntarNo ratings yet
- Cylinder Head, Pressure Test (First), D7CDocument4 pagesCylinder Head, Pressure Test (First), D7CAl BimaNo ratings yet
- Transport & Freight ForwardingDocument11 pagesTransport & Freight ForwardingSnigdha AgrawalNo ratings yet
- Cat Fines Guidance PDFDocument4 pagesCat Fines Guidance PDFStefas DimitriosNo ratings yet
- Title: Aim: Apparatus/Materials:: Sound Waves To Determine The Speed of Sound of A Stationary Wave Using HarmonicsDocument8 pagesTitle: Aim: Apparatus/Materials:: Sound Waves To Determine The Speed of Sound of A Stationary Wave Using HarmonicsericaNo ratings yet
- Repair manualTRAKKER ATH-ADH.0003Document1 pageRepair manualTRAKKER ATH-ADH.0003MihajloNo ratings yet
- Prostitution Intervention ProjectDocument7 pagesProstitution Intervention Projectchrisr310No ratings yet
- Caalogo Allen BradleyDocument27 pagesCaalogo Allen BradleyricardoqqNo ratings yet
- Cridia SergipensisDocument19 pagesCridia SergipensisedugersNo ratings yet
- Continuous Monitoring SystemDocument3 pagesContinuous Monitoring SystemsamiNo ratings yet
- P&F NBB3 V3 Z4 BrochureDocument2 pagesP&F NBB3 V3 Z4 BrochureVikrantNo ratings yet
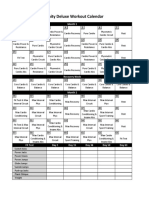
- Insanity Workout Deluxe Calendar SimpleDocument1 pageInsanity Workout Deluxe Calendar SimpleCristian Manuel GonzálezNo ratings yet
- NTE121 Germanium PNP Transistor Audio Frequency Power AmplifierDocument2 pagesNTE121 Germanium PNP Transistor Audio Frequency Power AmplifierDabro FabioNo ratings yet
- YP1 Prescribing MagnificationDocument10 pagesYP1 Prescribing MagnificationLi Chun TatNo ratings yet