You might also like
- Neuropsychological AssessmentDocument112 pagesNeuropsychological AssessmentCatalina BuzduganNo ratings yet
- Functional Assessment Interview and ObservationDocument20 pagesFunctional Assessment Interview and ObservationNatasha Bonybutt Khoo100% (1)
- Endurance Training (NSCA)Document22 pagesEndurance Training (NSCA)Jad Adrian Washif60% (5)
- Selective MutismDocument2 pagesSelective MutismTee Kok KeongNo ratings yet
- Medication Assisted Treatment of Opioid Use.2Document13 pagesMedication Assisted Treatment of Opioid Use.2tatanmenaNo ratings yet
- Ghadhiyali's TherapyDocument9 pagesGhadhiyali's TherapyPrajwal Mk100% (1)
- Med Surg Questions Oct 25 Angela DeVarsoDocument38 pagesMed Surg Questions Oct 25 Angela DeVarsonochip10100% (1)
- PacemakersDocument19 pagesPacemakersAswathy RCNo ratings yet
- Clinical Manual of Psychosomatic Medicine Rundell - Wise HandbookDocument351 pagesClinical Manual of Psychosomatic Medicine Rundell - Wise HandbookAdriana Mendoza67% (3)
- 02 - Biological WWTP II - Moving Bed Biofilm ReactorDocument45 pages02 - Biological WWTP II - Moving Bed Biofilm ReactorAquasoul CoNo ratings yet
- Pharmacoepidemiology, Pharmacoeconomics,PharmacovigilanceFrom EverandPharmacoepidemiology, Pharmacoeconomics,PharmacovigilanceRating: 3 out of 5 stars3/5 (1)
- CariesDocument99 pagesCariesKaran Arora100% (1)
- Oncology Nursing Exam and RationaleDocument9 pagesOncology Nursing Exam and RationaleTomzki Cornelio100% (5)
- Hypertensive CrisisDocument7 pagesHypertensive Crisisalul847474No ratings yet
- LactuloseDocument2 pagesLactuloseGrace Iloreta RN82% (11)
- Carousel Restricted AccessDocument12 pagesCarousel Restricted AccessJess BaerNo ratings yet
- Cooper 2020Document18 pagesCooper 2020Lohann MedeirosNo ratings yet
- Success in Treatment For Opioid UseDocument7 pagesSuccess in Treatment For Opioid Usemuhammad.marsoze.hattaNo ratings yet
- Psychotropic Medication For Children and Adolescents With EDocument10 pagesPsychotropic Medication For Children and Adolescents With EloloasbNo ratings yet
- Is There Long-Term Bene Fit From Stimulant Treatment For ADHD?Document2 pagesIs There Long-Term Bene Fit From Stimulant Treatment For ADHD?Maria Soledad HernandezNo ratings yet
- Buprenorphine Treatment For Young AdultsDocument2 pagesBuprenorphine Treatment For Young AdultsGNo ratings yet
- DownloadDocument6 pagesDownloadMr AggarwalNo ratings yet
- PDF TestDocument15 pagesPDF TestJess BaerNo ratings yet
- Mother NejmDocument12 pagesMother NejmIzara Maité Mondragón MorenoNo ratings yet
- Association BetweenAttention-Deficit/Hyperactivity Disorder andBenzodiazepinesandZ-HypnoticsinPregnancy-QuestionsRemainDocument3 pagesAssociation BetweenAttention-Deficit/Hyperactivity Disorder andBenzodiazepinesandZ-HypnoticsinPregnancy-QuestionsRemain321154501No ratings yet
- Cognitive Behavioral Therapy Program For Cannabis Use Cessation in First-Episode Psychosis Patients: A 1-Year Randomized Controlled TrialDocument19 pagesCognitive Behavioral Therapy Program For Cannabis Use Cessation in First-Episode Psychosis Patients: A 1-Year Randomized Controlled TrialAlfredo MorenoNo ratings yet
- Timlim 2014Document14 pagesTimlim 2014Romina Fernanda Inostroza NaranjoNo ratings yet
- Wakeman 2020 Oi 190774Document12 pagesWakeman 2020 Oi 190774Yed HeeNo ratings yet
- Deprescribing Benzodiazepines and Z-Drugs in Community-Dwelling Adults: A Scoping ReviewDocument12 pagesDeprescribing Benzodiazepines and Z-Drugs in Community-Dwelling Adults: A Scoping ReviewReyveen PrasadNo ratings yet
- Office-Based Treatment of Opiate Addiction With A Sublingual-Tablet Formulation of Buprenorphine and NaloxoneDocument10 pagesOffice-Based Treatment of Opiate Addiction With A Sublingual-Tablet Formulation of Buprenorphine and NaloxoneTomi AtmadirjaNo ratings yet
- Clinical StudyDocument5 pagesClinical StudyBruno Pedraz PetrozziNo ratings yet
- Mat LagieDocument7 pagesMat Lagieltnyf7eaNo ratings yet
- JMCP 2023 29 1 58Document11 pagesJMCP 2023 29 1 58Javier Martin Bartolo GarciaNo ratings yet
- Treatment of Methadone-Maintained Patients With Adult ADHD: Double-Blind Comparison of Methylphenidate, Bupropion and PlaceboDocument12 pagesTreatment of Methadone-Maintained Patients With Adult ADHD: Double-Blind Comparison of Methylphenidate, Bupropion and Placeboangelson_suryadi100% (1)
- Correspondence: Prof. Saeed Farooq, MCPS, FCPS, Professor Department ofDocument2 pagesCorrespondence: Prof. Saeed Farooq, MCPS, FCPS, Professor Department ofKaram Ali ShahNo ratings yet
- Circulatorio y Óseo MicrobiologiaDocument13 pagesCirculatorio y Óseo MicrobiologiaLinaMejiaNo ratings yet
- Dela Cruz, Christine v. - EbnDocument5 pagesDela Cruz, Christine v. - EbnChristine Dela CruzNo ratings yet
- Recaida de Primer Episodio Psicótico Con Adherencia Al TratamientoDocument7 pagesRecaida de Primer Episodio Psicótico Con Adherencia Al TratamientopsychforallNo ratings yet
- Hyperprolactinemia and Galactorrhea Induced by Serotonin and Norepinephrine Reuptake Inhibiting AntidepressantsDocument10 pagesHyperprolactinemia and Galactorrhea Induced by Serotonin and Norepinephrine Reuptake Inhibiting AntidepressantsSteven KatuukNo ratings yet
- Inggris IntervensionDocument8 pagesInggris IntervensionNasrudin JamilNo ratings yet
- Antipsychotic Use in Children and Adolescents A.13Document7 pagesAntipsychotic Use in Children and Adolescents A.13jacopo pruccoliNo ratings yet
- 3 Delinquent Mta Molinaetal07Document13 pages3 Delinquent Mta Molinaetal07lucasher35No ratings yet
- Pone 0267808Document22 pagesPone 0267808patowilliamsNo ratings yet
- Pharmacy: Ingestible Sensors and Medication Adherence: Focus On Use in Serious Mental IllnessDocument11 pagesPharmacy: Ingestible Sensors and Medication Adherence: Focus On Use in Serious Mental IllnessArif IrpanNo ratings yet
- Psychopharmacology and Preschoolers A Critical ReviewDocument19 pagesPsychopharmacology and Preschoolers A Critical ReviewOctavio GarciaNo ratings yet
- Research ArticleDocument12 pagesResearch ArticletiarNo ratings yet
- STart StroppDocument1 pageSTart StroppHoang Mai NguyenNo ratings yet
- Are Patients Taking TheirDocument6 pagesAre Patients Taking TheirCarlos De PazNo ratings yet
- Fphar-2021-734045 1..15Document15 pagesFphar-2021-734045 1..15Moch. NabilNo ratings yet
- A Preliminary Trial: Double-Blind Comparison of Nefazodone, Bupropion-SR, and Placebo in The Treatment of Cannabis DependenceDocument12 pagesA Preliminary Trial: Double-Blind Comparison of Nefazodone, Bupropion-SR, and Placebo in The Treatment of Cannabis DependenceJai KunvarNo ratings yet
- Polysubstance Use - Diagnostic Challenges, Patterns of Use and HealthDocument7 pagesPolysubstance Use - Diagnostic Challenges, Patterns of Use and HealthAndres Felipe Silva IbarraNo ratings yet
- Physician Factors Associated With Polypharmacy and Potentially Inappropriate Medication UseDocument9 pagesPhysician Factors Associated With Polypharmacy and Potentially Inappropriate Medication UseratnatriaaNo ratings yet
- Evaluation of Drug Related Problems in Patients With Chronic Disease at Tertiary Care Teaching HospitalDocument12 pagesEvaluation of Drug Related Problems in Patients With Chronic Disease at Tertiary Care Teaching HospitalenesNo ratings yet
- Tratamiento Del TDAH Dual: Una Gota en El Desierto: The Treatment of Dual ADHD: A Drop in The OceanDocument5 pagesTratamiento Del TDAH Dual: Una Gota en El Desierto: The Treatment of Dual ADHD: A Drop in The OceanJoana CalepsoNo ratings yet
- The Epidemiology of Pharmacologically Treated Attention Deficit Hyperactivity Disorder (ADHD) in Children, Adolescents and Adults in UK Primary CareDocument11 pagesThe Epidemiology of Pharmacologically Treated Attention Deficit Hyperactivity Disorder (ADHD) in Children, Adolescents and Adults in UK Primary CarecsilvaNo ratings yet
- Jurnal 4Document14 pagesJurnal 4Khansa najmaNo ratings yet
- Combined - Pharmacotherapies - and - Behaviora PDFDocument15 pagesCombined - Pharmacotherapies - and - Behaviora PDFalexandra mariaNo ratings yet
- Volk Ow 2008Document4 pagesVolk Ow 2008nurfitriaNo ratings yet
- Molina, B. S.,et Al. (2009) - The MTA at 8 Years PDFDocument17 pagesMolina, B. S.,et Al. (2009) - The MTA at 8 Years PDFjuanNo ratings yet
- Faculty of Medicine, Novi Sad, SerbiaDocument5 pagesFaculty of Medicine, Novi Sad, SerbiaAnkete FNo ratings yet
- Academic Pediatrics Volume 12 Issue 2 2012Document7 pagesAcademic Pediatrics Volume 12 Issue 2 2012Paul AsturbiarisNo ratings yet
- Tratamiento en Patología DualDocument7 pagesTratamiento en Patología DualBalmaNo ratings yet
- 9130Document13 pages9130BimaNo ratings yet
- Uso Inapropiado de Fármacos de Prescripción: Dependencia A Benzodiazepinas en Adultos MayoresDocument7 pagesUso Inapropiado de Fármacos de Prescripción: Dependencia A Benzodiazepinas en Adultos MayorespaofrancoNo ratings yet
- Chapter 1 - Pharma DostDocument3 pagesChapter 1 - Pharma DostabinchandrakumarNo ratings yet
- Research Paper On PolypharmacyDocument5 pagesResearch Paper On Polypharmacyefj02jba100% (1)
- Sam ADocument10 pagesSam AAngela Rivas CastilloNo ratings yet
- Adherence of Psychopharmacological Prescriptions To Clinical PDFDocument9 pagesAdherence of Psychopharmacological Prescriptions To Clinical PDFGaby ZavalaNo ratings yet
- Add 12140Document9 pagesAdd 12140imadhassanNo ratings yet
- Cope StudyDocument9 pagesCope StudyCarmen Paz Oyarzun ReyesNo ratings yet
- Jamapediatrics Renny 2021 Oi 210033 1623180608.24244Document10 pagesJamapediatrics Renny 2021 Oi 210033 1623180608.24244seetaNo ratings yet
- Cardiovascular Complications Among Individuals With Amphetamine-Positive Urine Drug Screening Admitted To A Tertiary Care Hospital in RiyadhDocument7 pagesCardiovascular Complications Among Individuals With Amphetamine-Positive Urine Drug Screening Admitted To A Tertiary Care Hospital in Riyadhluthfi syah saqiNo ratings yet
- Acute Myocardial Infarction With Multiple Oronary Thromboses in A Young Addict of Amphetamines and BenzodiazepinesDocument5 pagesAcute Myocardial Infarction With Multiple Oronary Thromboses in A Young Addict of Amphetamines and Benzodiazepinesluthfi syah saqiNo ratings yet
- The Necessity of Restorative Justice On Juvenile Delinquency in Indonesia, Lessons Learned From The Raju and AAL CasesDocument9 pagesThe Necessity of Restorative Justice On Juvenile Delinquency in Indonesia, Lessons Learned From The Raju and AAL Casesluthfi syah saqiNo ratings yet
- 1 s2.0 S1878535216301137 MainDocument9 pages1 s2.0 S1878535216301137 Mainluthfi syah saqiNo ratings yet
- Alem Mehari ReportDocument67 pagesAlem Mehari Reportetayhailu100% (5)
- Van Daele - Recommendations For Policy and Practice of Telepsychotherapy and E-Mental Health in Europe and BeyondDocument36 pagesVan Daele - Recommendations For Policy and Practice of Telepsychotherapy and E-Mental Health in Europe and BeyondMaximiliano AzconaNo ratings yet
- Clinical Applications of Ferric Sulfate in Dentistry: A Narrative ReviewDocument4 pagesClinical Applications of Ferric Sulfate in Dentistry: A Narrative ReviewAnonymous HfJEe9qrNo ratings yet
- Metacognitive Interpersonal Therapy in A Case of Obsessive-Compulsive and Avoidant Personality DisordersDocument14 pagesMetacognitive Interpersonal Therapy in A Case of Obsessive-Compulsive and Avoidant Personality DisordersAlejandro LeónNo ratings yet
- Early Life and EducationDocument3 pagesEarly Life and EducationNikullynNo ratings yet
- Zarjis Composite Knit Ind LTD PDFDocument3 pagesZarjis Composite Knit Ind LTD PDFMd. Suruz ZamanNo ratings yet
- Top Categoriestop Audiobook CategoriesDocument167 pagesTop Categoriestop Audiobook CategoriesmadhusudaniyaarNo ratings yet
- Connective Tissue DisorderDocument51 pagesConnective Tissue DisorderKathleenZunigaNo ratings yet
- Effectiveness of Physiotherapy Exercise After Knee Arthroplasty For OsteoarthritisDocument2 pagesEffectiveness of Physiotherapy Exercise After Knee Arthroplasty For OsteoarthritisGopi KrishnanNo ratings yet
- Government of Canada Report On The Pricing of Revlimid (Lenalidomide) in CanadaDocument2 pagesGovernment of Canada Report On The Pricing of Revlimid (Lenalidomide) in CanadajennabushNo ratings yet
- Experiment 6.2Document3 pagesExperiment 6.2cindy_lee_11No ratings yet
- The Bio-Col TechniqueDocument9 pagesThe Bio-Col TechniquewnelsenNo ratings yet
- FUNDA0319Document11 pagesFUNDA0319Clarissa Guifaya50% (2)
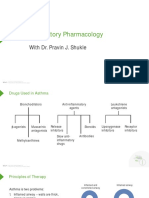
- Respiratory Pharmacology: With Dr. Pravin J. ShukleDocument28 pagesRespiratory Pharmacology: With Dr. Pravin J. ShukleKaish DahiyaNo ratings yet
- C V Dr. Cesar Guerrero 2014Document38 pagesC V Dr. Cesar Guerrero 2014ucbrotherNo ratings yet
- SLEDDDocument38 pagesSLEDDrini purwantiNo ratings yet
- (CPG) Philippine Practice Guidelines For The Diagnosis, Staging, and Management of Lung CarcinomaDocument54 pages(CPG) Philippine Practice Guidelines For The Diagnosis, Staging, and Management of Lung CarcinomaJobelleNo ratings yet
- PARKINSONISMDocument5 pagesPARKINSONISMPrashanth RajuNo ratings yet