You might also like
- 5 Signs Showing You May Suffer From Mental Slavery' by Dr. Amos WilsonDocument4 pages5 Signs Showing You May Suffer From Mental Slavery' by Dr. Amos Wilsonebitechukwudi100% (3)
- Jean Genet - Deathwatch-Faber & Faber (1961) PDFDocument38 pagesJean Genet - Deathwatch-Faber & Faber (1961) PDFValentin MarcosNo ratings yet
- Pastor. The History of The Popes, From The Close of The Middle Ages. 1891. Vol. 31Document540 pagesPastor. The History of The Popes, From The Close of The Middle Ages. 1891. Vol. 31Patrologia Latina, Graeca et Orientalis100% (1)
- Short Answer Questions CHCCSM004Document14 pagesShort Answer Questions CHCCSM004Tmg Preity100% (2)
- RTCDocument27 pagesRTCMaple De los SantosNo ratings yet
- AHP Calculator - Example in The Lecture - 1Document24 pagesAHP Calculator - Example in The Lecture - 1Afranur ErenNo ratings yet
- NCMB 419 Week 11 CU10Document23 pagesNCMB 419 Week 11 CU10GERALDINE GONZALESNo ratings yet
- Blending Online Asynchronous and Synchronous Learning PDFDocument24 pagesBlending Online Asynchronous and Synchronous Learning PDFAnonymous GOUaH7FNo ratings yet
- Assessment of Critical Success Factors For Construction Projects in PakistanDocument13 pagesAssessment of Critical Success Factors For Construction Projects in PakistanAbdul Qayoom Memon100% (1)
- Nurse Education Today: Carole Irwin, Julie Bliss, Karen PooleDocument12 pagesNurse Education Today: Carole Irwin, Julie Bliss, Karen PooleAndi Fajrin PermanaNo ratings yet
- Education and Training of Clinical and Translational Study Investigators and Research Coordinators A Competency-Based Approach.Document10 pagesEducation and Training of Clinical and Translational Study Investigators and Research Coordinators A Competency-Based Approach.Luis FelipeNo ratings yet
- 2020 1830048 PDFDocument14 pages2020 1830048 PDFMarietou SidibeNo ratings yet
- Facilitating Case Studies in Massage Therapy CliniDocument5 pagesFacilitating Case Studies in Massage Therapy ClinijorgenovachrolloNo ratings yet
- The Effectiveness of A Short Cognitive Behavioural TrainingDocument27 pagesThe Effectiveness of A Short Cognitive Behavioural TrainingArinze7No ratings yet
- The Implementation of Mindfulness-Based Cognitive Therapy: Learning From The UK Health Service ExperienceDocument9 pagesThe Implementation of Mindfulness-Based Cognitive Therapy: Learning From The UK Health Service ExperienceRutekNo ratings yet
- Wrightetal Acad Med GMC2012Document11 pagesWrightetal Acad Med GMC2012d_kourkoutasNo ratings yet
- Apn IcnDocument42 pagesApn IcnJohn Mark LingconNo ratings yet
- Clarkson 2004Document4 pagesClarkson 2004Claudia SilveraNo ratings yet
- 4-Global Leadership in IPECP Research An Intro To Co-Creation of BestDocument8 pages4-Global Leadership in IPECP Research An Intro To Co-Creation of BestodetNo ratings yet
- 1734 13 7495 2 10 20180324Document11 pages1734 13 7495 2 10 20180324Lieven VermeulenNo ratings yet
- 10005038measuringprofessionalismasamulti Dimensionalconstruct PDFDocument102 pages10005038measuringprofessionalismasamulti Dimensionalconstruct PDFJanry SimanungkalitNo ratings yet
- Oup Accepted Manuscript 2020Document8 pagesOup Accepted Manuscript 2020Yusril AhmadNo ratings yet
- The Effects of Pay-for-Performance Programs On Health, Health Care Use, and Processes of CareDocument14 pagesThe Effects of Pay-for-Performance Programs On Health, Health Care Use, and Processes of CareMasrun FatanahNo ratings yet
- E013318 FullDocument25 pagesE013318 FullKarina Mejía EscobarNo ratings yet
- How Effect Size Practical Significance Misleads Clinical Practice The Case For Switching To Practical Benefit To Assess Applied Research FindingsDocument13 pagesHow Effect Size Practical Significance Misleads Clinical Practice The Case For Switching To Practical Benefit To Assess Applied Research FindingsDami TepedeNo ratings yet
- Which Patients Miss Appointments With General Practice and The Reasons WhyDocument7 pagesWhich Patients Miss Appointments With General Practice and The Reasons WhyR. H.No ratings yet
- Interpersonal SkillsDocument3 pagesInterpersonal Skillsluciana fardilaNo ratings yet
- Interpersonal SkillsDocument2 pagesInterpersonal SkillsUmarameshKNo ratings yet
- Nurs FPX 4010 Assessment 2 Interview and Interdisciplinary Issue IdentificationDocument4 pagesNurs FPX 4010 Assessment 2 Interview and Interdisciplinary Issue Identificationalicecullen3No ratings yet
- NRSG 7200 EmilyharamesdnpprojectpaperDocument14 pagesNRSG 7200 Emilyharamesdnpprojectpaperapi-582004140No ratings yet
- Acp Led Therapeutic Parenthesis: Advanced Clinical Practice MSCDocument35 pagesAcp Led Therapeutic Parenthesis: Advanced Clinical Practice MSCJoana SilvaNo ratings yet
- Using Field Notes To Evaluate Competencies in Family Medicine Training: A Study of Predictors of IntentionDocument10 pagesUsing Field Notes To Evaluate Competencies in Family Medicine Training: A Study of Predictors of IntentionMirna Liliana Carmona GarciaNo ratings yet
- Are Physiotherapy Students Adequately Prepared To Successfully Gain Employment? Mandy Jones, Judith Mcintyre, Sandra NaylorDocument13 pagesAre Physiotherapy Students Adequately Prepared To Successfully Gain Employment? Mandy Jones, Judith Mcintyre, Sandra NaylorMilan AnandNo ratings yet
- Capability Beliefs On, and Use of Evidence-Based Practice Among Four Health Professional and Student Groups in Geriatric Care: A Cross Sectional StudyDocument16 pagesCapability Beliefs On, and Use of Evidence-Based Practice Among Four Health Professional and Student Groups in Geriatric Care: A Cross Sectional StudynofitaNo ratings yet
- Addington Et Al-2018-Early Intervention in PsychiatryDocument8 pagesAddington Et Al-2018-Early Intervention in PsychiatryLink079No ratings yet
- PDSA Improvement Plan - Kingston General Hospital: Name Institution Course Professor DateDocument5 pagesPDSA Improvement Plan - Kingston General Hospital: Name Institution Course Professor DateNilanjana ChakrabortyNo ratings yet
- 10th Biennial Monash Pharmacy Education Symposium 2019Document68 pages10th Biennial Monash Pharmacy Education Symposium 2019muveszsziNo ratings yet
- 10 1111@jhn 12756Document10 pages10 1111@jhn 12756Federico CilloNo ratings yet
- Career Goals and Student Perceptions of A Post-ProDocument20 pagesCareer Goals and Student Perceptions of A Post-ProCarlos Miguel SumagueNo ratings yet
- Workplace CounsellingDocument5 pagesWorkplace CounsellingUmi AfidaNo ratings yet
- Health Coaching in Pharmacy Practice: A Systematic ReviewDocument14 pagesHealth Coaching in Pharmacy Practice: A Systematic ReviewrujaklutisNo ratings yet
- The Barrier To Implementation of Evidence-Based Practice Among Novice TherapistsDocument11 pagesThe Barrier To Implementation of Evidence-Based Practice Among Novice TherapistsInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- 1-S2.0-S1939865422000315-MainDocument8 pages1-S2.0-S1939865422000315-MainnersrosdianaNo ratings yet
- Competency-Based Medical Education and Continuing Professional Development: A Conceptualization For ChangeDocument8 pagesCompetency-Based Medical Education and Continuing Professional Development: A Conceptualization For ChangeNader Elbokle100% (1)
- Hee Kim, Yeon. Effects of A Work-Based Critical Reflection Program For Novice NursesDocument6 pagesHee Kim, Yeon. Effects of A Work-Based Critical Reflection Program For Novice Nursescantoni1No ratings yet
- Using Staffing Ratios For Workforce Planning: Evidence On Nine Allied Health ProfessionsDocument8 pagesUsing Staffing Ratios For Workforce Planning: Evidence On Nine Allied Health ProfessionstikamdxNo ratings yet
- Py For Qualitu AMJDocument12 pagesPy For Qualitu AMJsunnyNo ratings yet
- Developing A Theory-Based Instrument To Assess The Impact of Continuing Professional Development Activities On Clinical Practice: A Study ProtocolDocument6 pagesDeveloping A Theory-Based Instrument To Assess The Impact of Continuing Professional Development Activities On Clinical Practice: A Study ProtocolSjktraub PahangNo ratings yet
- tmp7BD7 TMPDocument25 pagestmp7BD7 TMPFrontiersNo ratings yet
- 1.evidencebased Practices in Cognitive Behaviour Therapy CBT Case Formulation What Do Practitioners Believe Is Important and What Do They DoDocument21 pages1.evidencebased Practices in Cognitive Behaviour Therapy CBT Case Formulation What Do Practitioners Believe Is Important and What Do They DoGabriela RodriguezNo ratings yet
- Estudio Cualitativo Del Portafolio Que Explora Las Recomendaciones de Los Funcionarios ResponsablesDocument9 pagesEstudio Cualitativo Del Portafolio Que Explora Las Recomendaciones de Los Funcionarios ResponsablesFalconSerfinNo ratings yet
- 2014 Eberhart DNP Final Project PDFDocument81 pages2014 Eberhart DNP Final Project PDFaya PermatasariNo ratings yet
- Participatory Action ResearchDocument9 pagesParticipatory Action ResearchGilbert BaltazarNo ratings yet
- ACGME Outcome ProjectDocument8 pagesACGME Outcome ProjectsrisetyaNo ratings yet
- Graduate Radiographers' Expectations For Role Development e The Potential Impact of Misalignment of Expectation and Valence On Staff Retention and Service ProvisionDocument8 pagesGraduate Radiographers' Expectations For Role Development e The Potential Impact of Misalignment of Expectation and Valence On Staff Retention and Service ProvisionVincent OkekeNo ratings yet
- Evid Based Pract Final Feb 05Document41 pagesEvid Based Pract Final Feb 05Mus OubNo ratings yet
- The Right Place at The Right TimeDocument4 pagesThe Right Place at The Right TimeNian S KoNo ratings yet
- cg6 - Bmjopen-2016-012591Document7 pagescg6 - Bmjopen-2016-012591Mihalache Dan StefanNo ratings yet
- Comms Skills ReportDocument37 pagesComms Skills ReportbrendaNo ratings yet
- IPE Interprofessional EducationDocument10 pagesIPE Interprofessional EducationdewaNo ratings yet
- Jurnal Triad of Concern 2 PDFDocument10 pagesJurnal Triad of Concern 2 PDFKharina AreeistyNo ratings yet
- Education and Professional Development Strategy PDFDocument25 pagesEducation and Professional Development Strategy PDFColeen Ann BagasolNo ratings yet
- Stages of Milestones Implementation: A Template Analysis of 16 Programs Across 4 SpecialtiesDocument32 pagesStages of Milestones Implementation: A Template Analysis of 16 Programs Across 4 Specialtiesjustin76No ratings yet
- InternshipDocument8 pagesInternshipmahmoudNo ratings yet
- Factors Influencing Advanced Practitioners' Ability To Enact Leadership: A Case Study Within Irish HealthcareDocument12 pagesFactors Influencing Advanced Practitioners' Ability To Enact Leadership: A Case Study Within Irish HealthcareKarymeow1No ratings yet
- The Journey To Becoming An Adult Learner: From Dependent To Self-Directed LearningDocument3 pagesThe Journey To Becoming An Adult Learner: From Dependent To Self-Directed LearningAnonymous GOUaH7FNo ratings yet
- Adult Learning in Health Professions Education: Laura L. BieremaDocument14 pagesAdult Learning in Health Professions Education: Laura L. BieremaAnonymous GOUaH7FNo ratings yet
- Emerging Pedagogies For Effective Adult Learning: From Andragogy To HeutagogyDocument6 pagesEmerging Pedagogies For Effective Adult Learning: From Andragogy To HeutagogyAnonymous GOUaH7FNo ratings yet
- Friedman - Medical Humanities in CurriculumDocument3 pagesFriedman - Medical Humanities in CurriculumAnonymous GOUaH7FNo ratings yet
- Contribution To Setting Up A Sustainable Learning in An Eco-Neighbourhood Development Plan Based On "Serious Game"Document16 pagesContribution To Setting Up A Sustainable Learning in An Eco-Neighbourhood Development Plan Based On "Serious Game"Anonymous GOUaH7FNo ratings yet
- 4CID Model in Communication Skills CourseDocument8 pages4CID Model in Communication Skills CourseAnonymous GOUaH7FNo ratings yet
- Koczwara - Et - Al-2012-Medical - Education - Dr. SyntiaDocument10 pagesKoczwara - Et - Al-2012-Medical - Education - Dr. SyntiaAnonymous GOUaH7FNo ratings yet
- Assessment of Professionalism A Consolidation of Current ThinkingDocument6 pagesAssessment of Professionalism A Consolidation of Current ThinkingAnonymous GOUaH7FNo ratings yet
- 4CID Model AMEE GuideDocument17 pages4CID Model AMEE GuideAnonymous GOUaH7FNo ratings yet
- Situational Judgement Tests in Medical Education and Training: Research, Theory and Practice: AMEE Guide No. 100Document16 pagesSituational Judgement Tests in Medical Education and Training: Research, Theory and Practice: AMEE Guide No. 100Anonymous GOUaH7FNo ratings yet
- Pengaruh Metode Kombinasi Jigsaw Dan Concept Mapping Terhadap Prestasi BelajarDocument12 pagesPengaruh Metode Kombinasi Jigsaw Dan Concept Mapping Terhadap Prestasi BelajarAnonymous GOUaH7FNo ratings yet
- Blended Learning' As An Effective Teaching and Learning Strategy in Clinical Medicine: A Comparative Cross-Sectional University-Based StudyDocument6 pagesBlended Learning' As An Effective Teaching and Learning Strategy in Clinical Medicine: A Comparative Cross-Sectional University-Based StudyAnonymous GOUaH7FNo ratings yet
- Blended Learning For PostgraduateDocument7 pagesBlended Learning For PostgraduateAnonymous GOUaH7FNo ratings yet
- CSL Lab PDFDocument8 pagesCSL Lab PDFAnonymous GOUaH7FNo ratings yet
- Ats Scholar.2020 0046psDocument10 pagesAts Scholar.2020 0046psAnonymous GOUaH7FNo ratings yet
- Blended Learning For Medical ProfessionalsDocument2 pagesBlended Learning For Medical ProfessionalsAnonymous GOUaH7FNo ratings yet
- 26Document7 pages26Rinandar MusliminNo ratings yet
- ARTS10 WEEK3 A10PL-Ih-1Document15 pagesARTS10 WEEK3 A10PL-Ih-1rene nonatoNo ratings yet
- Marketing Strategy of Pepsi AssaignmentDocument48 pagesMarketing Strategy of Pepsi AssaignmentZekria Noori AfghanNo ratings yet
- Role-Play #1: Saving Energy: WellDocument4 pagesRole-Play #1: Saving Energy: WellDaniel VasquezNo ratings yet
- Theatres: 2 HellDocument10 pagesTheatres: 2 HellmooolkaNo ratings yet
- A. Biblical Studies C. Systematic Theology: TH THDocument2 pagesA. Biblical Studies C. Systematic Theology: TH TH謝樂知No ratings yet
- Happy Orere-Amadu 7&17 Professional CVDocument4 pagesHappy Orere-Amadu 7&17 Professional CVapi-284326863No ratings yet
- PIL Lecture Notes - Week 1Document3 pagesPIL Lecture Notes - Week 1Yoshita SoodNo ratings yet
- Chinese DragonDocument2 pagesChinese DragonwaiNo ratings yet
- Rizal Report - 19TH CenturyDocument25 pagesRizal Report - 19TH CenturyNamja PyosiNo ratings yet
- Jaltarang Instruments ShreyaDocument24 pagesJaltarang Instruments ShreyaKaushal DidwaniaNo ratings yet
- CBSE Class 2 EVS Our FestivalsDocument3 pagesCBSE Class 2 EVS Our FestivalsRakesh Agarwal100% (1)
- Rahail's ResumeDocument3 pagesRahail's ResumeRahailSalamatNo ratings yet
- An Informational Guide To Young Children's Outdoor Play SpacesDocument59 pagesAn Informational Guide To Young Children's Outdoor Play SpacesCristian NiculitaNo ratings yet
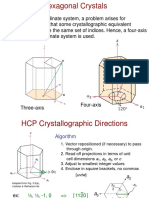
- Chap3.3 HexCrystal DirectionsDocument6 pagesChap3.3 HexCrystal DirectionsJeonghun LeeNo ratings yet
- Library Etymology - WiktionaryDocument4 pagesLibrary Etymology - WiktionarySamuel D. AdeyemiNo ratings yet
- Law437 Basic Features All PrintedDocument121 pagesLaw437 Basic Features All PrintedcfgqymsqdhNo ratings yet
- The Export Performance of Emerging Economy Firms The Influence of FirmDocument13 pagesThe Export Performance of Emerging Economy Firms The Influence of FirmJulio Jefrie Rojas SaraviaNo ratings yet
- Solution of IWTDocument6 pagesSolution of IWTreetikaNo ratings yet
- Mechanical Properties of Astm A572 Grade 65 SteelDocument123 pagesMechanical Properties of Astm A572 Grade 65 Steelcesarceron2003No ratings yet
- A Study On Customer Satisfaction Towards Parachute Hair Oil With Reference To Coimbatore CityDocument3 pagesA Study On Customer Satisfaction Towards Parachute Hair Oil With Reference To Coimbatore CityAbner Alexander Luiz86% (7)
- Chapter 1 To 3Document26 pagesChapter 1 To 3Hyman Jay Blanco100% (1)
- Tools Surveilans Hais Pencegahan & Pengendalian Infeksi 2021Document127 pagesTools Surveilans Hais Pencegahan & Pengendalian Infeksi 2021Yohana AnjaNo ratings yet
- Semi-Final NotesDocument6 pagesSemi-Final NotesRezel FuntilarNo ratings yet