You might also like
- Manual For Dental TechniciansDocument186 pagesManual For Dental Techniciansstabik96% (23)
- COVID-19 Medical Vulnerability Indicators: A Predictive, Local Data Model For Equity in Public Health Decision MakingDocument23 pagesCOVID-19 Medical Vulnerability Indicators: A Predictive, Local Data Model For Equity in Public Health Decision MakingWalter MendozaNo ratings yet
- Modeling The Impact of Social Distancing, Testing, Contact TracingDocument31 pagesModeling The Impact of Social Distancing, Testing, Contact TracingIkmal ShahromNo ratings yet
- Impact of COVID-19 Pandemic in Public Mental Health: An Extensive Narrative ReviewDocument21 pagesImpact of COVID-19 Pandemic in Public Mental Health: An Extensive Narrative ReviewValarmathiNo ratings yet
- Journal Pone 0251722Document17 pagesJournal Pone 0251722Augusto RicardiNo ratings yet
- 2020 04 15 20066068v1 FullDocument22 pages2020 04 15 20066068v1 FullcatmewNo ratings yet
- Temporal Clustering of Disorder Events During The COVID-19 PandemicDocument27 pagesTemporal Clustering of Disorder Events During The COVID-19 PandemicBank Data FIA UNW MataramNo ratings yet
- 2021 06 21 21259282v2 FullDocument16 pages2021 06 21 21259282v2 FullPDFReadAndDevelopNo ratings yet
- The Law, Economics, and Governance of Generation Covid-19 Long-HaulDocument80 pagesThe Law, Economics, and Governance of Generation Covid-19 Long-HaulEve AthanasekouNo ratings yet
- Alarid-Escudero Et Al. - 2021 - Dependence of COVID-19 Policies On End - Of-Year Holiday Contacts in Mexico City Metropolitan Area A ModeDocument14 pagesAlarid-Escudero Et Al. - 2021 - Dependence of COVID-19 Policies On End - Of-Year Holiday Contacts in Mexico City Metropolitan Area A ModeferalaesNo ratings yet
- 4902 36233 1 PB1Document14 pages4902 36233 1 PB1Alejandra CanoNo ratings yet
- 2021 07 15 21260543v1 FullDocument36 pages2021 07 15 21260543v1 FullNaufal IndraNo ratings yet
- Experiences, Impacts and Mental Health Functioning During A COVID-19 Outbreak and Lockdown Data From A Diverse New York City Sample of College StudentsDocument17 pagesExperiences, Impacts and Mental Health Functioning During A COVID-19 Outbreak and Lockdown Data From A Diverse New York City Sample of College StudentsAdrian LopezNo ratings yet
- Compliance and Containment in Social Distancing: Mathematical Modeling of COVID-19 Across TownshipsDocument25 pagesCompliance and Containment in Social Distancing: Mathematical Modeling of COVID-19 Across TownshipsScott PymNo ratings yet
- Knowledge, Attitude and Practices (KAP) Towards COVID-19 Pandemic in America: A Preliminary Systematic ReviewDocument14 pagesKnowledge, Attitude and Practices (KAP) Towards COVID-19 Pandemic in America: A Preliminary Systematic ReviewManasi PandaNo ratings yet
- 1 s2.0 S1544319121004891 MainDocument9 pages1 s2.0 S1544319121004891 Mainnizaar ferdianNo ratings yet
- Covid 19 Psychological Effects and Associated Factors in Mexican NursesDocument7 pagesCovid 19 Psychological Effects and Associated Factors in Mexican NursesDelgado Valdez AndrésNo ratings yet
- Epidemiological and Clinical Characteristics of Hospitalized Pediatric Patients With Sars-Cov-2 Infection in Mexico City, MéxicoDocument10 pagesEpidemiological and Clinical Characteristics of Hospitalized Pediatric Patients With Sars-Cov-2 Infection in Mexico City, MéxicoAndrea GarciaNo ratings yet
- 2020 05 12 COVID19 Report 22 PDFDocument21 pages2020 05 12 COVID19 Report 22 PDFMaria Bolivia Rothe CabaNo ratings yet
- Journal - Pone.0244843 PDFDocument35 pagesJournal - Pone.0244843 PDFashenafi woldesenbetNo ratings yet
- The Impact of Fake News On Social Media and Its Influence On Health During The COVID-19 Pandemic A Systematic ReviewDocument11 pagesThe Impact of Fake News On Social Media and Its Influence On Health During The COVID-19 Pandemic A Systematic ReviewZach Daniel Dela CruzNo ratings yet
- COVID-19 and Gender - FinalDocument12 pagesCOVID-19 and Gender - Finalrrhh.ansvNo ratings yet
- s12889 022 13485 2Document11 pagess12889 022 13485 2Pediatrics Department OPD CRMCNo ratings yet
- Anxiety, Worry and Perceived Stress in The World Due To The COVID-19 Pandemic, March 2020. Preliminary ResultsDocument11 pagesAnxiety, Worry and Perceived Stress in The World Due To The COVID-19 Pandemic, March 2020. Preliminary ResultsMayra Brissette Quispe RamosNo ratings yet
- The Effect of The COVID-19 Vaccine On Daily Cases and Deaths Based On Global Vaccine DataDocument12 pagesThe Effect of The COVID-19 Vaccine On Daily Cases and Deaths Based On Global Vaccine DataCorneliu PaschanuNo ratings yet
- A Study To Assess The Post Covid Home Quarantine Stress Level in Second Wave Among General Population in A Selected CommunityDocument3 pagesA Study To Assess The Post Covid Home Quarantine Stress Level in Second Wave Among General Population in A Selected CommunityEditor IJTSRDNo ratings yet
- Msystems 01496-21Document8 pagesMsystems 01496-21Felipe Rojas TraversoNo ratings yet
- Impact of Vaccines Health, Economic and Social PerspectivesDocument15 pagesImpact of Vaccines Health, Economic and Social PerspectivesJV BernNo ratings yet
- Association of Social Distancing and Face Mask Use With Risk of COVID-19Document10 pagesAssociation of Social Distancing and Face Mask Use With Risk of COVID-19Krutarth PatelNo ratings yet
- Association of Social Distancing and Face Mask Use With Risk of COVID-19Document10 pagesAssociation of Social Distancing and Face Mask Use With Risk of COVID-19Krutarth PatelNo ratings yet
- Conspiracy Beliefs, COVID-19 Vaccine Uptake and Adherence To Public Health Interventions During The Pandemic in Europe, Regazzi, 2023Document8 pagesConspiracy Beliefs, COVID-19 Vaccine Uptake and Adherence To Public Health Interventions During The Pandemic in Europe, Regazzi, 2023Ana-Maria BabalauNo ratings yet
- Resea CR H Report ProposalDocument5 pagesResea CR H Report ProposalLigsay, Dianne Rose N.No ratings yet
- SSRN Id3785434Document17 pagesSSRN Id3785434MarksNo ratings yet
- How Individualism Affects The Spread of COVID-19Document3 pagesHow Individualism Affects The Spread of COVID-19Frederick Edward FabellaNo ratings yet
- The Impact of COVID-19 On The Professional and Personal Lives of Pediatric Oncology Social WorkersDocument18 pagesThe Impact of COVID-19 On The Professional and Personal Lives of Pediatric Oncology Social Workersefinales13No ratings yet
- Racial and Ethnic Determinants of Covid 19 RiskDocument13 pagesRacial and Ethnic Determinants of Covid 19 RiskDIVYA RANI KOLLINo ratings yet
- European Journal of Public Health Study on Mental Health Impact of COVID-19 PandemicDocument5 pagesEuropean Journal of Public Health Study on Mental Health Impact of COVID-19 PandemicMCharis MawanNo ratings yet
- Impact of The Covid-19 Pandemic in The Hotspot Communities of Calbayog CityDocument26 pagesImpact of The Covid-19 Pandemic in The Hotspot Communities of Calbayog CityMa. Gina Derla100% (1)
- CovidGlobalizationEpidemics PDFDocument4 pagesCovidGlobalizationEpidemics PDFlefigariNo ratings yet
- From Crisis to Catastrophe: Care, COVID, and Pathways to ChangeFrom EverandFrom Crisis to Catastrophe: Care, COVID, and Pathways to ChangeNo ratings yet
- Alagoz Et Al. (2021) - The Impact of Vaccination To Control COVID-19 Burden in The United States A Simulation Modeling ApproachDocument12 pagesAlagoz Et Al. (2021) - The Impact of Vaccination To Control COVID-19 Burden in The United States A Simulation Modeling ApproachCristian Fernando Sanabria BautistaNo ratings yet
- 2022 - Teppone - Phase Dynamics of The COVID-19 Pandemic - 347-55Document9 pages2022 - Teppone - Phase Dynamics of The COVID-19 Pandemic - 347-55mtepponeNo ratings yet
- Lome-Hurtado Et Al 2021 - Child Mortality RiskDocument12 pagesLome-Hurtado Et Al 2021 - Child Mortality RiskAlejandro Lome HurtadoNo ratings yet
- Jarynowski SR Nowy 2Document51 pagesJarynowski SR Nowy 2Midya JalalNo ratings yet
- 1 s2.0 S0277953621007930 MainDocument12 pages1 s2.0 S0277953621007930 MainRirin KottenNo ratings yet
- Ijerph 17 04148Document12 pagesIjerph 17 04148Lau DíazNo ratings yet
- Departemen Ilmu Kesehatan Masyarakat, Universitas Indonesia, FKM UI Gedung F Lantai 1 Kampus Baru UI, Depok, Jawa Barat 16424Document13 pagesDepartemen Ilmu Kesehatan Masyarakat, Universitas Indonesia, FKM UI Gedung F Lantai 1 Kampus Baru UI, Depok, Jawa Barat 16424dimas kumambangNo ratings yet
- Non-Pharmaceutical Interventions To Combat COVID-19 in The Americas Described Through Daily Sub-National DataDocument8 pagesNon-Pharmaceutical Interventions To Combat COVID-19 in The Americas Described Through Daily Sub-National DataMoema Monteiro BatistaNo ratings yet
- Covid-19 Media Discourse and Public Perception: The Local Construction of A Social Threat in CameroonDocument10 pagesCovid-19 Media Discourse and Public Perception: The Local Construction of A Social Threat in CameroonOpen Access JournalNo ratings yet
- Journal of Public Economics: Pol Campos-Mercade, Armando N. Meier, Florian H. Schneider, Erik WengströmDocument23 pagesJournal of Public Economics: Pol Campos-Mercade, Armando N. Meier, Florian H. Schneider, Erik WengströmM Arif YudhiantoroNo ratings yet
- Role of Mass Media and Public Health Communications in The COVID-19 PandemicDocument13 pagesRole of Mass Media and Public Health Communications in The COVID-19 PandemicZino JamesNo ratings yet
- Biancovilli Et Al. - 2021 - Misinformation On Social Networks During The NovelDocument10 pagesBiancovilli Et Al. - 2021 - Misinformation On Social Networks During The NovelDaniel RomeroNo ratings yet
- Mathematical Modeling of Covid-19 Transmission Dynamics With Social Distance As An InterventionDocument10 pagesMathematical Modeling of Covid-19 Transmission Dynamics With Social Distance As An InterventionPaper PublicationsNo ratings yet
- COVID 19 PandemicDocument4 pagesCOVID 19 PandemiccatmewNo ratings yet
- Covid-19 Requires A Social Medicine Response - Trout and KleinmanDocument4 pagesCovid-19 Requires A Social Medicine Response - Trout and KleinmanNikos KarfakisNo ratings yet
- Economic and Social Impacts of COVID-19 and Public Health Measures - Results From An Anonymous Online Survey in Thailand, Malaysia, The UK, Italy and SloveniaDocument12 pagesEconomic and Social Impacts of COVID-19 and Public Health Measures - Results From An Anonymous Online Survey in Thailand, Malaysia, The UK, Italy and Sloveniapial radakNo ratings yet
- MN #COVID19 Tech DocumentationDocument16 pagesMN #COVID19 Tech DocumentationJill BurcumNo ratings yet
- COVID-19 Survey on educationDocument9 pagesCOVID-19 Survey on educationMonty SharmaNo ratings yet
- FLOOK ET AL - 2021 - Revisão Dos Fatores de Risco, Severida e MortalidadeDocument23 pagesFLOOK ET AL - 2021 - Revisão Dos Fatores de Risco, Severida e MortalidadeVictor FreireNo ratings yet
- Representação Social Covid 19Document18 pagesRepresentação Social Covid 19Mariele MacielNo ratings yet
- A Cross-Cultural Exploratory Analysis of Pandemic Growth - The Case of Covid 19Document22 pagesA Cross-Cultural Exploratory Analysis of Pandemic Growth - The Case of Covid 19gabriel6birsan-1No ratings yet
- Pemphigus Foliaceus: Fig. 29.13BDocument1 pagePemphigus Foliaceus: Fig. 29.13BCristian QuitoNo ratings yet
- Nuclear Medicine Therapy: Side Effects and Complications Luca GiovanellaDocument124 pagesNuclear Medicine Therapy: Side Effects and Complications Luca GiovanellaWhite HeartNo ratings yet
- Phlebotomy Essentials 7th EditionDocument61 pagesPhlebotomy Essentials 7th Editioneric.rodriguez669100% (44)
- Lista Detaliata A Serviciilor Regina MariaDocument69 pagesLista Detaliata A Serviciilor Regina MariaAmreusit SaschimbnumeleNo ratings yet
- Misconceptions About The Use of Genetic Tests in PopulationsDocument4 pagesMisconceptions About The Use of Genetic Tests in PopulationsAneeshNo ratings yet
- Lif Vis Pol Intp Unit 3b-300dpiDocument6 pagesLif Vis Pol Intp Unit 3b-300dpin6wr95xtmjNo ratings yet
- Research Article Smilacina Japonica A. Gray: Antifungal Activity of Crude Extract From The Rhizome and Root ofDocument10 pagesResearch Article Smilacina Japonica A. Gray: Antifungal Activity of Crude Extract From The Rhizome and Root ofJolianna Andrea Beatrice BallezaNo ratings yet
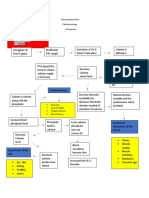
- Hypoparathyroidism PathophysiologyDocument1 pageHypoparathyroidism PathophysiologymaricarNo ratings yet
- Medically Compromised Patients in Prosthodontics - 818 (Autosaved)Document22 pagesMedically Compromised Patients in Prosthodontics - 818 (Autosaved)Suraj ShahNo ratings yet
- The Ultimate Guide To Breathwork 2024Document8 pagesThe Ultimate Guide To Breathwork 2024lucicdNo ratings yet
- Research Paper On Bells PalsyDocument5 pagesResearch Paper On Bells Palsyklbndecnd100% (1)
- List of International Days and WeeksDocument10 pagesList of International Days and WeeksSatram RoopaniNo ratings yet
- Usb Powered Led Strip: User GuideDocument5 pagesUsb Powered Led Strip: User Guidespiritos123456789No ratings yet
- A Survey On Data Mining Techniques For COVID PredictionDocument6 pagesA Survey On Data Mining Techniques For COVID PredictionWARSE Journals100% (2)
- Clobazam As First Add On What Is The Evidence and Experience - Final Deck - 14 Feb 2023Document51 pagesClobazam As First Add On What Is The Evidence and Experience - Final Deck - 14 Feb 2023veerraju tvNo ratings yet
- Interpersonal Relationships Professional Communication Skills For Nurses 6Th Edition Arnold Test Bank Full Chapter PDFDocument29 pagesInterpersonal Relationships Professional Communication Skills For Nurses 6Th Edition Arnold Test Bank Full Chapter PDFhungden8pne100% (11)
- Powerpoint Presentation MIOSHADocument77 pagesPowerpoint Presentation MIOSHAMD AZHER ULLAH BAIGNo ratings yet
- Causes of PtosisDocument3 pagesCauses of PtosisHenry Jonathan BadongenNo ratings yet
- Daily Health MonitoringDocument2 pagesDaily Health MonitoringAntonio CabildoNo ratings yet
- Eat Yourself Smart: Britain Faces Airlift DeadlineDocument64 pagesEat Yourself Smart: Britain Faces Airlift DeadlineNidhi BhartiNo ratings yet
- Info - PathophysiologyDocument6 pagesInfo - PathophysiologyRupert BassigNo ratings yet
- Emergency First Initial Assesment: Monday, October 05, 2020Document50 pagesEmergency First Initial Assesment: Monday, October 05, 2020Agoes TreeyantNo ratings yet
- Activity - Nutrition On The Internet Worksheet 3Document2 pagesActivity - Nutrition On The Internet Worksheet 3Carlo FernandoNo ratings yet
- Pharma Laboratory ExperimentsDocument34 pagesPharma Laboratory Experimentsapi-3748748100% (4)
- الميكروبيولوجى والتحكم فى العدوىDocument115 pagesالميكروبيولوجى والتحكم فى العدوىmahmoud salahNo ratings yet
- Paper 2 Digestive SYSTEM WorksheeetDocument8 pagesPaper 2 Digestive SYSTEM WorksheeetOmar AlfrouhNo ratings yet
- 07 - Towards Elimination DR Gottfried HirnschallDocument24 pages07 - Towards Elimination DR Gottfried HirnschallAjeet LohanaNo ratings yet
- 3 Methods of Food Preservation: Drying, Curing, Chemicals & RadiationDocument5 pages3 Methods of Food Preservation: Drying, Curing, Chemicals & Radiationpainx7No ratings yet
- Understand the Difference Between Omega-3 EPA and DHADocument7 pagesUnderstand the Difference Between Omega-3 EPA and DHASutanto TanakaNo ratings yet