You might also like
- Application of Four-Dimension Criteria To Assess Rigour of Qualitative Research in Emergency MedicineDocument11 pagesApplication of Four-Dimension Criteria To Assess Rigour of Qualitative Research in Emergency MedicinegvhNo ratings yet
- 2019 Article 894Document12 pages2019 Article 894Elfina NataliaNo ratings yet
- Primary Health Care Literature ReviewDocument4 pagesPrimary Health Care Literature Reviewafdtbluwq100% (1)
- Jurnal Retensi 2Document20 pagesJurnal Retensi 2tasyaNo ratings yet
- The Relationship Between Characteristics of Context and Research Utilization in A Pediatric SettingDocument10 pagesThe Relationship Between Characteristics of Context and Research Utilization in A Pediatric SettingReynaldi Esa RamadhanNo ratings yet
- Development Implementation and Evaluation of A CliDocument10 pagesDevelopment Implementation and Evaluation of A CliMinh HoangNo ratings yet
- 2014 Article 200Document7 pages2014 Article 200ubiktrash1492No ratings yet
- Ijerph 19 07327Document14 pagesIjerph 19 07327NataliaNo ratings yet
- The Integration of Primary Health Care Services A Systematic Literature ReviewDocument5 pagesThe Integration of Primary Health Care Services A Systematic Literature ReviewrdssibwgfNo ratings yet
- Introduction to Clinical Effectiveness and Audit in HealthcareFrom EverandIntroduction to Clinical Effectiveness and Audit in HealthcareNo ratings yet
- Employee engagement through a healthy workplace strategyDocument8 pagesEmployee engagement through a healthy workplace strategykapileshwariNo ratings yet
- Mzi040 PDFDocument6 pagesMzi040 PDFselamat parminNo ratings yet
- Mzi040 PDFDocument6 pagesMzi040 PDFselamat parminNo ratings yet
- Tonursj 11 108 PDFDocument16 pagesTonursj 11 108 PDFAnonymous OzgEr1FNvdNo ratings yet
- 556-Appropriateness of Clinical Decision Support - Final White Paper-Wei WuDocument15 pages556-Appropriateness of Clinical Decision Support - Final White Paper-Wei Wuapi-398506399No ratings yet
- Conjoint in HEALTH ResearchDocument17 pagesConjoint in HEALTH ResearchDiana Tan May KimNo ratings yet
- A Process-Based Framework To Guide Nurse Practitioners Integration Into Primary Healthcare Teams: Results From A Logic AnalysisDocument11 pagesA Process-Based Framework To Guide Nurse Practitioners Integration Into Primary Healthcare Teams: Results From A Logic AnalysisFlorsie MirandaNo ratings yet
- TDF On Primary CareDocument16 pagesTDF On Primary CareLammeessaa Assefa AyyaanaNo ratings yet
- Conceptual Frameworks For Health Systems Performance - A Quest For Effectiveness, Quality, and ImprovementDocument22 pagesConceptual Frameworks For Health Systems Performance - A Quest For Effectiveness, Quality, and ImprovementRegina GuzmanNo ratings yet
- Editorial: Evidence-Based Decision Making in Occupational HealthDocument2 pagesEditorial: Evidence-Based Decision Making in Occupational HealthNutanNo ratings yet
- Art - 253A10.1186 - 252Fs13049 017 0362 4Document8 pagesArt - 253A10.1186 - 252Fs13049 017 0362 4Fadhilah SudinNo ratings yet
- Cost-Effectiveness Analysis Alongside Clinical Trials II-An ISPOR Good Research Practices Task Force ReportDocument30 pagesCost-Effectiveness Analysis Alongside Clinical Trials II-An ISPOR Good Research Practices Task Force Reportelisabeth jawanNo ratings yet
- Mapping of Multiple Criteria For Priority Setting of Health Interventions: An Aid For Decision MakersDocument7 pagesMapping of Multiple Criteria For Priority Setting of Health Interventions: An Aid For Decision MakerstemesgenNo ratings yet
- Newsletter - July10 - Version01 4Document4 pagesNewsletter - July10 - Version01 4Reid BeelsNo ratings yet
- Critical Appraisal For Public Health: A New ChecklistDocument7 pagesCritical Appraisal For Public Health: A New Checklistkristina dewiNo ratings yet
- Effects of Worksite Health Promotion Interventions On Employee Diets: A Systematic ReviewDocument7 pagesEffects of Worksite Health Promotion Interventions On Employee Diets: A Systematic ReviewUtami LukitaNo ratings yet
- s12913 023 09612 3Document15 pagess12913 023 09612 3imidazolaNo ratings yet
- Hospital BenchmarkingDocument11 pagesHospital BenchmarkingDana ApostolNo ratings yet
- Published Researches in The Year 2010Document16 pagesPublished Researches in The Year 2010hsrimediaNo ratings yet
- Health RecordsDocument36 pagesHealth RecordsMatthew NdetoNo ratings yet
- Evidence Supporting PF As A Resource For Practice ImprovementDocument3 pagesEvidence Supporting PF As A Resource For Practice ImprovementJuliahNo ratings yet
- Ispor Alonside TrialsDocument12 pagesIspor Alonside TrialsJulivaiNo ratings yet
- The Barrier To Implementation of Evidence-Based Practice Among Novice TherapistsDocument11 pagesThe Barrier To Implementation of Evidence-Based Practice Among Novice TherapistsInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Health Human Resources Planning and The Production of HealthDocument6 pagesHealth Human Resources Planning and The Production of HealthMeiriele TavaresNo ratings yet
- Team Base Research (Assignment)Document3 pagesTeam Base Research (Assignment)Frank IbiokNo ratings yet
- International Journal of Health Care Quality AssuranceDocument12 pagesInternational Journal of Health Care Quality AssuranceMirza0% (1)
- Fasilita RefDocument10 pagesFasilita RefsukrangNo ratings yet
- E28716V9 HRMT20024 Assessment2Document16 pagesE28716V9 HRMT20024 Assessment2bitetNo ratings yet
- Understanding The Components of Quality Improvement Collaboratives A Systematic Literature ReviewDocument7 pagesUnderstanding The Components of Quality Improvement Collaboratives A Systematic Literature Reviewc5qrve03No ratings yet
- A Brief Analysis of The Connection Between EBP and The Quadruple AimDocument5 pagesA Brief Analysis of The Connection Between EBP and The Quadruple AimChacha PeterNo ratings yet
- Health Workforce Skill Mix and Task Shifting in Low Income Countries: A Review of Recent EvidenceDocument11 pagesHealth Workforce Skill Mix and Task Shifting in Low Income Countries: A Review of Recent Evidenceshouka.inNo ratings yet
- Systematic Review Protocol of Interventions To Improve The Psychological Well-Being of General PractitionersDocument6 pagesSystematic Review Protocol of Interventions To Improve The Psychological Well-Being of General PractitionersKasep PisanNo ratings yet
- How Can Clinical Epidemiology Better Support Evidence-Based Guidelines and Policies in Low-Income CountriesDocument3 pagesHow Can Clinical Epidemiology Better Support Evidence-Based Guidelines and Policies in Low-Income CountriesEko Wahyu AgustinNo ratings yet
- Lizarondo 2014 PerformanceEvalDocument13 pagesLizarondo 2014 PerformanceEvalKamila AmmarNo ratings yet
- Costs and Cost Effectiveness of Community Health WorkersDocument16 pagesCosts and Cost Effectiveness of Community Health WorkersMike TeeNo ratings yet
- Community Health Nurses ' Learning Needs in Relation To The Canadian Community Health Nursing Standards of Practice: Results From A Canadian SurveyDocument10 pagesCommunity Health Nurses ' Learning Needs in Relation To The Canadian Community Health Nursing Standards of Practice: Results From A Canadian SurveyPawan MishraNo ratings yet
- Knowledge Translation of Research Findings: Debate Open AccessDocument17 pagesKnowledge Translation of Research Findings: Debate Open AccessHANo ratings yet
- A Comparative Analysis of Six Audit Systems For Mental Health NursingDocument10 pagesA Comparative Analysis of Six Audit Systems For Mental Health NursingByArdieNo ratings yet
- Performance Measures For Mental Healthcare in Singapore: CommentaryDocument6 pagesPerformance Measures For Mental Healthcare in Singapore: Commentarypaijosuseno2242No ratings yet
- Healthcare 08 00354Document16 pagesHealthcare 08 00354Andi Fajrin PermanaNo ratings yet
- KN ClinicalGuidelines2Document2 pagesKN ClinicalGuidelines2Mhmd IrakyNo ratings yet
- Oral Health Guidelines in The Primary Care PoliciesDocument31 pagesOral Health Guidelines in The Primary Care Policiesgolimohamadzade1377No ratings yet
- Measuring Impact of Health Research InvestmentsDocument16 pagesMeasuring Impact of Health Research InvestmentsGesler Pilvan SainNo ratings yet
- Asamani Et Al 2021 - Activity Standards and Standard Workloads in Ghana - Healthcare-09-00332-V2Document38 pagesAsamani Et Al 2021 - Activity Standards and Standard Workloads in Ghana - Healthcare-09-00332-V2JAMES AVOKA AsamaniNo ratings yet
- 08-06-2021-1623140416-6-Impact - Ijrbm-1. Ijrbm - "HR Retention Practices in Hospitals" - Validating The Measurement ScaleDocument8 pages08-06-2021-1623140416-6-Impact - Ijrbm-1. Ijrbm - "HR Retention Practices in Hospitals" - Validating The Measurement ScaleImpact JournalsNo ratings yet
- Etoshow QuityDocument8 pagesEtoshow QuityAr JayNo ratings yet
- Literature Review Developing Competencies For Health Promotion Deliverable 3bDocument10 pagesLiterature Review Developing Competencies For Health Promotion Deliverable 3bxfeivdsifNo ratings yet
- Eview F Herapeutics: Economic Evaluations of Clinical Pharmacy Services: 2006 - 2010Document23 pagesEview F Herapeutics: Economic Evaluations of Clinical Pharmacy Services: 2006 - 2010Igor SilvaNo ratings yet
- Bridges, Hauber Et Al. 2011 - Conjoint Analysis Applications in Health-A PDFDocument11 pagesBridges, Hauber Et Al. 2011 - Conjoint Analysis Applications in Health-A PDFali rezaNo ratings yet
- Capability Beliefs On, and Use of Evidence-Based Practice Among Four Health Professional and Student Groups in Geriatric Care: A Cross Sectional StudyDocument16 pagesCapability Beliefs On, and Use of Evidence-Based Practice Among Four Health Professional and Student Groups in Geriatric Care: A Cross Sectional StudynofitaNo ratings yet
- Global Health Diplomacy Competency ModelDocument166 pagesGlobal Health Diplomacy Competency ModeltikamdxNo ratings yet
- Global Competency Educating The WorldDocument6 pagesGlobal Competency Educating The WorldtikamdxNo ratings yet
- Using Staffing Ratios For Workforce Planning: Evidence On Nine Allied Health ProfessionsDocument8 pagesUsing Staffing Ratios For Workforce Planning: Evidence On Nine Allied Health ProfessionstikamdxNo ratings yet
- Interpreting Diagnostic Test For Sars Cov 2 MARZODocument2 pagesInterpreting Diagnostic Test For Sars Cov 2 MARZOAsunción Anco RosalesNo ratings yet
- Piis0140673615008387 PDFDocument13 pagesPiis0140673615008387 PDFPedro CRuzNo ratings yet
- Pengalaman Penanganan Covid-19 dan Urgensi Reformasi Sistem KesehatanDocument16 pagesPengalaman Penanganan Covid-19 dan Urgensi Reformasi Sistem KesehatantikamdxNo ratings yet
- Global Health Diplomacy Competency ModelDocument166 pagesGlobal Health Diplomacy Competency ModeltikamdxNo ratings yet
- Global Health Diplomacy Competency ModelDocument166 pagesGlobal Health Diplomacy Competency ModeltikamdxNo ratings yet
- Global Supply of Health Professionals: Review ArticleDocument8 pagesGlobal Supply of Health Professionals: Review ArticletikamdxNo ratings yet
- Sustainable Cities Health at The Heart of Urban Development Low Res 12JUL18Document14 pagesSustainable Cities Health at The Heart of Urban Development Low Res 12JUL18tikamdxNo ratings yet
- TOEFL PBT BookDocument93 pagesTOEFL PBT Bookaqua_6978% (9)
- TOEFL PBT BookDocument93 pagesTOEFL PBT Bookaqua_6978% (9)
- Weekly Home Learning Plan For Grade 7 MAPEH 7 Quarter IVDocument10 pagesWeekly Home Learning Plan For Grade 7 MAPEH 7 Quarter IVMiguilaMaldita GamasNo ratings yet
- 2023 ST HELENA BAY Course DatesDocument2 pages2023 ST HELENA BAY Course DatesNelson TolosseNo ratings yet
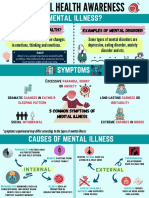
- Mental Health AwarenessDocument2 pagesMental Health Awarenessfarhatulhanimzulkifl100% (2)
- Relationships Between Beliefs About Medications and AdherenceDocument8 pagesRelationships Between Beliefs About Medications and Adherencenoor cahayaNo ratings yet
- The Effect of 5S On Employee Performance: An Empirical Study Among Lebanese HospitalsDocument7 pagesThe Effect of 5S On Employee Performance: An Empirical Study Among Lebanese HospitalsMuthu BaskaranNo ratings yet
- Pusher Syndrome-1Document39 pagesPusher Syndrome-1yenrilisnaNo ratings yet
- 986 Assessment of New Born NursingDocument91 pages986 Assessment of New Born NursingkrishnaNo ratings yet
- Angelbiss ManualDocument51 pagesAngelbiss ManualSineepa PLOYNo ratings yet
- Firefighter Candidate Prep GuideDocument21 pagesFirefighter Candidate Prep GuideEric Levy100% (1)
- Workplace Wellbeing Update For Busy Leaders and HR ProfessionalsDocument25 pagesWorkplace Wellbeing Update For Busy Leaders and HR ProfessionalsTamara Abdel RahimNo ratings yet
- Products You Can Cannot Mix 20Document2 pagesProducts You Can Cannot Mix 20RiaCasidsidNo ratings yet
- Mastering Your Fears Transforming Fear Into Effective Energies by Bobby G. Bodenhamer L. Michael HallDocument162 pagesMastering Your Fears Transforming Fear Into Effective Energies by Bobby G. Bodenhamer L. Michael HallparagnkpatelNo ratings yet
- Tle 8-Beautycare-Q4-M7Document8 pagesTle 8-Beautycare-Q4-M7Belinda OrigenNo ratings yet
- SDS-Dolphin Screen WashDocument10 pagesSDS-Dolphin Screen WashLiz CNo ratings yet
- "Nagsusuka Ang Anak Ko.": Nursing Care ProcessDocument2 pages"Nagsusuka Ang Anak Ko.": Nursing Care Processgeorgia50% (2)
- Junior High PE and Health Exam QuestionsDocument4 pagesJunior High PE and Health Exam QuestionsSarah Visperas RogasNo ratings yet
- Supplier Id Principal Manager: Price List Farma Maret 2020Document48 pagesSupplier Id Principal Manager: Price List Farma Maret 2020Maria Kristiyani TinentiNo ratings yet
- Biopharmaceutics and Pharmacokinetics of The Macrolide Antibiotic ... (Pdfdrive)Document231 pagesBiopharmaceutics and Pharmacokinetics of The Macrolide Antibiotic ... (Pdfdrive)rajakumarudu11No ratings yet
- The Number of Grade 10 Serenity Students of School Year 2022-2023 at San Pedro National High School Affected by Verbal Abuse - Irritability, Stress, and Self-Harm - Anxiety - Research ProposalDocument5 pagesThe Number of Grade 10 Serenity Students of School Year 2022-2023 at San Pedro National High School Affected by Verbal Abuse - Irritability, Stress, and Self-Harm - Anxiety - Research ProposalMa Lourdez BayanNo ratings yet
- Test Bank For Health Psychology 2 e 2nd Edition Deborah Fish RaginDocument34 pagesTest Bank For Health Psychology 2 e 2nd Edition Deborah Fish RaginpudgyoverburnnggNo ratings yet
- Draw AnatomyDocument117 pagesDraw AnatomydsaNo ratings yet
- Case StudyDocument3 pagesCase StudyNovelyn B. PlaniaNo ratings yet
- Workplace Inspection ProcedureDocument3 pagesWorkplace Inspection ProcedureKaavi MaharajNo ratings yet
- Pre-Employment Requirements - KFC S-FZDocument1 pagePre-Employment Requirements - KFC S-FZJenalyn AmarNo ratings yet
- Lewinsohn 1975Document3 pagesLewinsohn 1975serenadenightNo ratings yet
- Jurnal Mina Sains ISSN: 2407-9030 Volume 2 Nomor 2, Oktober 2016 71Document9 pagesJurnal Mina Sains ISSN: 2407-9030 Volume 2 Nomor 2, Oktober 2016 71yudhoNo ratings yet
- Sas-3.pmls1-Mls 037Document9 pagesSas-3.pmls1-Mls 037Michael MarzonNo ratings yet
- Menopause Thesis StatementDocument6 pagesMenopause Thesis Statementallisonweavereugene100% (2)
- AL Ehsan Welfare Eye Hospital Volunteer ReportDocument21 pagesAL Ehsan Welfare Eye Hospital Volunteer ReportKaamla BajwaNo ratings yet
- Faith in Time of CrisisDocument4 pagesFaith in Time of CrisisCerry Herradura BaldonadoNo ratings yet