You might also like
- Hemophilia and Von Willebrand Disease: Factor VIII and Von Willebrand FactorFrom EverandHemophilia and Von Willebrand Disease: Factor VIII and Von Willebrand FactorNo ratings yet
- IndexDocument20 pagesIndexMam video songs amd memesNo ratings yet
- Bio ProjectDocument19 pagesBio ProjecthemanthsharmavsNo ratings yet
- HemophiliaDocument3 pagesHemophiliasanghamitra jana0% (1)
- HemophiliaDocument62 pagesHemophiliaMuzlifah Abdul Rahman0% (1)
- Hemophilia A&bDocument33 pagesHemophilia A&bLovelyNo ratings yet
- Biology Project on HaemophiliaDocument15 pagesBiology Project on Haemophiliakirara hatakeNo ratings yet
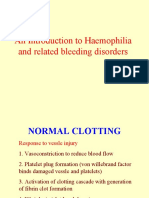
- An Introduction To Haemophilia and Related Bleeding DisordersDocument51 pagesAn Introduction To Haemophilia and Related Bleeding DisordersvaishnaviNo ratings yet
- Hemophilia B - StatPearls - NCBI BookshelfDocument8 pagesHemophilia B - StatPearls - NCBI BookshelflolNo ratings yet
- Haemo PhilliaDocument9 pagesHaemo Philliageorgeloto12No ratings yet
- Hemophilia BIO 2022Document19 pagesHemophilia BIO 2022Gia 0630No ratings yet
- Hemophilia: CPC Cram Like Hell NotesDocument9 pagesHemophilia: CPC Cram Like Hell NotesCitrusNo ratings yet
- Hemophilia FinalDocument4 pagesHemophilia FinalDom Mar Manuel SuicoNo ratings yet
- Heamophilia ResearchDocument21 pagesHeamophilia ResearchRohini SelvarajahNo ratings yet
- CONTENTDocument7 pagesCONTENTDr.Rathod RanjithNo ratings yet
- Hemophilia: Genetics Home ReferenceDocument7 pagesHemophilia: Genetics Home ReferenceSindiFantikaNo ratings yet
- Hemophilia - StatPearls - NCBI BookshelfDocument16 pagesHemophilia - StatPearls - NCBI BookshelflolNo ratings yet
- Hemophilia Narrative PathophysiologyDocument2 pagesHemophilia Narrative PathophysiologyJulianne Jeamer FabroaNo ratings yet
- (FAQs) National Hemophilia Awareness MonthDocument4 pages(FAQs) National Hemophilia Awareness Monthjampogaott100% (1)
- Hemophilia رهفDocument3 pagesHemophilia رهفDrmirfat AlkashifNo ratings yet
- Haemophilia AssignmentDocument2 pagesHaemophilia AssignmentKhadija JaraNo ratings yet
- HemophiliaDocument11 pagesHemophiliaYoga Angga TrinandaNo ratings yet
- HEMOPHILIADocument74 pagesHEMOPHILIASylvia LoongNo ratings yet
- HemophiliaDocument60 pagesHemophiliavibhurocksNo ratings yet
- Bleeding Disorders: Coagulopathy (Also Called Clotting Disorder and Bleeding DisorderDocument5 pagesBleeding Disorders: Coagulopathy (Also Called Clotting Disorder and Bleeding DisorderAyisha EdwinNo ratings yet
- Hemofilia C Dan DisfibrinogenemiaDocument6 pagesHemofilia C Dan DisfibrinogenemiaDavrina DavronNo ratings yet
- HemophiliaDocument19 pagesHemophiliaAtiya HajjajNo ratings yet
- Haemophilia:: What Is Hemophilia?Document3 pagesHaemophilia:: What Is Hemophilia?Abhisek SarkarNo ratings yet
- HemophiliaDocument3 pagesHemophiliaAdrian CoNo ratings yet
- Review Article: Hemophilia - An OverviewDocument9 pagesReview Article: Hemophilia - An OverviewNelly Lutfieta SariNo ratings yet
- Genetics: (Percentage Breakdown of Overall Hemophilia Population by Severity)Document2 pagesGenetics: (Percentage Breakdown of Overall Hemophilia Population by Severity)uikgykNo ratings yet
- Hemophilia ADocument20 pagesHemophilia Adiaharmayukti100% (1)
- Bleeding Disorders: Vascular Defects & Coagulation FactorsDocument11 pagesBleeding Disorders: Vascular Defects & Coagulation FactorslouisNo ratings yet
- Medical Surgical Nursing Understanding HemophiliaDocument2 pagesMedical Surgical Nursing Understanding HemophiliaChieChay DubNo ratings yet
- Hemophilia PPT 3 8 2015Document9 pagesHemophilia PPT 3 8 2015api-286823869No ratings yet
- Hemophilia Can Result In:: TypesDocument9 pagesHemophilia Can Result In:: TypesAntoniusdimasNo ratings yet
- Hemophilia Guide: Causes, Symptoms, TreatmentsDocument3 pagesHemophilia Guide: Causes, Symptoms, TreatmentsMuthoni NdongaNo ratings yet
- HemophiliaDocument62 pagesHemophiliamuhirwa Samuel100% (1)
- Bleeding Disorder: Agustin, Justine Helena Avila, Jed Naziel Bacani, Mitchzel Andrea Bacud, HoneyletteDocument45 pagesBleeding Disorder: Agustin, Justine Helena Avila, Jed Naziel Bacani, Mitchzel Andrea Bacud, HoneyletteJulius FrondaNo ratings yet
- Pendidikan Fisika, Universitas Negeri Jakarta Email: AbstractDocument7 pagesPendidikan Fisika, Universitas Negeri Jakarta Email: AbstractIhda NailulNo ratings yet
- Bleeding Disorders 2Document43 pagesBleeding Disorders 2itsspambroiNo ratings yet
- Haemophilia: Signs and SymptomsDocument17 pagesHaemophilia: Signs and SymptomsAbdul Fattah RinolNo ratings yet
- Bleeding Disorders: Group 6Document41 pagesBleeding Disorders: Group 6Jillian Bermundo LomaadNo ratings yet
- Hemophilia: A Guide to the Genetics, Symptoms and TreatmentDocument13 pagesHemophilia: A Guide to the Genetics, Symptoms and TreatmentSumati Gupta100% (1)
- Clotting Factor VIII (For Hemophilia A) or Clotting Factor IX (For Hemophilia B) Are Infused To Vein PF People With HemophiliaDocument2 pagesClotting Factor VIII (For Hemophilia A) or Clotting Factor IX (For Hemophilia B) Are Infused To Vein PF People With HemophiliaWande AlliNo ratings yet
- Haemophilia: DR Y S Vishnu Vardhan, PGDocument64 pagesHaemophilia: DR Y S Vishnu Vardhan, PGVishnu VardhanNo ratings yet
- HEMOPHILIADocument12 pagesHEMOPHILIAjismi vallachiraNo ratings yet
- Hemophilia Types and TreatmentDocument14 pagesHemophilia Types and TreatmentSophia Loraine Dorone JesuraNo ratings yet
- Ijhd 1 1 4Document5 pagesIjhd 1 1 4Melisa ClaireNo ratings yet
- Biology Investigatory Project: Name: Nasla Abdul Salam Class: 12-L School: Mes Indian SchoolDocument32 pagesBiology Investigatory Project: Name: Nasla Abdul Salam Class: 12-L School: Mes Indian SchoolNasla AbdulsalamNo ratings yet
- HemophiliaDocument4 pagesHemophiliaMechelle ChenNo ratings yet
- Secondary Disorders: Group 3Document33 pagesSecondary Disorders: Group 3Joseph VillamorNo ratings yet
- H P1Document5 pagesH P1mhik296No ratings yet
- Hemophilia B causes, symptoms, and treatmentsDocument2 pagesHemophilia B causes, symptoms, and treatmentsHoger AmediNo ratings yet
- Readings About Hemophilia: Submitted By: Mary Elijah Jane P. PopesDocument10 pagesReadings About Hemophilia: Submitted By: Mary Elijah Jane P. PopesMary Elijah Jane PopesNo ratings yet
- Hemophilia 2Document11 pagesHemophilia 2Dr.Rathod RanjithNo ratings yet
- READING Q - Ans OetDocument22 pagesREADING Q - Ans OetWisdomofGod OfficialNo ratings yet
- Care of HemophiliaDocument7 pagesCare of HemophiliaBasant karn100% (4)
- 4 HemophiliaDocument5 pages4 HemophiliaMary Rose F. MalaluanNo ratings yet
- Hereditary Hemorrhagic Diseases Hemophilia and Von Willebrandt DiseaseDocument12 pagesHereditary Hemorrhagic Diseases Hemophilia and Von Willebrandt Diseaseseries recapNo ratings yet
- Soal Compile Hemato-OncologyDocument25 pagesSoal Compile Hemato-OncologyDapot SianiparNo ratings yet
- Hysterosalpingography A Re - Emerging Study With CDocument7 pagesHysterosalpingography A Re - Emerging Study With CTuyul Yelsi 1No ratings yet
- Antibacterial Activity of Thaaleesaadhi Chooranam Against Human PathogensDocument8 pagesAntibacterial Activity of Thaaleesaadhi Chooranam Against Human PathogensRAJ KUMARNo ratings yet
- Automated Detection of Diabetic Foot With and Without Neuropathy Using Double Density-Dual Tree-Complex Wavelet Transform On Foot ThermogramsDocument32 pagesAutomated Detection of Diabetic Foot With and Without Neuropathy Using Double Density-Dual Tree-Complex Wavelet Transform On Foot ThermogramsLuis Martínez RamírezNo ratings yet
- Unit 3 BK Academic Connections 1 2Document22 pagesUnit 3 BK Academic Connections 1 2api-515535366No ratings yet
- An Interactive Videogame For Arm and Hand Exercise in People With Parkinson's Disease - A Randomized Controlled Trial - Journals - NCBIDocument4 pagesAn Interactive Videogame For Arm and Hand Exercise in People With Parkinson's Disease - A Randomized Controlled Trial - Journals - NCBIWenderson MoraisNo ratings yet
- Matrix On Somatic Disorders: Luzenne Sanchez Jones PSYC 118X Clinical Psyc TTH 4:30-6:00 March 12, 2020Document5 pagesMatrix On Somatic Disorders: Luzenne Sanchez Jones PSYC 118X Clinical Psyc TTH 4:30-6:00 March 12, 2020Monina JonesNo ratings yet
- Lung Volumes and CapacitiesDocument16 pagesLung Volumes and CapacitiesMoses DumbuyaNo ratings yet
- Magsaysay Memorial College of Zambales, IncDocument4 pagesMagsaysay Memorial College of Zambales, IncJoanne CuestaNo ratings yet
- Primary Mitochondrial Myopathies in Childhood 2021 Neuromuscular DisordersDocument10 pagesPrimary Mitochondrial Myopathies in Childhood 2021 Neuromuscular DisordersSuzie Simone Mardones SilvaNo ratings yet
- Impact of Stubble Burning on Air Quality and Human HealthDocument2 pagesImpact of Stubble Burning on Air Quality and Human HealthAshishNo ratings yet
- Excess Deaths Involving CVD in England An Anlysis and ExplainerDocument36 pagesExcess Deaths Involving CVD in England An Anlysis and ExplainerJamie White100% (2)
- Ophthalmology 2Document235 pagesOphthalmology 2yididiyagirma30No ratings yet
- Home Visit Plan and Family Care PlanDocument5 pagesHome Visit Plan and Family Care PlanApril Rose Alivio67% (6)
- Cardiovascular System PharmacothDocument78 pagesCardiovascular System PharmacothKumera Dinkisa ToleraNo ratings yet
- Fiji Communicable Disease Surveillance and Outbreak Response Guidelines 2016 1Document133 pagesFiji Communicable Disease Surveillance and Outbreak Response Guidelines 2016 1roddy narayanNo ratings yet
- WEEK 6 LM#2 LymphaticsDocument5 pagesWEEK 6 LM#2 LymphaticsClyde Tan100% (1)
- OET SpeakingDocument13 pagesOET SpeakingWarangkana96% (23)
- Fayara Aretha Kunaefi Pathophysiology QBD1 FG2Document25 pagesFayara Aretha Kunaefi Pathophysiology QBD1 FG2fayaNo ratings yet
- Case Study Ischemic Heart DiseaseDocument16 pagesCase Study Ischemic Heart DiseaseRawan KhateebNo ratings yet
- A Clinical Decision Support Framework For Heterogeneous Data SourcesDocument10 pagesA Clinical Decision Support Framework For Heterogeneous Data SourcesdineshshaNo ratings yet
- This Is What Happens When You're A Couch Potato: Que-Resultan-Insultantes-Para-Los-HombresDocument6 pagesThis Is What Happens When You're A Couch Potato: Que-Resultan-Insultantes-Para-Los-HombresKatarina JovanovićNo ratings yet
- NHM Goals - Reduce MMR, IMR, TFR & MoreDocument14 pagesNHM Goals - Reduce MMR, IMR, TFR & Morekuruvagadda sagarNo ratings yet
- Ventilasi MekanikDocument47 pagesVentilasi MekanikzahrahNo ratings yet
- Renal Stone Types, Causes and SymptomsDocument29 pagesRenal Stone Types, Causes and Symptomsarim100% (1)
- Rufus Giwa Polytechnic OwoDocument7 pagesRufus Giwa Polytechnic OwoOLATIGBE NASIFNo ratings yet
- Urinary SystemDocument9 pagesUrinary SystemMary Joyce RamosNo ratings yet
- Fracture Healing - Basic Science - Orthobullets PDFDocument2 pagesFracture Healing - Basic Science - Orthobullets PDFMelAcostaNo ratings yet
- CHCAGE002 Implement Falls Prevention Strategies: Mode OneDocument26 pagesCHCAGE002 Implement Falls Prevention Strategies: Mode OnemaxsalNo ratings yet
- Copar (Nursing)Document9 pagesCopar (Nursing)MariaNo ratings yet