You might also like
- Jared Griffin Care PlanDocument14 pagesJared Griffin Care PlanKarina Rodriguez100% (4)
- EL-Calculating Endotoxin LimitsDocument5 pagesEL-Calculating Endotoxin Limitsjaks2771% (7)
- PATHOPHYSIOLOGY SCHEMATIC DIAGRAM OF PREECLAMPSIADocument4 pagesPATHOPHYSIOLOGY SCHEMATIC DIAGRAM OF PREECLAMPSIACarrie A100% (2)
- Patho A 1. 5 Hemodynamic Disorders (Bongat, 2015)Document12 pagesPatho A 1. 5 Hemodynamic Disorders (Bongat, 2015)Grant GarcesNo ratings yet
- Problem With The PassageDocument3 pagesProblem With The PassageLuiciaNo ratings yet
- Neofax 2020 (001-430)Document430 pagesNeofax 2020 (001-430)Paola Yelitza Rodriguez TorreNo ratings yet
- Guaifenesin Drug CardDocument1 pageGuaifenesin Drug CardJessie JenningsNo ratings yet
- Pre Eclampsia LermaDocument9 pagesPre Eclampsia LermaJINYVEV APARICINo ratings yet
- NCM 109 Rle - MidtermsDocument12 pagesNCM 109 Rle - Midtermsmegprado77No ratings yet
- PathophysioDocument2 pagesPathophysioaasimon2466cabNo ratings yet
- Cream Modern Simple & Lined Thesis Defense PresentationDocument43 pagesCream Modern Simple & Lined Thesis Defense PresentationCayla DeniceNo ratings yet
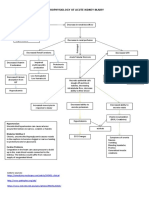
- Pathophysiology of Acute Kidney InjuryDocument4 pagesPathophysiology of Acute Kidney InjuryJane Arian Berzabal0% (1)
- Module 5 HYPERTENSION - OUTPUT - VILLANUEVADocument12 pagesModule 5 HYPERTENSION - OUTPUT - VILLANUEVAClarice VillanuevaNo ratings yet
- Case Report on Severe PreeclampsiaDocument98 pagesCase Report on Severe Preeclampsianovika100% (1)
- CH 2 Case PresDocument10 pagesCH 2 Case Prestintin srgpnNo ratings yet
- Hypertension in Pregnancy: A Guide to Diagnosis and ManagementDocument85 pagesHypertension in Pregnancy: A Guide to Diagnosis and ManagementLammaa T DHNo ratings yet
- Pre Eclampsia: An OverviewDocument13 pagesPre Eclampsia: An OverviewJay PaulNo ratings yet
- Preeclampsia and EclampsiaDocument23 pagesPreeclampsia and Eclampsiaapi-3705046100% (6)
- 6 Med Ward (WK - 1) PathophysiologyDocument3 pages6 Med Ward (WK - 1) PathophysiologyZaijean Kate Dianne LigutomNo ratings yet
- Chronic Kidney Disease Stages, Causes, SymptomsDocument5 pagesChronic Kidney Disease Stages, Causes, Symptomsjazzy penzNo ratings yet
- Difference CH and PEDocument39 pagesDifference CH and PEPAOGI UNANDNo ratings yet
- Bab Ii Tinjauan PustakaDocument20 pagesBab Ii Tinjauan PustakairwanNo ratings yet
- Ascites: Diagnosis and Management: Clinical MedicineDocument9 pagesAscites: Diagnosis and Management: Clinical MedicineRizqi Amalia100% (1)
- Pre Eklamsia Dan EklamsiaDocument6 pagesPre Eklamsia Dan EklamsiaVammy Beverly ValentineNo ratings yet
- Steroid Responsif Nephrotic Syndrome (SRNS)Document16 pagesSteroid Responsif Nephrotic Syndrome (SRNS)Ikrar AbdillahNo ratings yet
- Lo OjiDocument7 pagesLo OjiJosephine Grace SuryadiNo ratings yet
- Renal FailureDocument5 pagesRenal FailureAmoroso, Marian Corneth D.No ratings yet
- Presented By: Sonia Dagar: Renal FailureDocument40 pagesPresented By: Sonia Dagar: Renal FailureRavanshi ThakurNo ratings yet
- Renal SystemDocument20 pagesRenal SystemRahul DasNo ratings yet
- Chemistry Presentation (Hypertonic)Document14 pagesChemistry Presentation (Hypertonic)OscarNo ratings yet
- Cirrhosis and Its ComplicationsDocument3 pagesCirrhosis and Its ComplicationsMahaNo ratings yet
- Case Analysis Group 1Document12 pagesCase Analysis Group 1mark_partolanNo ratings yet
- Pathophysio PreeclampsiaDocument2 pagesPathophysio PreeclampsiaMarlowe Czar Catalan SoriñoNo ratings yet
- Complications of CirrhosisDocument2 pagesComplications of CirrhosisDanielle DiorioNo ratings yet
- Pa Tho Physiology Final DMDocument6 pagesPa Tho Physiology Final DMJamil LorcaNo ratings yet
- Pathophysiology EclampsiaDocument5 pagesPathophysiology EclampsiaYael EzraNo ratings yet
- Edema Guide: Causes, Symptoms and Treatment of Fluid RetentionDocument4 pagesEdema Guide: Causes, Symptoms and Treatment of Fluid RetentionWanchung ZienNo ratings yet
- Portal Hypertension and Ascites: Table 1Document7 pagesPortal Hypertension and Ascites: Table 1Hưng Nguyễn KiềuNo ratings yet
- Quiz 2 (Continued)Document10 pagesQuiz 2 (Continued)Teresa DumalagNo ratings yet
- MetabolismDocument39 pagesMetabolismTiffany KnepperNo ratings yet
- Pregnancy Induced HypertensionDocument9 pagesPregnancy Induced HypertensionYalc LapidNo ratings yet
- Hypertension in PregnancyDocument34 pagesHypertension in PregnancyMusekhirNo ratings yet
- +nephrotic SyndromeDocument22 pages+nephrotic SyndromeDr. SAMNo ratings yet
- Pregnancy Induced Hypertension VBRDocument50 pagesPregnancy Induced Hypertension VBRBrylee CudalNo ratings yet
- Preeclampsia: Causes, Symptoms and TreatmentDocument47 pagesPreeclampsia: Causes, Symptoms and TreatmentrranindyaprabasaryNo ratings yet
- Liver Cirrhosis: Vitebsk State Medical University Pathological Physiology DepartmentDocument19 pagesLiver Cirrhosis: Vitebsk State Medical University Pathological Physiology DepartmentSanduni WickramaratneNo ratings yet
- Pathophysiology of Chronic Kidney Disease: Predisposing Factors: Precipitating FactorsDocument1 pagePathophysiology of Chronic Kidney Disease: Predisposing Factors: Precipitating FactorsReina SamsonNo ratings yet
- Pregnancy Hypertension GuideDocument11 pagesPregnancy Hypertension Guideyssa deliNo ratings yet
- Lecture - Acute Renal FailureDocument57 pagesLecture - Acute Renal FailureJames StiltonNo ratings yet
- Pre EclampsiaDocument55 pagesPre EclampsiaDuncan Jackson100% (2)
- Edema Types and CausesDocument31 pagesEdema Types and CausesLIEBERKHUNNo ratings yet
- Ascites: Fredric D. GordonDocument15 pagesAscites: Fredric D. GordonNancy Mac Lean BalboaNo ratings yet
- Hypertension in Pregnancy: Margaret S. Hamilton, DNS, RNDocument33 pagesHypertension in Pregnancy: Margaret S. Hamilton, DNS, RNHaji RajiNo ratings yet
- Reviewer MaternalDocument10 pagesReviewer MaternalJohana Pinagayao AngkadNo ratings yet
- Pathohysiology of Ascites: Waleed Al-HamoudiDocument36 pagesPathohysiology of Ascites: Waleed Al-Hamoudiarina31No ratings yet
- Presented By: Medicine Unit 1Document95 pagesPresented By: Medicine Unit 1Abdullah Muceddidi100% (1)
- Doctor's Visit Takes A Funny TurnDocument106 pagesDoctor's Visit Takes A Funny TurnaahadNo ratings yet
- Lecture 6-ShockDocument5 pagesLecture 6-ShockMadiha MadiNo ratings yet
- Hepatorenal SyndromeDocument10 pagesHepatorenal SyndromeAmaiiranii GarciiaNo ratings yet
- Portal Hypertension: Pathophysiology, Diagnosis and ManagementDocument11 pagesPortal Hypertension: Pathophysiology, Diagnosis and ManagementXol-TikaNo ratings yet
- Acute Kidney InjuryDocument23 pagesAcute Kidney InjuryBaraka SayoreNo ratings yet
- (Study Group) Diabetic Nephropathy, Hypertensive NephropathyDocument7 pages(Study Group) Diabetic Nephropathy, Hypertensive NephropathyZarif IzzuddinNo ratings yet
- Approach To Patient With Diseases of The Kidney and Urinary Tract FINALDocument9 pagesApproach To Patient With Diseases of The Kidney and Urinary Tract FINALgelskNo ratings yet
- Fast Facts: Deficiencia de piruvato quinasa para pacientes y familiares: Una enfermedad genética rara que afecta a los glóbulos rojos Información + Asumir el control = El mejor resultadoFrom EverandFast Facts: Deficiencia de piruvato quinasa para pacientes y familiares: Una enfermedad genética rara que afecta a los glóbulos rojos Información + Asumir el control = El mejor resultadoNo ratings yet
- Fast Facts: Pyruvatkinase-Mangel für Patienten und Angehörige: Eine seltene genetische Erkrankung der roten Blutkörperchen Informationen + Mitreden-Können = Bestmöglicher VerlaufFrom EverandFast Facts: Pyruvatkinase-Mangel für Patienten und Angehörige: Eine seltene genetische Erkrankung der roten Blutkörperchen Informationen + Mitreden-Können = Bestmöglicher VerlaufNo ratings yet
- Nutrition Essentials for Growing ChildrenDocument2 pagesNutrition Essentials for Growing ChildrenLuiciaNo ratings yet
- The Endocrine System: A Network of Hormone-Secreting GlandsDocument6 pagesThe Endocrine System: A Network of Hormone-Secreting GlandsLuiciaNo ratings yet
- Addison ReviewerDocument3 pagesAddison ReviewerLuiciaNo ratings yet
- Musculoskeletal ReviewerDocument6 pagesMusculoskeletal ReviewerLuiciaNo ratings yet
- Cushing ReviewerDocument3 pagesCushing ReviewerLuiciaNo ratings yet
- Multiple SclerosisDocument2 pagesMultiple SclerosisLuiciaNo ratings yet
- The Intellectual RevolutionDocument4 pagesThe Intellectual RevolutionLuiciaNo ratings yet
- AlzheimerDocument5 pagesAlzheimerLuiciaNo ratings yet
- DI Diagnosis and TreatmentDocument2 pagesDI Diagnosis and TreatmentLuiciaNo ratings yet
- Microscopy Techniques and Staining MethodsDocument2 pagesMicroscopy Techniques and Staining MethodsLuiciaNo ratings yet
- ParkinsonDocument5 pagesParkinsonLuiciaNo ratings yet
- Amyotrophic Lateral SclerosisDocument5 pagesAmyotrophic Lateral SclerosisLuiciaNo ratings yet
- Drugs RespiratoryDocument15 pagesDrugs RespiratoryLuiciaNo ratings yet
- Cradle of CivilizationDocument3 pagesCradle of CivilizationLuiciaNo ratings yet
- Expanded Program On Immunization (EPI) 7 Vaccine-Preventable Diseases VaccinesDocument7 pagesExpanded Program On Immunization (EPI) 7 Vaccine-Preventable Diseases VaccinesLuiciaNo ratings yet
- Process Quality - III - 2005 - 2010 - Outcome or Impact QualityDocument2 pagesProcess Quality - III - 2005 - 2010 - Outcome or Impact QualityLuiciaNo ratings yet
- Without This, We Would Be Blinded and Bound As We Face More Serious Threats To Health GloballyDocument2 pagesWithout This, We Would Be Blinded and Bound As We Face More Serious Threats To Health GloballyLuiciaNo ratings yet
- Addison ReviewerDocument3 pagesAddison ReviewerLuiciaNo ratings yet
- The Endocrine System: Hormones and Glands that Regulate the BodyDocument6 pagesThe Endocrine System: Hormones and Glands that Regulate the BodyLuiciaNo ratings yet
- Cushing ReviewerDocument3 pagesCushing ReviewerLuiciaNo ratings yet
- Antibiotics That Selectively Inhibit The Growth or Kill Microorganisms With Minimal Effects On ManDocument7 pagesAntibiotics That Selectively Inhibit The Growth or Kill Microorganisms With Minimal Effects On ManLuiciaNo ratings yet
- Anomalies of The Placenta and CordDocument2 pagesAnomalies of The Placenta and CordLuiciaNo ratings yet
- Hyperthyroidism ReviewerDocument5 pagesHyperthyroidism ReviewerLuiciaNo ratings yet
- Respiratory Disorders and PregnancyDocument3 pagesRespiratory Disorders and PregnancyLuiciaNo ratings yet
- Complications With The PowerDocument9 pagesComplications With The PowerLuiciaNo ratings yet
- Gastrointestinal Disorders and PregnancyDocument2 pagesGastrointestinal Disorders and PregnancyLuiciaNo ratings yet
- MastitisDocument2 pagesMastitisLuiciaNo ratings yet
- Renal and Urinary Disorders and PregnancyDocument2 pagesRenal and Urinary Disorders and PregnancyLuiciaNo ratings yet
- Nasal Steroid Proven Effective Rhinitis TreatmentDocument80 pagesNasal Steroid Proven Effective Rhinitis TreatmentYuliastuti RahayuNo ratings yet
- Scientific Evidence For Bromelain, Trypsin and RutinDocument9 pagesScientific Evidence For Bromelain, Trypsin and Rutinganesh.divekar7256No ratings yet
- College of Nursing: Pharmacological ManagementDocument3 pagesCollege of Nursing: Pharmacological ManagementAnika PleñosNo ratings yet
- Nice 2016Document85 pagesNice 2016Diana ToroNo ratings yet
- Chloral Hydrate (Drug Study)Document3 pagesChloral Hydrate (Drug Study)Franz.thenurse6888No ratings yet
- Answer Sheet Interpreting Prescription OrdersDocument3 pagesAnswer Sheet Interpreting Prescription OrdersAUDREY ARQUERONo ratings yet
- Current Concepts About Motr Neuron DiseaseDocument68 pagesCurrent Concepts About Motr Neuron DiseaseMuhammad MuaazNo ratings yet
- Impact of Postoperative Dexmedetomidine Infusion On Incidence of Delirium in Elderly Patients Undergoing Major Elective Noncardiac Surgery2019Document12 pagesImpact of Postoperative Dexmedetomidine Infusion On Incidence of Delirium in Elderly Patients Undergoing Major Elective Noncardiac Surgery2019Cláudia Regina FernandesNo ratings yet
- Midwest HIDTA Kansas 2023 Overdose ReportDocument9 pagesMidwest HIDTA Kansas 2023 Overdose ReportMatthew SelfNo ratings yet
- Data Bu ShellaDocument114 pagesData Bu Shellaruri nur indahNo ratings yet
- Anatomy & Physiology Unit 1Document29 pagesAnatomy & Physiology Unit 1Priyanjali SainiNo ratings yet
- Liposome-as Drug Carriers: A Review of Their Structure and ApplicationsDocument8 pagesLiposome-as Drug Carriers: A Review of Their Structure and Applicationsgalangpramadhan pcNo ratings yet
- Fourteen Illustrated Drug Information Booklets: The Truth About Drugs Is A SeriesDocument3 pagesFourteen Illustrated Drug Information Booklets: The Truth About Drugs Is A Seriesjoshuaangue60% (5)
- The stellate ganglion is located anterior to the transverse processes of C7 and T1 vertebraeDocument287 pagesThe stellate ganglion is located anterior to the transverse processes of C7 and T1 vertebraeSAJID ALINo ratings yet
- The Examiner of Alternative MedicineDocument4 pagesThe Examiner of Alternative MedicineLee Ming HinNo ratings yet
- Importance of Dravyaguna Vigayan in AyurvedaDocument17 pagesImportance of Dravyaguna Vigayan in AyurvedaPramba Kumar Ahuja100% (3)
- DaturaDocument2 pagesDaturaJasmine StuczynskiNo ratings yet
- Dr. Reddy's API Product List PDFDocument9 pagesDr. Reddy's API Product List PDFROUNAK PALNo ratings yet
- Status Epilepticus and ICPDocument9 pagesStatus Epilepticus and ICPjoomds51No ratings yet
- Flange Tables PDFDocument18 pagesFlange Tables PDFDylan RamasamyNo ratings yet
- Dolsten (Mefenamic Acid) : Relief of Pain Including Muscular, Rheumatic, TraumaticDocument2 pagesDolsten (Mefenamic Acid) : Relief of Pain Including Muscular, Rheumatic, TraumaticDavid VillanuevaNo ratings yet
- Centella Asiatica (Gotu Kola) As A Neuroprotectant and Its Potential Role in Healthy AgeingDocument10 pagesCentella Asiatica (Gotu Kola) As A Neuroprotectant and Its Potential Role in Healthy AgeingTrần Thuý QuỳnhNo ratings yet
- Management of Local Anesthetic Complications: Ross Camiel, Samuel Roh, and Christy LottingerDocument10 pagesManagement of Local Anesthetic Complications: Ross Camiel, Samuel Roh, and Christy LottingerErryskaNo ratings yet
- Nursing care for inflammatory and immunologic disordersDocument8 pagesNursing care for inflammatory and immunologic disordersSitty Aizah MangotaraNo ratings yet
- King's Research Portal: Peer Reviewed VersionDocument48 pagesKing's Research Portal: Peer Reviewed VersionADNo ratings yet
- Drug Therapy in Nursing 3e Test BankDocument4 pagesDrug Therapy in Nursing 3e Test BankcharmainebellamykixNo ratings yet