Professional Documents
Culture Documents
CDEM 19july Web
Uploaded by
Ricardo Jonathan Ayala GarciaOriginal Title
Copyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
CDEM 19july Web
Uploaded by
Ricardo Jonathan Ayala GarciaCopyright:
Available Formats
Volume 33 Number 7 July 2019
Observation Deck
Observation units are increasingly used to manage
acute presentations when safe discharge is in doubt
and the need for inpatient admission is unclear. While
there are a number of existing models for this approach
to care, emergency departments have become keenly
invested in the surge of new, protocolized observation
units. As such, clinicians must be prepared to maximize
this safety net by selecting appropriate patients for
monitoring and using interdisciplinary protocols to
manage their conditions.
Warning Shots
The relative rarity of measles, mumps, pertussis,
varicella, and tetanus can make it particularly difficult
to recognize and appropriately treat these potentially
deadly illnesses. While herd immunity provides
significant protection against most of these diseases,
a recent decrease in vaccination rates and a rise in
international travel have created the opportunity
for new outbreaks. As such, it is vital for front-line
clinicians to renew their understanding of vaccine-
preventable illnesses and be prepared to manage them.
THE OFFICIAL CME PUBLICATION OF THE AMERICAN COLLEGE OF EMERGENCY PHYSICIANS
IN THIS ISSUE
Lesson 13 n Vaccine-Preventable Illnesses . . . . . . . . . . . . . . . . . . . . . . . . 3
Critical ECG . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 13 Critical Decisions in Emergency Medicine is the official
CME publication of the American College of Emergency
Critical Image . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 14
Physicians. Additional volumes are available.
Critical Cases in Orthopedics and Trauma . . . . . . . . . . . . . . . . . . . . . . . . . 16
EDITOR-IN-CHIEF
Critical Procedure . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 18 Michael S. Beeson, MD, MBA, FACEP
Lesson 14 n Emergency Department Observation Care . . . . . . . . . . . 19 Northeastern Ohio Universities,
Rootstown, OH
LLSA Literature Review . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 25
SECTION EDITORS
CME Questions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 26
Joshua S. Broder, MD, FACEP
Drug Box/Tox Box . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 28 Duke University, Durham, NC
Andrew J. Eyre, MD, MHPEd
Contributor Disclosures. In accordance with the ACCME Standards for Commercial Support Brigham & Women’s Hospital/
and policy of the American College of Emergency Physicians, all individuals with control Harvard Medical School, Boston, MA
over CME content (including but not limited to staff, planners, reviewers, and authors) must John Kiel, DO, MPH
disclose whether or not they have any relevant financial relationship(s) to learners prior to the University of Florida College of Medicine, Jacksonville, FL
start of the activity. These individuals have indicated that they have a relationship which, in
the context of their involvement in the CME activity, could be perceived by some as a real or Frank LoVecchio, DO, MPH, FACEP
apparent conflict of interest (eg, ownership of stock, grants, honoraria, or consulting fees), Maricopa Medical Center/Banner Phoenix Poison
but these individuals do not consider that it will influence the CME activity. Joshua S. Broder, and Drug Information Center, Phoenix, AZ
MD, FACEP: He owns OmniSono Inc, an ultrasound technology company, and his wife is Amal Mattu, MD, FACEP
employed by GlaxoSmithKline as a research organic chemist. Christopher C. Raio, MD, MBA, University of Maryland, Baltimore, MD
FACEP: He is a consultant for Butterfly Network/Hyperfine Research, a medical product
development company. All remaining individuals with control over CME content have no Lynn P. Roppolo, MD, FACEP
significant financial interests or relationships to disclose. UT Southwestern Medical Center,
Dallas, TX
This educational activity consists of two lessons, a post-test, and evaluation questions;
as designed, the activity should take approximately 5 hours to complete. The participant Christian A. Tomaszewski, MD, MS, MBA, FACEP
should, in order, review the learning objectives, read the lessons as published in the print University of California Health Sciences,
or online version, and complete the online post-test (a minimum score of 75% is required) San Diego, CA
and evaluation questions. Release date July 1, 2019. Expiration June 30, 2022. Steven J. Warrington, MD, MEd
Accreditation Statement. The American College of Emergency Physicians is accredited by Orange Park Medical Center, Orange Park, FL
the Accreditation Council for Continuing Medical Education to provide continuing medical
education for physicians.
ASSOCIATE EDITORS
Wan-Tsu W. Chang, MD
The American College of Emergency Physicians designates this enduring material for a
University of Maryland, Baltimore, MD
maximum of 5 AMA PRA Category 1 Credits™. Physicians should claim only the credit
commensurate with the extent of their participation in the activity. Walter L. Green, MD, FACEP
UT Southwestern Medical Center,
Each issue of Critical Decisions in Emergency Medicine is approved by ACEP for 5 ACEP
Dallas, TX
Category I credits. Approved by the AOA for 5 Category 2-B credits.
John C. Greenwood, MD
Commercial Support. There was no commercial support for this CME activity.
University of Pennsylvania, Philadelphia, PA
Target Audience. This educational activity has been developed for emergency physicians.
Danya Khoujah, MBBS
University of Maryland, Baltimore, MD
Critical Decisions in Emergency Medicine is a trademark owned and published monthly by the American
Sharon E. Mace, MD, FACEP
College of Emergency Physicians, PO Box 619911, Dallas, TX 75261-9911. Send address changes and
comments to Critical Decisions in Emergency Medicine, PO Box 619911, Dallas, TX 75261-9911, or to
Cleveland Clinic Lerner College of Medicine/
cdem@acep.org; call toll-free 800-798-1822, or 972-550-0911. Case Western Reserve University, Cleveland, OH
Nathaniel Mann, MD
Copyright 2019 © by the American College of Emergency Physicians. All rights reserved. No part of this
Greenville Health System, Greenville, SC
publication may be reproduced, stored, or transmitted in any form or by any means, electronic or mechanical,
including storage and retrieval systems, without permission in writing from the Publisher. Printed in the USA. Jennifer L. Martindale, MD, MSc
Mount Sinai St. Luke’s/Mount Sinai West,
The American College of Emergency Physicians (ACEP) makes every effort to ensure that contributors to its
publications are knowledgeable subject matter experts. Readers are nevertheless advised that the statements
New York, NY
and opinions expressed in this publication are provided as the contributors’ recommendations at the time David J. Pillow, Jr., MD, FACEP
of publication and should not be construed as official College policy. ACEP recognizes the complexity of UT Southwestern Medical Center, Dallas, TX
emergency medicine and makes no representation that this publication serves as an authoritative resource
for the prevention, diagnosis, treatment, or intervention for any medical condition, nor should it be the basis George Sternbach, MD, FACEP
for the definition of or standard of care that should be practiced by all health care providers at any particular Stanford University Medical Center, Stanford, CA
time or place. Drugs are generally referred to by generic names. In some instances, brand names are added
Joseph F. Waeckerle, MD, FACEP
for easier recognition. Device manufacturer information is provided according to style conventions of the
American Medical Association. ACEP received no commercial support for this publication.
University of Missouri-Kansas City School of Medicine,
Kansas City, MO
To the fullest extent permitted by law, and without
limitation, ACEP expressly disclaims all liability for EDITORIAL STAFF
errors or omissions contained within this publication,
Rachel Donihoo, Managing Editor
and for damages of any kind or nature, arising out of
use, reference to, reliance on, or performance of such
rdonihoo@acep.org
information. Suzannah Alexander, Publishing Assistant
ISSN2325-0186(Print) ISSN2325-8365(Online)
Warning Shots
Vaccine-Preventable
Illnesses
LESSON 13
By Prince Harrison, MBBS; and Timothy Ruttan, MD
Dr. Harrison is an assistant professor in the Department of Pediatrics in the Division
of Emergency Medicine at the University of Nebraska Medical Center in Omaha.
Dr. Ruttan is a clinical assistant professor in the Department of Pediatrics at the
University of Texas at Austin Dell Medical School.
Reviewed by Walter L. Green, MD, FACEP
OBJECTIVES
On completion of this lesson, you should be able to: CRITICAL DECISIONS
1. Recognize the signs and symptoms of measles,
n What clinical features differentiate the various
mumps, pertussis, varicella, and tetanus.
vaccine-preventable illnesses?
2. Determine which diagnostic tests are warranted.
3. Explain when to administer vaccines or n Which diagnostic tests can help identify each illness?
immunoglobulins. n How should each illness be treated, and which
4. Formulate appropriate disposition plans based on patients are at high risk for complications?
host characteristics.
n What measures can help prevent patients and
5. Summarize when to report illnesses and when to treat
susceptible contacts from becoming ill?
potential contacts of the source patient.
n What factors should be considered before
FROM THE EM MODEL discharging a patient?
10.0 Systemic Infectious Disorders
When immunization programs in the United States were introduced, the incidence of measles, mumps,
pertussis, varicella, and tetanus decreased dramatically. Many clinicians now complete their entire training without
seeing an actual case. Unfortunately, this relative rarity can make it particularly difficult to recognize these potentially
deadly pathologies and mitigate their threat to public health. While herd immunity provides significant protection, a
recent decrease in vaccination rates and a rise in international travel have created the opportunity for new outbreaks.1
As such, it is vital for front-line clinicians to renew their understanding of vaccine-preventable illnesses and be
prepared to address them appropriately.
July 2019 n Volume 33 Number 7 3
CASE PRESENTATIONS
■ CASE ONE whole body but is most promi ■ CASE THREE
nent on the face, neck, and
A 10-month-old girl presents A 5-week-old, full-term infant with no
behind the ears.
with a rash that developed over the significant medical history presents with
last 2 days. Her mother explains ■ CASE TWO a cough that her parents say began 5 days
that it started on the child’s face, A 14-year-old girl presents ago. Her father reports that she seems to
spread to her chest on the second with right-sided facial swelling choke when coughing, turns red in the face,
day, and then spread to her arms for 1 day and a subjective, tactile and has post-tussive emesis. There is no
and legs. fever with fatigue that began reported history of fever, apnea, or cyanosis.
On arrival, the patient has 2 days ago. She has no history She is feeding well and is producing wet
a rectal temperature of 38.5°C of dental problems, and her diapers. The infant appears nontoxic,
(101.3°F). Her other vital signs are immunizations are up to date. and her lungs are clear to auscultation.
normal, and she is in no distress. The physician notes tender During the clinical examination, she starts
She has erythema and chemosis swelling over the right side of her coughing intensively, and cyanosis of the
of the conjunctiva, a cough, and a face, inferior and anterior to the face is witnessed. The episode resolves, and
maculopapular rash that covers her earlobe; her dentition is intact. she returns to her baseline.
CRITICAL DECISION the rash appears, the other symptoms hepatitis, myocarditis, and encephalitis.
begin to subside. The rash, which Pneumonia, which can be precipitated
What clinical features
typically resolves over the next 5 to 10 by the measles virus itself or arise from
differentiate the various vaccine-
days, may desquamate about 1 week a bacterial superinfection, presents in a
preventable illnesses? later. In vaccinated patients, the rash comparable manner to pneumonia in a
and other symptoms can be mild or similarly aged patient.
Measles
absent.3 Vaccinated individuals are also Although less routine complications
Once infected, the incubation
less likely to transmit the illness than can be more challenging to detect,
period for measles is approximately
unvaccinated patients infected with a they are important to recognize.
8 to 12 days. The initial phase of the
classic course of measles.4 Measles-related encephalitis is an
illness is characterized by a cough,
Any patient suspected of having immunologically mediated process that
coryza, conjunctivitis, and an increasing
measles must be evaluated for signs of typically begins during the rash phase of
fever. This period is followed by the
development of Koplik spots (Figure 1), complications, including otitis media, the illness. Patients present with seizures,
a pathognomonic feature that is found pneumonia, dehydration from diarrhea, lethargy, and altered mental status, with
in 60% to 70% of cases.2 These discrete,
red lesions, which typically have a bluish FIGURE 1. Koplik Spots
white center, commonly erupt on the
buccal mucosa opposite the premolars;
however, they can also involve the lips,
gingivae, hard palate, conjunctivas, and
vaginal mucosa. While Koplik spots are
pathognomonic, they are not present in
every case; the absence of this finding
should not be used to rule out measles
when a high clinical suspicion exists.
Generalized lymphadenopathy can also
develop.
An erythematous, maculopapular
rash appears 1 to 4 days later, starting
on the forehead, traveling along the
hairline to behind the ears and neck,
and then spreading down to the trunk
and extremities (Figure 2). The rash also
involves the palms of the hands and soles
of the feet in up to half of patients. Once
4 Critical Decisions in Emergency Medicine
an incidence of 1 per 1,000 measles
cases.5 When managing any patient with FIGURE 2. Measles Rash
a similar set of presenting symptoms, it
is important to remember that measles
encephalitis is a diagnosis of exclusion
that can be made only after other
etiologies, such as bacterial meningitis,
have been ruled out.
A less common and more chronic
complication of measles is subacute
sclerosing panencephalitis (SSPE), which
presents 7 to 10 years after the initial
measles illness.5 SSPE, which starts
insidiously with a progressive decline
in behavioral and intellectual abilities,
can lead to ataxia and seizures. The
prognosis for SSPE is poor, eventually
causing death.5
Mumps
After an incubation period of 15 to
24 days, mumps begins with prodromal
symptoms of fever, headache, and body FIGURE 3. Parotid Swelling in a Patient With Mumps
aches that last 1 to 2 days.6 Because
the initial phase is nonspecific, the
disease can be easily confused with
other viral illnesses. Unilateral parotid
swelling with tenderness often occurs,
becoming bilateral in 90% of patients
with parotitis (Figure 3).7 Ear pain can
also accompany parotid swelling. As
with parotitis caused by more common
etiologies, eating sour or acidic foods
can inflame the parotid gland and
worsen pain.
The opening to the Stensen duct can
also become red and edematous, and
parotid swelling can become so severe
that it obscures the angle of the jaw;
the earlobe can become displaced up
and out. Submandibular and sublingual
salivary gland swelling also occurs in
10% of patients.7 Fever is typically
moderate and lasts for up to 7 days. A disease.8 Although deafness — both Impaired fertility affects as many
nonspecific, maculopapular rash may transient and permanent — is a known as 13% of these patients, and up to
also develop on the patient’s trunk. complication of mumps, it is very rare in 50% develop an atrophied testicle.10
As when assessing other vaccine- the post-vaccine era (<1%).9 Abdominal pain in female patients,
preventable illnesses, emergency One of the more common which can be related to oophoritis, may
physicians should evaluate for complications, particularly in mimic appendicitis. Other less common
complications, including meningitis and adolescents and adults, is mumps complications include pancreatitis,
encephalitis, which present with typical orchitis, which is present in up to 40% nephritis, myocarditis, thyroiditis,
symptoms of fever, headache, vomiting, of patients. Most of these cases include mastitis, and arthritis.11
neck stiffness, or seizures. Up to 10% unilateral testicular involvement,
of patients with mumps develop aseptic although up to 30% are marked by Pertussis
meningitis, which is typically benign; bilateral symptoms. In addition to acute Symptoms of pertussis can vary
however, a small portion of these cases pain, mumps orchitis is a significant widely based on the patient’s age.
progress to more severe neurological cause of long-term fertility problems. The classically described illness is
July 2019 n Volume 33 Number 7 5
characterized by three stages. During Adolescents and adults often respiratory illness accompanied by
the initial phase — the catarrhal stage — present without an inspiratory whoop, persistent coughing. Because the cough
patients exhibit nonspecific symptoms as classically described.13 Coughing may not be characterized by the classic
of fever and rhinorrhea, which last 1 episodes can be preceded by a feeling of whoop, these cases can be challenging to
to 2 weeks. The second stage — the strangulation and followed by a feeling diagnose. Pertussis should be considered
paroxysmal phase — begins with the of suffocation. Paroxysms of cough with in any patient with a chronic cough,
onset of a cough. Initially, the cough is post-tussive emesis, in which patients especially in the setting of potentially
dry and intermittent, but it gradually remain relatively asymptomatic between waning vaccine immunity.
becomes paroxysmal. During a violent coughing episodes, can help identify
coughing episode, a well-appearing child potential pertussis cases. Adults may also Varicella
can suddenly become anxious; experience present only with nonspecific respiratory After a 10- to 21-day incubation
a bout of repetitive, staccato coughs; and symptoms that persist for longer than period, adults and adolescents with
then immediately project a loud “whoop,” 3 weeks.14 varicella typically develop malaise and
as air is inhaled against a partially closed As with many other vaccine- fever. This prodrome is usually absent
airway. The paroxysms become more preventable illnesses, common in children, in whom the onset of a
severe and frequent as the paroxysmal complications of pertussis include pruritic rash is the first sign of illness
phase progresses over 2 to 6 weeks. The otitis media and secondary bacterial (Figure 4). The rash, which begins on the
final phase — the convalescent period pneumonia, which can be managed face and scalp and spreads centripetally
— lasts more than 2 weeks. During this according to standards of care. Seizures to the trunk and back, first manifests as
period, the paroxysms become milder and can be a symptom of pertussis-related macules but soon evolves into papules,
less frequent. encephalopathy.15 Moreover, coughing then vesicles, and finally pustules. The
In an infant younger than 3 months, paroxysms can cause subdural pustules have an erythematous base and a
the catarrhal stage can be short, lasting hemorrhage, epistaxis, subconjunctival “dew drops on a rose petal” appearance.
only a few days. A cough may be hemorrhages, pneumothorax, rib
Lesions occur in crops, passing through
inconspicuous during the paroxysmal fractures, hernia, and rectal prolapse.16
the various stages from macules to
stage, which can obscure the diagnosis.12 Despite this, older patients and
pustules to crusting. The pustules are
Infants may exhibit choking, gasping, adults with pertussis typically recover
often in various stages of healing, a
or gagging, with reddening of the face, uneventfully.
process that differs from smallpox, in
flailing of the arms, and minimal startling Particularly when managing older
which all lesions typically progress at
to stimulation. A whoop is less common. patients, it is paramount to address
the same time (Figure 5). Patients are no
Apnea and cyanosis, the most concerning public health concerns and disease
clinical features of pertussis, increase the prevention. Older patients serve as longer infectious once all the lesions have
risk of death in young infants. Moreover, the vector for disease transmission to crusted over (usually in 4-5 days).
the disease can present atypically in unvaccinated or partially vaccinated Previously vaccinated patients may
infants, resembling bronchiolitis or other children, who are at higher risk of severe have a mild, atypical disease course,
forms of respiratory distress. In neonates, and potentially fatal complications. or symptoms that resemble “standard”
the convalescent phase can be prolonged Vaccinated children, adolescents, chicken pox. In the mild form, lesions are
for several months, with the paroxysms and adults with pertussis may be more commonly maculopapular, rather
becoming paradoxically louder. asymptomatic or present with a mild than vesicular. Immunocompromised
patients are at risk for progressive
varicella, a disease characterized by
extensive lesions that continue to
develop over a prolonged period of time,
multiorgan involvement, and potential
sepsis-like symptoms. The risk of
n The initial phase of measles is characterized by a cough, coryza, complications is higher in these patients,
conjunctivitis, and an increasing fever, which may be followed by the who often require hospitalization and
development of Koplik spots. more aggressive treatment.
n Pertussis should be considered in any patient with a chronic cough, Complications from varicella include
especially in the setting of potentially waning vaccine immunity. bacterial superinfection of the skin
n Mumps begins with prodromal symptoms of fever, headache, and body lesions, direct viral pneumonia, secondary
aches that last 1 to 2 days. Because the initial phase is nonspecific, the bacterial pneumonia, acute cerebellar
disease can be easily confused with other viral illnesses. ataxia, encephalitis, and Reye syndrome
n Any patient with a potentially contaminated injury or wound should receive a (in children taking aspirin). Complication
tetanus toxoid to prevent tetanus. rates are higher in children aged less than
1 year and in adolescents and adults.
6 Critical Decisions in Emergency Medicine
FIGURE 4. Varicella Rash FIGURE 5. Smallpox Rash
Tetanus as high as 88% in neonates.17 With CRITICAL DECISION
Tetanus is the result of a toxin intensive care, however, the mortality
Which diagnostic tests can help
produced by Clostridium tetani. In most rate may be as low as 15%.18 Sequelae
in survivors include gait abnormalities, identify each illness?
cases, spores enter the patient through a
traumatic wound, where they germinate muscle rigidity, memory loss, and a
Measles
and ultimately produce an exotoxin that persistent vegetative state.17
In the absence of confirmatory
precipitates the clinical disease. The initial In neonates, tetanus results from
testing, a timely clinical diagnosis is
wound can be relatively inconsequential, poor hygiene of the umbilical stump.
critical when evaluating for measles, an
so the patient may not even recall being Although this complication is extremely
illness with particularly important public
rare in the US, it is relatively common
injured. The incubation period ranges health ramifications. Measles can be
in developing countries because of
from 3 to 21 days after wound exposure. confirmed by serology, when indicated.
poor umbilical cord hygiene and poor
The toxin irreversibly binds to nerves Immunoglobulin M (IgM) becomes
maternal immunization. Symptoms,
and blocks the presynaptic release of elevated 1 to 2 days after the appearance
which usually begin within the first week
inhibitory agents, which causes motor of the rash and remains high for up to
of life, include poor feeding, decreased
neuron discharge. 1 month. Elevated immunoglobulin G
movement, crying, irritability, muscle
Symptoms of generalized tetanus (IgG) levels in convalescent serum,
rigidity, and spasms.
include trismus, facial muscle spasms in comparison to acute-phase serum,
Localized tetanus affects the muscles
(risus sardonicus) (Figure 6), opistho can also help determine the disease
surrounding the injury site and can
tonos, and a rigid abdomen. Dysphagia timeline. Viral cultures of blood, urine,
progress to generalized disease. The
and neck muscle spasms can also mortality rate is lower when the illness or respiratory secretions may also be
occur, and spasms of the laryngeal and remains local. helpful.
respiratory muscles can lead to airway Cephalic tetanus is a distinct type Real-time polymerase chain reaction
compromise. Initially, muscle spasms of localized tetanus that occurs due to (PCR) testing on serum and throat swabs
occur over a few seconds to minutes, injuries to the head or infections of the can be used to confirm measles. An
intermixed with spasm-free intervals. ear or nose. Muscles of the eyes, face, additional urine specimen can be used
As the disease progresses, spasms become tongue, and pharynx are involved; for PCR testing to increase the study’s
longer and more frequent. These events some patients also suffer from cranial sensitivity.5,20 Patients may also have
can be triggered by even minor stimuli, nerve palsies, which can be mistakenly a relative lymphopenia or an absolute
such as noise or touch. attributed to other diseases such as leukopenia, although these findings
Tetanus-related autonomic Bell palsy. Overall mortality is lower in are not diagnostic and are somewhat
disturbances can cause tachycardia, patients with cephalic tetanus than in nonspecific. In some cases, erythrocyte
hypertension, diaphoresis, and dysrhyth those with generalized disease. Some sedimentation rates (ESR) and c-reactive
mias. The illness lasts 6 to 8 weeks, and patients spontaneously recover, although protein (CRP) levels are slightly elevated.
recovery is slow if not fatal.17 Mortality a significant number of cases progress to If there is a bacterial superinfection,
can be as high as 52% in adults and generalized tetanus.19 however, ESR and CRP levels are often
July 2019 n Volume 33 Number 7 7
detect a rise in IgM are not typically used
FIGURE 6. Risus Sardonicus in a Patient with Tetanus due to poor sensitivity and specificity.26
Tetanus
Tetanus is diagnosed based solely on
clinical findings. Clostridium tetani is
identified in only 30% of cases; as a result,
bacteriologic confirmation is unnecessary
and often impractical. Moreover, timely
recognition is important for implementing
early supportive care measures.
CRITICAL DECISION
How should each illness be
treated, and which patients are at
high risk for complications?
Measles
Treatment for measles is typically
PHOTO COURTESY OF CHRISTO PHILLIP, MD
supportive in developed countries,
assuming complications have been
higher, although this is a relatively have been vaccinated or treated with
appropriately ruled out. In normal hosts,
nonspecific test.21 antibiotics. PCR testing for pertussis is
antiviral therapies are neither required nor
Differential diagnoses include, but ideally performed within 3 to 4 weeks
of any benefit. In immunocompromised
are not limited to, rubella, roseola, of the onset of the cough; testing beyond
patients, however, ribavirin may be
toxic shock syndrome, Rocky Mountain 4 weeks can lead to false-negative
beneficial.27
spotted fever, and Kawasaki disease. results. Serology is primarily useful for
Vitamin A therapy has been shown
Testing may be indicated to rule out making a late diagnosis (up to 12 weeks
to decrease morbidity and mortality from
these alternative pathologies. from the onset of the cough).22
A CBC test that reveals leukocytosis measles and can be used in children aged
Mumps with absolute lymphocytosis should 6 months to 2 years. The World Health
As with measles, mumps is a clinical increase suspicion for pertussis. Organization recommends Vitamin A for
diagnosis that can be confirmed by Markedly elevated leukocyte counts all children diagnosed with measles.28
serology. During the acute infection, the can indicate a more severe course; in Because measles causes relative
presence of IgM antibodies corroborates such cases, hospitalization should be immunosuppression, patients are at
the diagnosis. Viral culture or PCR considerered.23 Chest x-rays should increased risk of developing a variety of
testing can also be used to detect the be considered for pediatric patients illnesses during the convalescent period,
mumps virus in respiratory secretions, who also exhibit signs and symptoms including otitis media and pneumonia.
urine, or cerebrospinal fluid (CSF). A of pneumonia, such as shortness of In addition, the late neurological
rise in IgG titers in convalescent serum breath, tachypnea, and hypoxemia. complication of SSPE can develop 7 to 10
compared to acute-phase serum is also Echocardiography can be used to years later, so appropriate counseling and
seen. Serum amylase can be elevated diagnose pulmonary hypertension in follow-up care should be arranged.
with the onset of parotitis, although this severely ill children, although this test Mumps
test is optional. is often unnecessary in the emergency
There are no antiviral therapies
Pertussis department setting.24
for mumps, so treatment is supportive.
Although a positive culture is Varicella Primary treatment for mumps orchitis is
still considered the gold standard for Although varicella is usually scrotal support and bed rest, as needed
diagnosing pertussis, PCR testing is diagnosed based on clinical findings, for pain. Interferon alpha-2b may
equally sensitive and can be performed the disease can be rapidly confirmed by help reduce symptoms that can lead
on nasopharyngeal swab specimens. PCR testing.25 A sample for testing can to testicular atrophy and infertility.29
As a result, PCR testing is growing to be obtained by unroofing a vesicle and Intravenous immunoglobulin (IVIG),
become the clinical test of choice. Direct scraping the base with a collection swab. although of no benefit for post-exposure
fluorescent antibody testing has low A crust from a lesion is a good second prophylaxis, is indicated for the
sensitivity and is less commonly used. choice. Varicella can also be isolated by autoimmune complications of mumps,
Notably, cultures can be falsely negative tissue culture, but this takes longer, is not including Guillain-Barré syndrome,
later in the illness (ie, >2 weeks from as sensitive as PCR testing, and is less idiopathic thrombocytopenia, and post-
the onset of the cough) in patients who routinely performed. Serologic tests to infectious encephalitis.7
8 Critical Decisions in Emergency Medicine
Pertussis not indicated. According to American significant autonomic instability can
When pertussis is suspected, Academy of Pediatrics guidelines, be a prominent feature that requires
macrolide antibiotics should be routine oral antivirals are recommended intensive care management. On
administered to prevent disease only for patients considered to be recovery, tetanus toxoid administration
transmission; however, available at higher risk, such as unvaccinated is required to provide immunity, as
evidence does not suggest that these patients older than 12 years, those with a primary infection does not protect
medications decrease the length of the chronic skin or pulmonary conditions, against subsequent disease.
disease course.30 and patients receiving salicylate or
Trimethoprim-sulfamethoxazole is corticosteroid therapy, including short, CRITICAL DECISION
a recommended second-line agent for intermittent, or aerosolized steroids.36 What measures can help prevent
infants older than 2 months for whom Oral antivirals are also used to treat patients and susceptible contacts
macrolides cannot be used or who have pregnant women and secondary patients
from becoming ill?
pertussis that is resistant to macrolide (eg, family members and close contacts)
treatment.31 Exchange transfusions at risk for severe illness. IV therapy is Measles
have been shown to improve survival indicated for pregnant women with Primary vaccinations for measles are
rates in those with severe pertussis with severe complications of varicella and given at age 12 to 15 months, along with
hyperleukocytosis.32 Extracorporeal immunocompromised patients, including a second dose at age 4 to 6 years. Even
membrane oxygenation (ECMO) is an those taking high-dose corticosteroids during unrelated health care encounters
option for children who have severe for more than 14 days.36 for routine childhood illnesses, clinicians
pulmonary hypertension or are critically should seize the opportunity to
Tetanus
ill, although survival rates are still poor encourage families to maintain proper
Tetanus treatment has two primary
even with intensive treatment.33,34 vaccination schedules.
components: efforts to neutralize any
Infants younger than 4 months and For post-exposure prophylaxis
unbound toxin and supportive care.
any child with a history of cardiac, against measles, immunoglobulin is
Tetanus immune globulin (TIG) is used
pulmonary, neurologic, or muscular indicated up to 6 days after exposure
to eliminate unbound toxins, and any
disorders should be admitted to the for infants younger than age 12 months,
ongoing infections can be treated with
hospital for observation due to the risk pregnant women with no immunity
antibiotics that destroy Clostridium
of complications.35 Infants older than to measles, and immunocompromised
tetani at the wound site. Surgical
4 months should be considered for hosts. Immunoglobulin can also be used
debridement and wound care are also
admission based on the severity of the for individuals with no immunity to
important to decrease the bacterial load.
paroxysms and any history of apnea or measles who have had close, prolonged
Spasms are controlled with muscle
cyanosis. contact with the patient. Between the
relaxants, such as benzodiazepines.
ages of 6 and 11 months, vaccines can
Varicella Although dantrolene and baclofen are
be used instead of immunoglobulin for
Acyclovir or valacyclovir can be commonly used to manage tetanus
post-exposure prophylaxis up to 72 hours
used to treat varicella. To achieve the in the ICU setting, evidence-based
after exposure.5
optimal benefit, medication must be guidelines are limited. In some cases,
initiated within 24 to 72 hours of the neuromuscular-blocking agents are also Mumps
onset of the rash. Antiviral agents used.37 Airway management may be The full mumps vaccination consists
provide only a modest benefit in required, although caution should be of two doses of the measles, mumps, and
otherwise healthy patients; as a result, used to avoid inducing spasms during rubella (MMR) vaccine. Its effectiveness
routine antiviral therapy is generally airway manipulation. In addition, is an estimated 78% for a single dose
and 88% for two doses.9 With time,
however, antibody levels can wane,
and older vaccinated patients can be at
risk for developing mumps, which may
present atypically.38
The MMR vaccine may help prevent
n Failing to report a suspected case of measles or mumps to the local health mumps in the unvaccinated contacts of
department. an infected patient.39 In the event of an
n Neglecting to evaluate for serious complications of vaccine-preventable outbreak, a third dose can be considered
illnesses, including meningitis and encephalitis. for previously vaccinated contacts.40
n Overlooking apnea and cyanosis, the most concerning clinical features of Because the MMR vaccine is live, it is
pertussis, which increase the risk of death in young infants. contraindicated for pregnant women
n Failing to encourage families to maintain proper vaccination schedules. These and immunocompromised patients.
conversations should take place during unrelated health care encounters for
Immunoglobulin is ineffective for post-
routine childhood illnesses.
exposure prophylaxis.9
July 2019 n Volume 33 Number 7 9
cases. VariZIG should be administered
TABLE 1. Tetanus Prophylaxis for Routine Wound Management43,44 as soon as possible, ideally within
Adsorbed Tetanus Minor, Clean Wounds All Other Wounds 96 hours of exposure, although
Toxoid Doses DTaP, Tdap, or Td TIG DTaP, Tdap, or Td TIG some degree of benefit is seen when
Unknown or <3 doses Yes No Yes Yes the drug is given within 10 days.41
administered to date
IVIG can be used when VariZIG is
≥3 doses adminis No (if <10 years since No No (if <5 years since No
tered to date last tetanus-containing last tetanus-containing unavailable. Neonates born to mothers
vaccine dose) vaccine dose) who develop a varicella rash within
Yes (if ≥10 years since Yes (if ≥5 years since 5 days before or 2 days after giving
last tetanus-containing last tetanus-containing birth, exposed pregnant patients, and
vaccine dose) vaccine dose)
immunocompromised individuals
should all receive VariZIG, according
Pertussis fifth dose of DTaP). Children 7 years to the Centers for Disease Control and
Household members, close contacts, and older who have not had a Tdap Prevention.41
and health care workers who did dose should receive one as a booster; Oral acyclovir can be used for
not use masks during the care of a however, there is insufficient data on the prophylaxis for children with no
pertussis patient should be treated with vaccine’s effectiveness for post-exposure evidence of immunity, including those
macrolides. Contacts younger than prophylaxis.22
who are mildly immunocompromised
7 years can receive a DTaP (diphtheria, Varicella or are immunocompetent but for whom
tetanus, pertussis) dose if they have not Susceptible patients should receive prevention is desired. Acyclovir can be
already received a total of four doses. a varicella vaccine within 3 to 5 days administered 7 to 10 days after exposure
DTaP should also be administered to of exposure for optimal benefit and to prevent or reduce the severity of the
close contacts between the ages of 4 and protection.26 Varicella-zoster immune illness; however, there is limited data
6 years who have not already received globulin (VariZIG ) can also provide regarding the drug’s efficacy for post-
the second booster dose (usually the post-exposure prophylaxis in select exposure prophylaxis.36
FIGURE 7. US States with Measles Cases in 2019
Washington
Oregon New Hampshire
Massachusetts
New York
Michigan Connecticut
Iowa New Jersey
Nevada
Illinois Maryland
Indiana
Colorado
Missouri
California Kentucky
Tennessee
Arizona
Georgia
Texas
Florida
ADAPTED FROM THE CENTERS FOR DISEASE CONTROL AND PREVENTION
10 Critical Decisions in Emergency Medicine
CASE RESOLUTIONS
■ CASE ONE The patient’s fever resolved after 2 ■ CASE THREE
The febrile infant’s rash more days, and the rash began to fade The cyanotic 5-week-old infant
was consistent with measles. after 1 week. was admitted to the inpatient floor for
Acetaminophen and ibuprofen were observation. More episodes of coughing
prescribed for fever control, and the ■ CASE TWO and cyanosis occurred; she developed
department of health was notified. The adolescent girl with facial apnea on day 2 and required intubation
Her parents revealed that several swelling was determined to have and mechanical ventilation. Chest
extended family members, including mumps. Supportive management imaging showed an infiltrate suspicious
a 9-month-old boy, also live in their for pneumonia. A CBC test showed a
of her fever and pain with
home. On the recommendation of WBC count of 50,000. Pertussis PCR
ibuprofen and acetaminophen were
the emergency physician, the exposed testing was positive, and the patient was
infant was brought to the emergency recommended. The parotid swelling given azithromycin. She gradually made
department to receive an MMR started to decrease after 5 days and a full recovery and was discharged home
vaccine for post-exposure prophylaxis. resolved completely after 2 weeks. after 16 days.
Tetanus should remain off work, from day 5 after a malignancy, such as leukemia, have
Any patient with a potentially exposure to the first case to day 21 after a high mortality rate (approaching
contaminated injury or wound should exposure to the last case.5 30%) and should be admitted. Adult
receive a tetanus toxoid to prevent patients with primary varicella are also
Mumps
tetanus. TIG may also be indicated. The at much greater risk, with a mortality
As with measles, suspected cases
decision to immunize or administer TIG rate that is more than 25 times that of
of mumps should be reported to the
in the emergency department should children. Most well-appearing patients
local health department. The need for
be made based on the patient’s prior without other risk factors can be treated
hospitalization is rare in the absence of
vaccination history, the amount of time with oral antiviral medications at
an uncommon complication, and most
that has passed since the last tetanus home. Anyone with severe secondary
patients can be discharged home. The
toxoid dose, and whether the wound is complications, such as pneumonia,
highest risk of infection transmission
considered minor or major (Table 1). should be admitted. Children younger
through respiratory droplets and saliva
Immunization is administered as DTaP, than 1 year are also at much higher risk,
occurs from 2 days before to 5 days after
Tdap, or Td based on the patient’s age but most can be managed as outpatients
the onset of parotid swelling, so isolation
and prior vaccination history. Because if they are otherwise well appearing.
precautions at home should be discussed
tetanus is not a contagious disease, no
with patients and their family members.39 Tetanus
prophylaxis is required for any close
contacts or medical personnel. Standard and droplet precautions should Patients with symptoms of tetanus
be followed when managing hospitalized should be admitted to the ICU and are
CRITICAL DECISION patients.39 unsuitable for discharge.
What factors should be Pertussis SUMMARY
considered before discharging Children with pertussis — even those Despite a global decrease in
a patient? with severe disease — often appear normal vaccine-preventable illnesses in recent
between paroxysms. When managing decades, progress has stalled in certain
Measles a young infant, a paroxysm must be
Clinically suspected cases of measles sectors, resulting in a growing public
witnessed to assess severity before a
should be reported to local health health risk. It can be particularly
discharge decision is made. When in doubt,
departments, which can help coordinate challenging to recognize the signs of
emergency physicians should maintain
care and track cases (Figure 7). To measles, mumps, pertussis, varicella,
a low threshold for admission when
prevent the spread of the disease, and tetanus, five vaccine-preventable
evaluating infants younger than 4 months.
patients and their household contacts diseases that carry potentially deadly
The vast majority of older patients can be
should use airborne isolation precautions complications. It is imperative for
discharged home with appropriate follow-
for approximately 4 days after the rash emergency physicians to understand
up care and public health reporting.
begins. Due to prolonged viral shedding, which diagnostic tests are warranted,
immunocompromised patients may Varicella know when to administer vaccines
require isolation for the entire duration The severity of each varicella case or immunoglobulins, and formulate
of the disease.5,42 Moreover, exposed is dependent on the patient’s age and appropriate disposition plans based on
health care workers with no immunity underlying immune status. Patients with the characteristics of each case.
July 2019 n Volume 33 Number 7 11
REFERENCES 25. Leung J, Harpaz R, Baughman AL, et al. Evaluation of
laboratory methods for diagnosis of varicella.
1. Centers for Disease Control and Prevention (CDC). Clin Infect Dis. 2010 Jul 1;51(1):23-32.
Notes from the field: measles outbreak among 26. Varicella. In: Centers for Disease Control and
members of a religious community - Brooklyn, New Prevention; Hamborsky J, Kroger A, Wolfe C, eds.
York, March-June 2013. MMWR Morb Mortal Wkly Epidemiology and Prevention of Vaccine-Preventable
Rep. 2013 Sep 13;62(36):752-753. Diseases. 13th ed. Washington, DC: Public Health
2. Perry RT, Halsey NA. The clinical significance of Foundation; 2015:353-376.
measles: a review. J Infect Dis. 2004 May 1;189 27. Roy Moulik N, Kumar A, Jain A, Jain P. Measles
(suppl 1):S4-S16. outbreak in a pediatric oncology unit and the role
3. Helfand RF, Kim DK, Gary HE Jr, et al. Nonclassic of ribavirin in prevention of complications and
measles infections in an immune population exposed containment of the outbreak. Pediatr Blood Cancer.
to measles during a college bus trip. J Med Virol. 2013 Oct;60(10):e122-e124.
1998 Dec;56(4):337-341. 28. Measles. World Health Organization website. http://
4. Rota JS, Hickman CJ, Sowers SB, Rota PA, Mercader www.who.int/news-room/fact-sheets/detail/measles.
S, Bellini WJ. Two case studies of modified measles in Published November 2018. Updated May 9, 2019.
vaccinated physicians exposed to primary measles Accessed June 13, 2018.
cases: high risk of infection but low risk of trans 29. Ku JH, Kim YH, Jeon YS, Lee NK. The preventive
mission. J Infect Dis. 2011 Jul;204(suppl 1):S559-S563. effect of systemic treatment with interferon-alpha2B
5. Measles. In: Centers for Disease Control and for infertility from mumps orchitis. BJU Int. 1999 Nov;
Prevention; Hamborsky J, Kroger A, Wolfe C, eds. 84(7):839-842.
Epidemiology and Prevention of Vaccine-Preventable 30. Altunaiji SM, Kukuruzovic RH, Curtis NC, Massie J.
Diseases. 13th ed. Washington, DC: Public Health Cochrane Review: antibiotics for whooping cough
Foundation; 2015:209-229. (pertussis). Evid Based Child Health. 2012 May 3;
6. Richardson M, Elliman D, Maguire H, Simpson J, 7(3):893-956.
Nicoll A. Evidence base of incubation periods, 31. Pertussis (whooping cough). In: Red Book: 2018-2021
periods of infectiousness and exclusion policies for Report of the Committee on Infectious Diseases. 31st
the control of communicable diseases in schools and ed. Itasca, IL: American Academy of Pediatrics;
preschools. Pediatr Infect Dis J. 2001 Apr;20(4): 2018:620-634.
380-391. 32. Kuperman A, Hoffmann Y, Glikman D, Dabbah H,
7. Hviid A, Rubin S, Mühlemann K. Mumps. Lancet. 2008 Zonis Z. Severe pertussis and hyperleukocytosis: is it
Mar 15;371(9616):932-944. time to change for exchange? Transfusion. 2014 Jun;
8. Johnstone JA, Ross CA, Dunn M. Meningitis and 54(6):1630-1633.
encephalitis associated with mumps infection. A 10- 33. Halasa NB, Barr FE, Johnson JE, Edwards KM. Fatal
year survey. Arch Dis Child. 1972 Aug;47(254):647-651. pulmonary hypertension associated with pertussis in
9. Mumps: for healthcare providers. Centers for Disease infants: does extracorporeal membrane oxygenation
Control and Prevention website. https://www.cdc.gov/ have a role? Pediatrics. 2003 Dec;112(6, pt 1):
mumps/hcp.html. Updated March 15, 2019. Accessed 1274-1278.
June 18, 2018. 34. De Berry BB, Lynch JE, Chung DH, Zwischenberger
10. Davis NF, McGuire BB, Mahon JA, Smyth AE, JB. Pertussis with severe pulmonary hypertension
O’Malley KJ, Fitzpatrick JM. The increasing incidence and leukocytosis treated with extracorporeal
of mumps orchitis: a comprehensive review. BJU Int. membrane oxygenation. Pediatr Surg Int. 2005 Aug;
2010 Apr;105(8):1060-1065. 21(8):692-694.
11. Bengtsson E, Orndahl G. Complications of 35. Cherry JD, Wendorf K, Bregman B, et al. An obser
mumps with special reference to the incidence of vational study of severe pertussis in 100 infants
myocarditis. Acta Med Scand. 1954;149(5):381-388. ≤120 days of age. Pediatr Infect Dis J. 2018 Mar;
12. Vittucci AC, Spuri Vennarucci V, Grandin A, et al. 37(3):202-205.
Pertussis in infants: an underestimated disease. BMC 36. Varicella-zoster virus infections. In: Red Book: 2018-2021
Infect Dis. 2016 Aug 15;16(1):414. Report of the Committee on Infectious Diseases. 31st ed.
13. Cornia PB, Hersh AL, Lipsky BA, Newman TB, Itasca, IL: American Academy of Pediatrics; 2018:
Gonzales R. Does this coughing adolescent or adult 869-883.
patient have pertussis? JAMA. 2010 Aug 5;304(8): 37. Rodrigo C, Fernando D, Rajapakse S. Pharma
890-896. cological management of tetanus: an evidence-
14. Philipson K, Goodyear-Smith F, Grant CC, Chong A, based review. Crit Care. 2014 Mar 26;18(2):217.
Turner N, Stewart J. When is acute persistent cough 38. Myung NS, Kim YJ, Kim YJ, Koo SK. Complicated
in school-age children and adults whooping cough? mumps viral infection: an unusual presentation
A prospective case series study. Br J Gen Pract. 2013 affecting only submandibular gland. Am J
Aug;63(613):e573-e579. Otolaryngol. 2013 Sep-Oct;34(5):600-602.
15. Chan MH, Ma L, Sidelinger D, et al. The California 39. Centers for Disease Control and Prevention (CDC).
pertussis epidemic 2010: a review of 986 pediatric Updated recommendations for isolation of persons
case reports from San Diego County. J Pediatric with mumps. MMWR Morb Mortal Wkly Rep. 2008
Infect Dis Soc. 2012 Mar;1(1):47-54. Oct 10;57(40):1103-1105.
16. Watts CC, Acosta C. Pertussis and bilateral subdural 40. Marin M, Marlow M, Moore KL, Patel M.
hematomas. Am J Dis Child. 1969 Sep;118(3):518-519. Recommendation of the Advisory Committee on
17. Thwaites CL, Beeching NJ, Newton CR. Maternal and Immunization Practices for use of a third dose
neonatal tetanus. Lancet. 2015 Jan 24;385(9965): of mumps virus-containing vaccine in persons at
362-370. increased risk for mumps during an outbreak. MMWR
18. Trujillo MH, Castillo A, España J, Manzo A, Zerpa Morb Mortal Wkly Rep. 2018 Jan 12;67(1):33-38.
R. Impact of intensive care management on the 41. Centers for Disease Control and Prevention (CDC).
prognosis of tetanus. Analysis of 641 cases. Chest. Updated recommendations for use of VariZIG—
1987 Jul;92(1):63-65. United States, 2013. MMWR Morb Mortal Wkly Rep.
19. Jagoda A, Riggio S, Burguieres T. Cephalic tetanus: a 2013 Jul 19;62(28):574-576.
case report and review of the literature. Am J Emerg 42. Permar SR, Moss WJ, Ryon JJ, et al. Prolonged
Med. 1988 Mar;6(2):128-130. measles virus shedding in human immunodeficiency
20. Woo GK, Wong AH, Lee WY, et al. Comparison of virus-infected children, detected by reverse
laboratory diagnostic methods for measles infection transcriptase-polymerase chain reaction. J Infect Dis.
and identification of measles virus genotypes in 2001 Feb 15;183(4):532-538.
Hong Kong. J Med Virol. 2010 Oct;82(10):1773-1781. 43. Tetanus (lockjaw). In: Red Book: 2018-2021 Report
21. Griffin DE, Hirsch RL, Johnson RT, De Soriano IL, of the Committee on Infectious Diseases. 31st ed.
Roedenbeck S, Vaisberg A. Changes in serum Itasca, IL: American Academy of Pediatrics; 2018:
C-reactive protein during complicated and 793-798.
uncomplicated measles virus infections. Infect 44. Liang JL, Tiwari T, Moro P, et al. Prevention of
Immun. 1983 Aug;41(2):861-864. pertussis, tetanus, and diphtheria with vaccines in
22. Pertussis. In: Centers for Disease Control and the United States: recommendations of the Advisory
Prevention; Hamborsky J, Kroger A, Wolfe C, eds. Committee on Immunization Practices (ACIP). MMWR
Epidemiology and Prevention of Vaccine-Preventable Recomm Rep. 2018 Apr 27;67(2):1-44.
Diseases. 13th ed. Washington, DC: Public Health
Foundation; 2015:261-278.
23. Pierce C, Klein N, Peters M. Is leukocytosis
a predictor of mortality in severe pertussis
infection? Intensive Care Med. 2000 Oct;26(10):
1512-1514.
24. Casano P, Odena MP, Cambra FJ, Martín JM,
Palomeque A. Bordetella pertussis infection causing
pulmonary hypertension. Arch Dis Child. 2002 Jun;
86(6):453.
12 Critical Decisions in Emergency Medicine
A 68-year-old man with dyspnea, hypotension, and evidence of pulmonary edema.
The Critical ECG
Sinus tachycardia, rate 125, acute anterior-lateral myocardial infarction. At first By Amal Mattu, MD, FACEP
glance, the ECG appears to reflect a wide QRS complex tachycardia. However, Dr. Mattu is a professor, vice chair, and
director of the Emergency Cardiology
leads II and V1 clearly demonstrate that the QRS complexes are narrow, and it is Fellowship in the Department of
Emergency Medicine at the University
the marked ST-segment deflections (elevations or depressions) that give the false
of Maryland School of Medicine in
appearance of wide QRS complexes. A truly wide QRS complex rhythm should Baltimore.
demonstrate wide complexes in every lead. Marked ST-segment elevation (STE)
is present in the anterior (V2-V4) and lateral (V5, V6, I, and aVL) leads, and reciprocal
ST-segment depression is present in the inferior leads and in lead V1. When diffuse
STE is present, these reciprocal changes exclude other causes of STE, such as
pericarditis, benign early repolarization, ventricular aneurysm, and left ventricular
hypertrophy.
From Mattu A, Brady W. ECGs for the Emergency Physician 2. London: BMJ Publishing; 2008. Reprinted with permission.
July 2019 n Volume 33 Number 7 13
The Critical Image
A 62-year-old man with hypertension presents with 5 days of nontraumatic By Joshua S. Broder, MD, FACEP
neck pain. He describes severe, burning, midline cervical pain that radiates to Dr. Broder is an associate professor and the
residency program director in the Division
the back of his head. His symptoms, which are progressive and constant, are
of Emergency Medicine at Duke University
now associated with numbness in his hands. The patient also reports difficulty Medical Center in Durham, North Carolina.
swallowing solid foods but denies fever. He is a former cigarette smoker but Case contributor: Brian Nelson, MD
denies drug or alcohol use. An urgent care center performed screening x-rays
of the patient’s cervical spine before referring him to the emergency department.
His vital signs are blood pressure 168/93, heart rate 76, respiratory rate 18, temperature 37.5°C (99.5°F), and oxygen saturation
94% on room air. His cervical pain is not reproducible with palpation. His physical and neurologic examinations are otherwise
normal, and he has no stridor or drooling.
The emergency physician reviews the patient’s cervical x-ray, places him in a Miami J cervical collar, and obtains additional
imaging.
KEY POINTS A
n Cervical spine instability can result
from trauma and malignant or
infectious processes. The flexion-
extension images presented here
demonstrate subluxation of the
cervical spine, which increases the
risk of spinal cord injury.
n Flexion-extension imaging should
be performed with caution, and
— when instability is suspected —
preferably in consultation with a
C1 vertebra
spine surgeon. If flexion-extension
images are obtained, the patient
should actively perform cervical Lytic
motion, stopping immediately if any destruction
neurologic symptoms arise. of C2
n Passive cervical motion (ie, vertebral
movement of the cervical spine body
by an external operator) increases
the risk of spinal cord injuries and
should never be performed. C3 vertebra
n When malignancy is suspected, CT
with intravenous (IV) contrast can
further delineate the spinal lesion
and identify a primary mass. MRI of
the spine may also be necessary to
characterize spinal cord or epidural
involvement. A. Lateral cervical spine x-ray demonstrating lytic destruction of the C2
vertebral body. This lesion destabilizes the patient’s cervical spine and creates
a risk of spinal cord injury caused by cervical motion.
CASE RESOLUTION
The patient was admitted, and a biopsy of his renal mass confirmed renal cell carcinoma.
His cervical spine was surgically fixated, and he underwent radiation therapy.
14 Critical Decisions in Emergency Medicine
B. Flexion
B C
radiograph;
C. Extension
radiograph.
These images C1 vertebra
reveal dynamic and dens,
instability, with anteriorly
subluxation subluxed
of C1 and
the dens
C2 vertebra
relative to the
remainder of
the cervical
spine.
C3 vertebra
D. CT of the
D E cervical spine and
soft tissues of the
Dens neck, performed
with IV contrast.
With bone windows,
the extent of C2
destruction is
evident.
C1
vertebra E. Same data set
as Figure B, soft-
tissue windows.
An enhancing
soft-tissue mass in
Lytic Peripherally C2 is evident. This
destruction enhancing, finding suggests
of C2 C3 expansile, lytic metastatic disease
vertebral vertebral lesion of C2 (as opposed to
body body vertebral body osteomyelitis with
osteolysis).
F. CT of the chest, F G
abdomen, and
pelvis with IV
contrast. The test
was performed
to identify a
suspected primary
malignant lesion of
unknown location.
A heterogeneously
enhancing mass
in the left kidney
suggests renal cell
carcinoma.
G. Lateral x-ray
following internal Heterogeneously
spinal fixation. enhancing
renal mass
July 2019 n Volume 33 Number 7 15
Critical Cases
in Orthopedics and Trauma
Malleolar Ankle Fracture
By John Kiel, DO, MPH; and Roseline Desvaristes, MD
University of Florida College of Medicine – Jacksonville
A 56-year-old woman presents after falling while walking her dog. As she fell, she twisted her
left ankle in the opposite direction of her path. She explains that she experienced an immediate
onset of pain in the extremity, and severe swelling developed 30 minutes later. In the emergency
department, an obvious ankle deformity is noted with mild, medial deviation and eversion of the
foot. The patient’s neurovascular examination is intact, and the skin is intact. She complains of
mild tenderness over the knee joint laterally.
Fracture Reduction and Splinting
FIGURE 1. Medial Malleolus Fracture
Radiographs identified a trimalleolar fracture with
anterior-posterior dislocation of the talus and a spiral
fibular neck fracture, consistent with a Maisonneuve
injury. Pain control was achieved with intravenous
fentanyl (100 mcg), an oral dose of hydrocodone, and a
hematoma block. With the patient in a supine position,
chlorhexidine was used to prepare the injection site,
which was located anteromedially between the medial
malleolus and the tibialis anterior tendon. The fracture
hematoma was aspirated with a 23-gauge needle, and
10 mL of 1% lidocaine was injected.
Reduction was achieved by grasping the midfoot
and calcaneus and applying axial traction. The talus was
further manipulated anteriorly to achieve anatomical
alignment with the articular surface of the tibia. A
combined posterior and stirrup splint was used to
stabilize the posterior ankle and foot to prevent plantar-
and dorsiflexion.
CASE RESOLUTION
Following reduction and splinting, the patient
continued to experience considerable swelling
and was strictly advised to elevate her foot
and avoid bearing weight. She was discharged
in stable condition. On follow-up, her initial
radiographs were found to be misleading;
the orthopedic staff determined that the
patient had a bimalleolar fracture rather than
REFERENCES
a trimalleolar injury. She underwent an open 1. Daly PJ, Fitzgerald RH Jr, Melton LJ, Ilstrup DM. Epidemiology of ankle fractures in
reduction and internal fixation of the medial Rochester, Minnesota. Acta Orthop Scand. 1987 Oct; 58:539-544.
2. Elsoe F, Ostgaard SE, Larsen P. Population-based epidemiology of 9767 ankle fractures. Foot
and lateral malleoli 9 days later. Ankle Surg. 2018 Feb;24(1):34-39.
3. Kalyani BS, Roberts CS, Giannoudis PV. The Maisonneuve injury: a comprehensive review.
Orthopedics. 2010 Mar;33(3):196-197.
16 Critical Decisions in Emergency Medicine
FIGURE 2. Bimalleolar Fracture FIGURE 3. Trimalleolar Fracture
KEY POINTS
n Malleolar injuries account for the vast majority of ankle n Supination-adduction, supination-external rotation, and
fractures. Lateral malleolus fractures account for 55% pronation-external rotation result in various malleolar
of these cases, and trimalleolar fractures account for and fibular fractures and disruption of the syndesmotic
approximately 7% to 12%.1,2 and deltoid ligaments. Supination-external rotation, the
n A unimalleolar fracture, an isolated injury in one of the most common cause of ankle fractures, can damage the
malleoli (Figure 1), can remain stable if no additional distal fibula and result in avulsion of the posterior-inferior
ligament injury is present. A stress-view radiograph tibiofibular ligament. While this mechanism can lead to
can further help identify instability by demonstrating Maisonneuve fractures, pronation-external rotation is
widening of the ankle mortise. A bimalleolar-equivalent reported in more than half of these cases.3
fracture (Figure 2), which involves both the medial and n Ankle injuries can prevent patients from returning to
their previous level of activity and can result in job
lateral malleoli, should be suspected if a lateral talar
loss, osteoarthritis, and chronic pain. When evaluating
shift is present. In such cases, an additional injury to the
these cases, the physician should perform a thorough
deltoid ligament can cause subsequent joint instability.
neurovascular examination and carefully examine the joint
The trimalleolar fracture (Figure 3) is so termed because
above and below the site of injury.
it involves an additional fracture at the posterior edge
n In general, stable ankle fractures are managed with
of the tibia.
immobilization, elevation, and ice therapy as tolerated. A
n An ankle injury that is accompanied by a high fibular short-leg walking cast or a cast boot worn for 4 to 6 weeks
fracture and disruption of the syndesmosis is called a can be useful. Unstable ankle fractures (eg, bimalleolar,
Maisonneuve fracture. This pathology is often missed bimalleolar equivalent, trimalleolar) require immediate
in the initial evaluation.3 Patients may be distracted by closed reduction and splinting to prevent tissue ischemia,
the severity of their ankle pain and not complain of pain avert articular surface damage, and help resolve swelling.
proximally. Three-view radiographs are indicated; stress The definitive management of these injuries involves open
views may be necessary. The Ottawa Ankle Rules can reduction and internal fixation. Maisonneuve fractures may
help reduce unnecessary imaging. require surgical management if there is true syndesmosis
n Malleolar fractures are classified by the Danis-Weber, instability or compression of the superficial fibular nerve
AO/OTA, and Lauge-Hansen classification systems. with subsequent motor weakness.
July 2019 n Volume 33 Number 7 17
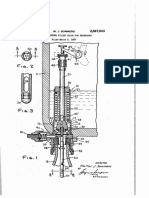
The Critical Procedure
Starting or Stopping an Implanted
Vagal Nerve Stimulator
By Steven J. Warrington, MD, MEd
Dr. Warrington is the director of the Emergency Medicine
Residency Program and academic chair of the Department of
Emergency Medicine at Orange Park Medical Center in Orange Park, Florida.
Implanted vagal nerve stimulators (VNS) can be
used to manage multiple conditions, including epilepsy,
mood disorders, and migraines, by delivering electrical
impulses along the left vagus nerve to the brain stem.
Patients frequently present to the emergency
department for acute conditions that can be
managed by triggering or disabling the device.
Benefits and Risks Special Considerations To avoid accidental stimulation,
On-demand VNS stimulation can Patients who undergo VNS implanta clinicians should be mindful of the
be used to stop or treat seizure activity. tion are typically provided with a position of the magnet in relationship
Conversely, pain, coughing, and other to the patient. It is also important to
bar-shaped magnet that matches the
understand that these devices do not
side effects associated with these devices shape of their device. Magnets found in
provide continuous stimulation. Each
can be relieved by temporarily disabling emergency departments, most of which VNS is programmed to stimulate the
the stimulation they provide. are circular, may fail to stop or induce vagus nerve according to a particular
Disabling a VNS can inadvertently stimulation. Whenever possible, the frequency or pattern. Activating the
induce stimulation and its associated patient’s device-specific magnet should device simply triggers its preprogrammed
risks, including dyspnea, voice problems, be used. stimulation sequence (eg, hourly).
coughing, and pain. Rare incidents of
bradycardia and asystole have also been TECHNIQUE
reported.
STOPPING a VNS
Alternatives 1. Locate an appropriate magnet,
Alternative therapies primarily focus preferably bar shaped.
on resolving the complaints noted 2. Identify the location of the VNS by
earlier. Certain symptoms that can be palpating the patient’s left chest.
provoked by a VNS, including pain and 3. Place the magnet over the top of
spasms, may be more difficult to treat. the device. If the magnet is circular,
consider slowly approaching the
Reducing Side Effects
VNS from the side until symptoms
It is important to understand that
resolve.
the clinician can induce on-demand
4. Secure the magnet in place. (Any
stimulation by using a magnet to close
movement may induce stimulation.) VNS Magnet
and open a switch within the VNS.
When planning to disable a device, on TRIGGERING a VNS 3. Move the magnet over the device,
the other hand, efforts must be made 1. Locate an appropriate magnet. hold it in place for 1 to 2 seconds,
to keep the magnet in place, as removal 2. Identify the location of the VNS by and then quickly remove it.
(or position changes) will prompt palpating the patient’s left chest. 4. Repeat if necessary.
stimulation.
18 Critical Decisions in Emergency Medicine
Observation
Deck
Emergency Department
Observation Care
LESSON 14
By Robert M. Bramante, MD, FACEP;
and Christopher C. Raio, MD, MBA, FACEP
Dr. Bramante is codirector of observation medicine and associate chairman of
emergency medicine, and Dr. Raio is chairman of emergency medicine at Good
Samaritan Hospital Medical Center in West Islip, New York.
Reviewed by John C. Greenwood, MD
OBJECTIVES
On completion of this lesson, you should be able to: CRITICAL DECISIONS
1. Describe the various types of hospital observation
n How should observation services be defined?
care.
2. Explain the difference between inpatient admission n Which patients should be selected for
and observation status. observation?
3. Identify patients who are appropriate for protocolized
n How can protocolized observation units be used
observation care.
4. Discuss the goals of observation care. to streamline patient care?
5. Summarize the management goals and metrics n What metrics and quality data matter most when
associated with observation medicine. operating an observation unit?
FROM THE EM MODEL n Who should manage the protocolized
20.0 Other Core Competencies of the Practice observation unit?
of Emergency Medicine
20.4 Systems-Based Practice
Observation units are increasingly used to manage acute presentations when safe discharge is in doubt and
the need for inpatient admission is unclear. While there are a number of existing models for this approach to
care, emergency departments have become keenly invested in the surge of new, protocolized observation care.
As such, clinicians must be prepared to maximize this safety net by selecting appropriate patients for monitoring
and using interdisciplinary protocols to expertly manage them.
July 2019 n Volume 33 Number 7 19
CASE PRESENTATIONS
■ CASE ONE ■ CASE TWO ■ CASE THREE
A 51-year-old man with a A 72-year-old woman presents A 42-year-old man presents with
history of hypertension presents via ambulance with an episode of sharp, severe, left flank pain that is
via ambulance with moderate slurred speech that started 5 hours radiating to his groin. He has had
chest pressure that radiates to his prior to arrival. She complains of two to three bouts of renal colic
left shoulder. He explains that left-sided facial numbness and left over the past 6 years but has passed
the symptoms began an hour ago leg weakness but notes that her stones spontaneously after receiving
while he was walking to work. symptoms are improving. She has a treatment on all prior occasions. He
The pain is nonpleuritic and has had multiple episodes of nausea
history of type 2 diabetes mellitus,
associated with mild shortness and vomiting over the past 8 hours,
hypertension, and intermittent vertigo.
of breath. He has no back pain, which have been nonbloody and
Although the patient initially did not
abdominal pain, nausea, vomiting, nonbilious. There is no chest pain
think much of the event, a concerned
or diaphoresis. The patient does or shortness of breath. The patient
friend encouraged her to call 911 after
not take aspirin and smokes half denies dysuria and gross hematuria.
learning of her symptoms. She took a He drinks alcohol socially, does not
of a pack of cigarettes daily. He
325-mg aspirin prior to arrival. The smoke, takes no medications, and
reports no recent immobility
patient describes no recent trauma, denies other medical problems. He is
or travel. His family history
headache, or pain. afebrile and tachycardic at 118 beats
is significant for hypertension
The patient’s vital signs are per minute.
without coronary artery disease.
significant for hypertension with a His physical examination is
Paramedics administered
blood pressure of 164/92. Her physical significant for moderate distress due
325 mg of aspirin while en route
examination is significant for 4/5 to pain; he is writhing in bed and
to the hospital, and the patient’s
left lower-extremity strength with has left flank and lower-quadrant
symptoms are now improving.
normal sensation and mild dysarthria, abdominal tenderness without rebound
An initial ECG reveals isolated
which equates to a National Institute or guarding. His genitourinary exam
T-wave inversions in leads V5
of Health Stroke Scale score of 2. ination is normal. Laboratory tests
through V6 . No prior ECG is demonstrate no leukocytosis, a normal
available for comparison. His An ECG demonstrates normal
sinus rhythm with left ventricular creatinine level, and hypokalemia at
vital signs are within normal 2.6 mEq/L. Urinalysis is positive for
limits, and his lungs are clear. hypertrophy. An initial CT of her
blood and 1 to 2 WBC/hpf, without
His cardiac and abdominal brain is normal, with no evidence of a
leukocyte esterase or nitrites. A
examinations are normal, and he stroke, intracranial hemorrhage, shift,
focused, point-of-care ultrasound
has equal pulses, no reproducible or mass. Her laboratory evaluation is
examination reveals mild left-sided
pain, and no extremity edema. unremarkable, except for mild anemia
hydronephrosis and a hyperechoic
Initial laboratory tests, including with a hemoglobin level of 11.2 g/dL. focus measuring 3 mm with posterior
his troponin level, are normal. Neurology recommends evaluating shadowing at the left ureterovesical
The emergency physician the patient for a cerebrovascular junction.
informs the patient that he will be accident versus a resolving transient Despite intravenous (IV) hydration
transferred to the observation unit ischemic attack. The observation unit and analgesia, the patient’s pain and
for further telemetry monitoring, physician is called to further assess vomiting persist. The emergency
provocative cardiac testing, and the patient’s appropriateness for physician considers further
frequent reevaluation. observation care. management in the observation unit.
While many observation units admission is becoming increasingly necessary to evaluate the outpatient’s
were initially dedicated to the rigorous, these valuable units exist in condition or determine the need
evaluation of chest pain (Figure 1), only about one-third of US hospitals.1 of that patient’s admission to the
they have since expanded to The Centers for Medicare and
hospital as an inpatient.”2
address numerous diagnoses that Medicaid Services (CMS) has continued
In addition to providing patients
require management, testing, and to increase the scope of observation,
with focused care, these units help
reevaluation beyond the scope of the with the addition of the Two-Midnight
emergency department. Although Rule and new assessments of medical hospitals prevent inappropriate
observation medicine is rapidly necessity. Medicare defines observation admissions, subsequent CMS audits,
evolving, and the criteria for hospital as services “that are reasonable and and the loss of vital revenue.3
20 Critical Decisions in Emergency Medicine
CRITICAL DECISION under Medicare Part B. Observation is are four distinct types of observation
now used to determine whether patients care. The type 1 (scattered) model, in
How should observation
receiving ongoing treatment can be which beds are dispersed throughout the
services be defined? safely discharged within 24 hours or hospital, allows any provider to manage
In decades past, emergency physicians require inpatient care. Although various patients under observation. This scenario
were forced to answer a binary question reimbursement rules have been applied to actually shifts costs from the payers to
when determining the disposition for each observation care over the last 30 years, the hospital; care proceeds as it would for
case: Can this patient be safely discharged most payers now recognize its unique any admitted patient — only for a shorter
home, or is inpatient admission required advantages and routinely cover the period of time.4,6 The type 2 (open) model
for the provision of further testing and services these units provide. describes a distinct unit in which any
treatment? In 1983, however, CMS CMS defines observation as a admitting clinician can place and manage
limited Medicare costs by creating a “well-defined set of specific, clinically observation cases.
payment system based on admission appropriate services, which include Type 3 (virtual) care is directed by
criteria. Under this new model, Medicare ongoing short-term treatment, observation protocols, but the patients are
payments are based on the diagnosis, assessment, and reassessment before a spread throughout the hospital without a
rather than on each service rendered.4 decision can be made regarding whether designated unit. Finally, a type 4 (closed)
This change, which mandates that the patients require further treatment as unit is a separate, distinct space in
hospitals assume more risk, eventually led hospital inpatients or if they are able to which clinicians develop and implement
to the development of observation care. be discharged from the hospital.”5 interdisciplinary protocols for patient
As opposed to inpatient services, While observation is a status, not a care.6 This space is optimally located
which are covered under Medicare location, this article will focus on closed, within or adjacent to the emergency
Part A, observation care is covered protocol-driven observation units. There department.
FIGURE 1. One Sample Algorithm for the Observation of Chest Pain
CHEST PAIN SYNDROME
OR POSSIBLE ACUTE CORONARY SYNDROME (ACS)
Possible ACS
Clinical Assessment: Definite ACS:
NOT cardiac Unstable angina
Non–ST-elevation
Age ≤75 years with no known Age ≥75 years or known
myocardial infarction
coronary artery disease coronary artery disease
ST-elevation myocardial
Consider other diagnoses infarction
• ECG and troponin at 0 hours
(follow up with ECG and troponin at 0, 3,
(if pain >6 hours ago)
primary care provider) and 6 hours
• ECG and troponin at 0 and
3 hours (if pain 3-6 hours ago) Admit/
• ECG and troponin at 0, 3, and cardiology consultation
6 hours (if pain <3 hours ago)
No recurrent angina, ECG (–)
Recurrent angina, ECG (+) and troponin(s) (–)
or troponin(s) (+)
Business hours:
Admit/ Stress test
cardiology consultation
After hours:
Dismiss with 1-3 day Abnormal Normal
cardiology follow-up for
possible stress testing
Admit/ Dismiss (follow up with
cardiology consultation primary care provider)
July 2019 n Volume 33 Number 7 21
Regardless of the model employed, the first 24 hours of care, the average own to meet their unique needs, workflow,
emergency physicians must ensure length of stay has increased over the resources, and patient populations. The
that patients receive the appropriate past decade, as payers have directed key is to create standardized pathways that
level of care (inpatient vs observation more complex cases toward this clinical optimize efficiency and outcomes. These
vs discharge) by contributing to the model.4,7 Under Medicare’s Two-Midnight protocols have been shown to improve
appropriate disposition decision. Rule, care must cross two midnights care at lower costs than inpatient treatment
before the case is deemed an inpatient (Figure 2).7
CRITICAL DECISION admission, while treatment provided Because patients with multiple, acute
Which patients should be for less than two midnights must problems often cannot be managed with
selected for observation? meet additional, specific criteria to be streamlined pathways, focused protocols
considered inpatient care.8 It is important should provide specific inclusion and
Observation is inappropriate for
to recognize that the time spent under exclusion criteria and outline necessary
two primary populations: patients
observation does not count toward the diagnostic tests and treatment. Protocolized
who meet the criteria for inpatient care
3 days a Medicare patient must spend as care fosters clinical consistency and more
and those whose emergent condition
an “inpatient” before becoming eligible for efficient patient management.10 When
has been treated, allowing them to be
skilled nursing facility coverage. developing these standards, it is important
safely discharged home directly from
In emergency medicine–operated, to ask: Does this test or treatment need to
the emergency department. CMS uses
protocolized observation units, treatment be completed during this visit?
standardized criteria to help determine if
and disposition should be completed in Protocols should focus on the key
an individual qualifies for inpatient care.
less than 24 hours to allow for continued tests required to determine the need for
Several reliable triage tools, including
the InterQual Criteria and Milliman throughput and flow.4 The average outpatient follow-up or hospital admission.
Care Guidelines, can help determine the length of stay in an emergency medicine Unnecessary testing and procedures
need for hospital admission; however, observation unit is 15 hours; more than can increase the average length of stay,
these protocols are not all-inclusive and 80% of these patients are discharged home needlessly occupy valuable resources, and
should not supersede documented clinical after the observation period.9,10 The ideal decrease monetary returns. It is important
judgment. observation patient has a limited illness to note that Medicare pays facilities a fixed
Conversely, there are two populations that requires a limited intensity of care.4 fee for observation services, which means
that should be considered for observation the hospital shares the financial risk.
status: patients who require further CRITICAL DECISION
CRITICAL DECISION
treatment and testing to determine How can protocolized
their need for inpatient admission and What metrics and quality data
observation units be used to
those who need prolonged treatment or matter most when operating an
streamline patient care?
evaluation in the emergency department observation unit?
but are not well enough to be discharged Protocolized observation units
can help hospitals avoid unnecessary Many observation metrics closely
home. Examples include patients
admissions and risky emergency depart mirror standards used in the emergency
with low- to moderate-risk chest pain
ment discharges, increase throughput, department. Data on the unit’s volume,
(pending serial cardiac enzyme testing),
enhance the patient experience, and utilization patterns, average length of stay,
a transient ischemic attack (pending
final disposition, and completion of care
further advanced imaging), or asthma ultimately improve clinical care.
should be tracked on a weekly, monthly,
that requires ongoing nebulizer treatment, While numerous guidelines have
and yearly basis. Volume data includes the
monitoring, and reevaluation. been developed for the management of
quantity of observation cases, number and
Although emergency department observation patients, institutions can
percentage of cases sorted by diagnosis
observation has historically focused on modify these protocols or create their
and final disposition, and the number
of observation cases compared to the
total number of emergency department
patients.4
It also helps to be aware of the
hospital’s concurrent case review and
n Plan ahead by staffing the observation unit with clinicians who are adaptable, insurance denials, as this information
responsible, and understand the goals of observation medicine. may provide opportunities to increase
n Meet with key personnel (eg, hospital leadership, medical billing, clinical staff) observation unit volume while decreasing
prior to initiating observation services. the hospital’s exposure to CMS audits.4,7
n Identify a leader within the emergency department to manage the unit, follow This information, in conjunction with the
the metrics, and educate staff on protocolized observation care. ratio of emergency department to hospital
n The observation unit is an important safety net that also enables clinicians to
admissions, can help measure the effect of
monitor emergency department care and operations.
observation on hospital utilization.
22 Critical Decisions in Emergency Medicine
Each length of stay is another crucial
metric, as patients who require less than 6 FIGURE 2. Relative Costs for Observation vs Inpatient Care
to 8 hours of care are unlikely candidates
EMERGENCY DEPARTMENT INPATIENT
for observation. Most cases should include
OBSERVATION UNIT 2%
a plan for discharge or admission within
18 to 24 hours, and a typical length of 2% 3% 3% 4%
1%
stay should be targeted at 15 hours.10,11 3%
By carefully tracking every diagnosis, 9%
17%
emergency physicians can tailor the 25%
observation unit’s priorities and resources
to the presenting patient population.
Laboratory and imaging turnaround times 24%
38% 8%
are also important to monitor, as they can
add significant time to the length of stay
of inappropriately prioritized observation 9%
7%
patients. 10% 35%
While it is important to regularly
evaluate the unit’s patient volume, quality
measurements are an equally valuable
barometer of success. Quality metrics Electrical Emergency
cardioversion Diagnostic Echocardiography Imaging department
include data about post-observation Fees charged
return visits, concerns and complaints, Laboratory Medication by clinicians Room Sedation
patient satisfaction scores, upgrades Circle sizes are proportionate to the respective costs of care (40% lower for patients
from observation to intensive care, the managed with observation). “Inpatient” represents patients hospitalized for ≤1 day.
percentage of patients who decompensate ADAPTED FROM THE JOURNAL OF THE AMERICAN HEART ASSOCIATION
or suffer unexpected complications, and
mortality.4,10,12 extension of acute care. Observation a dedicated emergency department–
Finally, units cannot function properly units are often located where the effects protocolized observation unit does not
without financial stability. Care should of acute treatment can be monitored and preclude the hospital from offering
cost less in dedicated units, which decrease reevaluated, while enabling clinicians to additional hospitalist observation
variability when protocols are used. Even if determine the appropriate disposition for services. This option becomes useful
reimbursements are unprofitable, economic each case.4 for cases that do not meet the criteria
benefits can be gained by increasing The American College of Emergency for inpatient admission but also fall
efficiency and expediting care. Additionally, Physicians supports the use of emergency outside the parameters of protocolized
observing patients who previously had clinicians to staff and manage observation observation care.
prolonged emergency department stays units.14 It is important to specifically When staffing observation units, it
designate these areas as “closed”; ideally, is imperative to select providers who are
can improve throughput and help hospitals
emergency physicians should maintain adaptable, responsible, thorough, and
obtain reimbursement for the additional
authority over observation cases until a willing to learn. For many emergency
care provided.12
final disposition can be determined.4 physicians, working in observation
By tracking average payments by payer
Emergency department observation units medicine is a new role that requires
(eg, Medicare, Medicaid, commercial),
typically offer shorter lengths of stay significant interaction with hospital
emergency departments can gain a better
than those managed by hospitalists, are leadership, consultants, and colleagues.
understanding of the unit’s payer mix and
more cost effective, have fewer patient These clinicians can play a unique role
bottom-line influence. It is key to remember
handoffs, and incur fewer barriers in evaluating patient care and assessing
that the financial success of an observation
when transitioning between acute and emergency department processes. In
unit is dependent on the appropriate
observation care. These benefits are addition, observation physicians who are
selection of patients.
particularly favorable for patients placed welcomed into the fold of an emergency
CRITICAL DECISION in observation, 80% of whom are medicine group can provide constructive
expected to be discharged home within
Who should manage the feedback that helps improve practice
24 hours.9,10,12 patterns and staff performance.
protocolized observation unit? By contrast, hospitalist-run
More than 50% of US observation observation units can provide more Summary
units are managed administratively by continuity of care for those converting to Emergency department observation
emergency departments.13 The rationale for inpatient status, and staff may be more units operate best when they follow a
this arrangement stems from the concept familiar with long-term care coordination closed, protocolized, unit-based model.
that protocolized observation is a natural than those focused on acute care.12 Having Appropriate patient selection is crucial.
July 2019 n Volume 33 Number 7 23
CASE RESOLUTIONS
■ CASE ONE new paroxysmal atrial fibrillation. ■ CASE THREE
The hypertensive man with chest The observation physician discussed The 42-year-old man’s dehydration
pain was determined to have a the case with the emergency
and persistent left flank pain were
HEART score of 4, which indicated department attendings and reviewed
determined to be the result of renal
that he was at moderate risk of the observation unit’s admission
colic and an electrolyte disturbance
having a major adverse cardiac event and protocol exclusion criteria for
attributed to vomiting. The emergency
in the next 6 weeks. Continuous transient ischemic attacks (eg, ongoing
physician transferred him to the
telemetry monitoring was performed neurologic symptoms). The patient met
observation unit, where he received
in the observation unit, which the criteria for inpatient management
IV fluid hydration and antiemetics,
demonstrated no clinically significant and was admitted to the hospitalist
potassium repletion, and a urology
arrhythmia. The patient’s serial service with a neurology consultation.
consultation. Per protocol, analgesics
cardiac enzymes remained negative, The following morning, an MRI
were administered as needed while the
and he continued to be pain-free demonstrated an acute infarction with
no focal stenosis or lesions noted on patient underwent frequent reevalua-
and asymptomatic while undergoing
magnetic resonance angiography of tions. His vomiting subsided with
frequent reevaluation. In consultation
the head and neck. Echocardiography treatment, and his diet was advanced.
with cardiology, he was scheduled to
showed mild mitral regurgitation and Serial laboratory tests revealed
undergo outpatient stress testing the
left ventricular hypertrophy. A plan improvement in his electrolyte levels.
following day. He was discharged
for anticoagulation for the paroxysmal Urology recommended urine
home on daily aspirin therapy after
atrial fibrillation was initiated. straining, oral hydration, and
10 hours of observation care.
Physical and speech therapists outpatient follow-up care. After a
■ CASE TWO evaluated the patient and determined 16-hour stay, the patient was stable
The elderly woman’s symptoms, that she required further rehabilitation enough for discharge and was given
including slurred speech, facial before returning home. She was a prescription for nonsteroidal
numbness, and left leg weakness transferred to subacute rehabilitation analgesics. He provided high
persisted. In addition, she developed on day 3 to continue treatment. satisfaction scores via an online survey.
Well-trained, experienced staff can 3. Exploring the impact of the RAC program on hospitals Alliance (EDOBA): characteristics of high volume
nationwide. American Hospital Association website. teaching hospital observation units. Acad Emerg Med.
effectively monitor patients who require http://www.aha.org/content/16/16q1ractracresults.pdf. 2009;16:S251-S252.
Updated June 2016. Accessed September 28, 2016. 10. American College of Emergency Physicians. State
further treatment and testing or are too 4. Brillman J, Mathers-Dunbar L, Graff L, et al. Management of the Art: Observation Units in the Emergency
of observation units. American College of Emergency
sick to be discharged home. The ideal Physicians. Ann Emerg Med. 1995 Jun;25(6):823-830.
Department. Policy Resource and Education Paper.
Dallas, TX: American College of Emergency Physicians;
observation unit patient has a focused 5. Hospital services covered under Part B. In: Medicare 2011.
Benefit Policy Manual. Centers for Medicare and 11. Mace SE, Graff L, Mikhail M, Ross M. A national survey
problem and defined goal of care that can Medicaid Services website. https://www.cms.gov/ of observation units in the United States. Am J Emerg
Regulations-and-guidance/guidance/manuals/
be met in less than 24 hours. downloads/bp102c06.pdf. Updated December 18, 2015.
Med. 2003 Nov;21(7):529-533.
12. Napolitano JD, Saini I. Observation units: definition,
Emergency department observation Accessed September 28, 2016.
6. Graff LG. Observation Medicine: The Healthcare
history, data, financial considerations, and metrics.
Curr Emerg Hosp Med Rep. 2014 Mar;2(1):1-8.
units should be managed administratively System’s Tincture of Time. Dallas, TX: American College
13. Wiler JL, Ross MA, Ginde AA. National study of
or Emergency Physicians; 2011.
by the emergency department staff, as 7. Baugh CW, Schuur JD. Observation care—high-value emergency department observation services.
care or a cost-shifting loophole? N Engl J Med. 2013 Jul Acad Emerg Med. 2011 Sep;18(9):959-965.
most observation patients are discharged 25;369(4):302-305. 14. Policy statement: emergency department observation
home without requiring inpatient 8. Sheehy AM, Caponi B, Gangireddy S, et al. Observation services. American College of Emergency Physicians
and inpatient status: clinical impact of the 2-midnight website. https://www.acep.org/globalassets/new-
admission. This model helps facilitate rule. J Hosp Med. 2014 Apr;9(4):203-209. pdfs/policy-statements/emergency-department-
9. Annathurai A, Ross MA, Lemos JP, et. al. Data from the observation-services.pdf. Updated October 2015.
department flow and maximize the Emergency Department Observation Unit Benchmark Accessed September 28, 2016.
quality of care provided. An observation
unit’s success is dependent on its ability
to monitor its volume and quality metrics
while providing ongoing medical care.
REFERENCES
1. Baugh CW, Venkatesh AK, Hilton JA, Samuel PA, Schuur
JD, Bohan JS. Making greater use of dedicated hospital n Failing to create thorough, diagnosis-specific protocols.
observation units for many short-stay patients could n Assuming that consultants, primary care physicians, and other hospital staff
save $3.1 billion a year. Health Aff (Millwood). 2012 Oct;
31(10):2314-2323. understand the goals and purpose of observation units.
2. Department of Health and Human Services; n Placing patients into an observation service who either can be safely
Health Care Financing Administration. Section 455:
outpatient observation services. In: Medicare discharged or clearly meet inpatient admission criteria.
Hospital Manual. https://www.cms.gov/Regulations-
and-Guidance/Guidance/Transmittals/downloads/
n Neglecting to clearly delineate the clinical and administrative roles and
R770HO.pdf. Published February 23, 2001. Accessed responsibilities required for managing the observation unit.
September 14, 2016.
24 Critical Decisions in Emergency Medicine
The LLSA Literature Review
Brief Resolved
Unexplained Events
By Andrew Loomis MD, LCDR; and Daphne Morrison Ponce MD, LCDR
Naval Medical Center, Portsmouth, Virginia
Reviewed by Andrew Eyre, MD, MHPEd
Tieder JS, Bonkowsky JL, Etzel RA, et al. Brief resolved unexplained events (formerly apparent life-threatening
events) and evaluation of lower-risk infants: executive summary. Pediatrics. 2016 May;137(5).
Infants frequently present to the emergency department for episodes that trigger parental
concern, even after the initial event has resolved. Before 1986, many of these cases were
attributed to near-miss sudden infant death syndrome (SIDS); in 1986, SIDS was replaced by a
new term: apparent life-threatening event (ALTE). This updated clinical practice guideline by
the American Academy of Pediatrics has two primary objectives. First, it recommends replacing
the term ALTE with a new one: brief resolved unexplained event (BRUE). Second, it provides
guidance for the systematic, risk-based evaluation and management of these cases.
This summary outlines a three-step process diagnosed, and risk stratification CPR was required, the patient should
for the evaluation of a possible BRUE. should proceed. be considered LOW RISK; treatment
1. Is this a BRUE? 2. Is the patient low risk? should proceed according to the following
• Is the patient younger than 1 year? • Is the child older than 60 days? guidelines.
• Is the patient well appearing? • Was the child born at or after 3. When managing low-risk BRUE,
• Did the child present following 32 weeks of gestation, and is the clinicians:
a sudden, brief, resolved event corrected gestational age 45 weeks • SHOULD educate caregivers, provide
that included one or more of the or more? resources for CPR training, and use
• Did the event last less than a shared decision-making approach
following: cyanosis or pallor;
1 minute? regarding the child’s evaluation,
absent, decreased, or irregular
• Is this the first such event? disposition, and follow-up care.
breathing; a marked change in tone
• Are the patient’s history and • MAY offer or consider pertussis
(hyper- or hypotonia); or altered
examination normal (eg, no family testing, obtain an ECG, and provide
responsiveness?
history of sudden cardiac death; brief monitoring (eg, pulse oximetry,
• Is the event unexplained (eg, no serial examinations).
no nondiagnostic social, feeding,
history or symptoms of gastro or respiratory problems)? • SHOULD NOT reflexively initiate
esophageal reflux disease [GERD], If the answer to any question is NO laboratory testing, diagnostic
feeding difficulties, or airway and the child required CPR by a imaging, GERD studies,
abnormalities)? trained medical provider, the case electroencephalography, or home
If the answer to any question is NO, should be considered HIGH RISK. cardiac or respiratory monitoring.
BRUE should be ruled out, and Although these patients require further In addition, there is no need
the patient should undergo further evaluation, there is no evidence to to prescribe GERD or seizure
evaluation. If the answer to all four guide their management. If the answer medications or admit a low-risk
questions is YES, BRUE should be to the above questions is YES and no patient solely for cardiovascular or
respiratory monitoring.
KEY POINTS DISCLOSURES
The views expressed in this article are those of the authors and do
n Children who meet the criteria for BRUE without high-risk features can be not necessarily reflect the official policy or position of the Dept. of
the Navy, Dept. of Defense, or the US Government.
safely discharged without undergoing invasive testing, diagnostic imaging,
We are military service members. This work was prepared as
or inpatient admission. part of our official duties. Title 17 U.S.C. 105 provides that
n There are no formal guidelines regarding the evaluation or disposition of “Copyright protection under this title is not available for any
work of the US Government.” Title 17 U.S.C. 101 defines a
high-risk BRUE cases. US Government work as a work prepared by a military service
n The patient’s parents should be involved in clinical decision making. member or employee of the US Government as part of that
person’s official duties.
Critical Decisions in Emergency Medicine’s series of LLSA reviews features articles from ABEM’s 2019 Lifelong Learning and
Self-Assessment Reading List. Available online at acep.org/moc/llsa and on the ABEM website.
July 2019 n Volume 33 Number 7 25
CME
Reviewed by Lynn Roppolo, MD, FACEP
Qualified, paid subscribers to Critical Decisions in Emergency Medicine may receive
CME certificates for up to 5 ACEP Category I credits, 5 AMA PRA Category 1
Credits™, and 5 AOA Category 2-B credits for completing this activity in its
QUESTIONS entirety. Submit your answers online at acep.org/cdem; a score of 75% or better
is required. You may receive credit for completing the CME activity any time within
3 years of its publication date. Answers to this month’s questions will be published
in next month’s issue.
1 In what pattern does a measles rash typically
spread? 6 Which patient population is at greatest risk for
pertussis-related complications?
A. Extremities to trunk and head A. Children aged 2 to 5 years
B. Head to trunk and extremities B. Children aged 5 to 12 years
C. Trunk to extremities only C. Infants aged 4 months to 1 year
D. Trunk to head and extremities D. Infants younger than 4 months
2 Which measles-related complication can arise
7 to 10 years after the acute illness? 7 The American Academy of Pediatrics recommends
oral antiviral varicella treatment for which group?
A. Myocarditis A. Unvaccinated children older than 12 years
B. Otitis media B. Unvaccinated children younger than 12 years
C. Pneumonia C. Vaccinated children older than 12 years
D. SSPE D. Vaccinated children younger than 12 years
3 A 17-year-old boy presents after his boarding
school roommate is diagnosed with mumps. He
explains that six of his classmates have been
8 A 13-year-old girl presents with a right-sided facial
droop for 1 day. She reports sustaining a minor
laceration to her right cheek 1 week ago, which was
diagnosed with the illness this week. The patient contaminated by horse manure. The patient is noted
previously received one dose of the MMR vaccine. to have right-sided facial weakness, weak closure of
Which post-exposure prophylaxis should be the right eye, and an absence of forehead wrinkling
administered? on the right side. She has no other symptoms, and
A. Immunoglobulin the rest of her physical examination is normal. Which
B. MMR vaccine diagnosis is probable?
C. MMR vaccine and IVIG A. Cephalic tetanus
D. Ribavirin B. Generalized tetanus
C. Localized tetanus
4 A fully vaccinated 17-year-old girl presents after
being exposed to her unvaccinated 14-year-old
D. Splanchnic tetanus
brother, who returned home from a school trip
2 days prior with a varicella rash. She reports that
she is 28 weeks pregnant. Which treatment should
9 Which treatment is an ineffective tetanus
prophylaxis?
A. Antibiotics
be administered as a post-exposure prophylaxis? B. DTaP
A. Acyclovir C. Tdap
B. IVIG D. TIG
C. Varicella vaccine
D. VariZIG
10
What second-line treatment should be administered
to a 4-month-old infant diagnosed with pertussis who
5 While culture is the gold standard, what is the
clinical study of choice for diagnosing pertussis?
is allergic to macrolide antibiotics?
A. Amoxicillin
A. Chest x-rays B. Cefdinir
B. Direct fluorescent antibody testing C. Ciprofloxacin
C. PCR testing D. Trimethoprim-sulfamethoxazole
D. Serology
26 Critical Decisions in Emergency Medicine
11 Which observation model is most efficient?
A. Unit based; closed 17 Which of the following patients is appropriate
for observation care?
B. Unit based; open A. 20-year-old asthmatic with complete symptom
C. Virtual; closed resolution after treatment
D. Virtual; open B. 60-year-old with a brief facial droop and
slurred speech that is now fully resolved
12 What is the approximate length of stay for most
patients who require observation?
pending a neurology consultation, telemetry
monitoring, MRI, and neurological checks
A. 2-4 hours C. 80-year-old with an acute hip fracture pending
B. 6-8 hours surgical repair
C. 12-18 hours D. An admitted patient who has been boarding
D. 24-48 hours in the emergency department due to inpatient
capacity overload
13 What percentage of observation patients can
be managed and discharged without inpatient
admission? 18
What resource should be referenced when
determining if a case warrants inpatient
A. 15% admission?
B. 50% A. CENTOR score
C. 80% B. Medical textbooks
D. 90% C. Milliman Care Guidelines or InterQual Criteria
D. The opinions of the nursing staff
14 Which Medicare program covers observation
services?
A. Part A outpatient services
19 Which approach is most helpful when
developing observation protocols?
B. Part B inpatient services A. Create the protocol autonomously, without
C. Part B outpatient services input from consulting services or hospital
D. Part D outpatient services leadership
B. Include guidelines regarding inclusion/
15 Which of the following is considered a key metric
for tracking observation care?
A. The average emergency department length of stay
exclusion criteria, ideal testing and treatment,
and disposition planning information
C. List all possible testing and treatment options
B. The final disposition of observation patients regardless of evidence
C. The number of 72-hour emergency department D. Write loosely defined guidelines to allow for
returns clinician discretion
D. The percentage of negative cardiac
catheterizations
20
Which of the following most accurately
describes the role of virtual observation?
16 For whom are observation services most
appropriate?
A. Any policy that allows a clinician to place
patients under observation
A. Patients who do not warrant inpatient admission B. Documentation that outlines a patient’s need
but require treatment beyond the scope of the for observation after an insurance denial
emergency department C. The process of interspersing observation
B. Patients who require more than 2 midnights of patients among those on general admission
hospital care floors
C. Patients whose care is completed but whose ride D. Using telemedicine to provide services to
home may be delayed or prolonged observation patients
D. Stroke patients who require skilled nursing or
placement in a rehabilitation facility
ANSWER KEY FOR JUNE 2019, VOLUME 33, NUMBER 6
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20
A C C B A D C A D B D C A A C D D B D D
July 2019 n Volume 33 Number 7 27
zz
Drug Box Tox Box
METHOHEXITAL METHANOL POISONING
By Frank LoVecchio, DO, MPH, FACEP By Christian A. Tomaszewski, MD, MS, MBA, FACEP
Maricopa Medical Center, Phoenix, Arizona University of California, San Diego
Methohexital is a rapid anesthetic that can be used In 2018, more than 150 deaths in India were attributed to the consumption
in the acute setting for procedural sedation. As a of counterfeit liquor that had been laced with methanol. In recent months,
short-acting barbiturate, the drug produces cortical a number of American tourists have died mysteriously in the Dominican
and cerebellar sedation and hypnosis. Republic after drinking from their hotel minibars. Methanol, a substance
often used to extend the life of bootleg liquor, is widely suspected to be
Dose
the culprit. Also known as wood alcohol, methanol is found in carburetor
Adults and children: 1 mg/kg IV, then 0.5 mg/kg cleaner, windshield washer fluid, paint removers, and fracking fluid. The
every 2-5 minutes as needed toxin accounts for approximately 5,000 poisonings in the US every year.
Induction: 50-120 mg (70 mg average) IV push at
10 mg (1 mL of 1% solution) over 5 seconds, Pharmacokinetics
depending on the patient’s response • Potentially toxic dose: 0.1 mL/kg; potentially lethal dose: 1 mL/kg
Pharmacokinetics • Peaks quickly (<1 hour) post ingestion
Half-life: 3-6 hours Mechanism of Action
Onset: Immediate (IV); 2-10 min (IM); 5-15 min (PR) • Methanol is hepatically metabolized to toxic acids.
Duration: 10-20 min (IV); 45 min (PR) • The metabolites formaldehyde and formic acid are toxic.
Metabolism: Hepatically conjugated to inactive Clinical Manifestations (can be delayed by hours)
metabolites; slow • Central nervous system: inebriation (less than with ethanol), headache
Excretion: Urine; trace amounts of drug and/or • Vision: blindness (ie, “snowstorm”)
metabolites also excreted in feces and sweat • Gastrointestinal: vomiting, abdominal pain, pancreatitis
Precautions • Metabolic: anion gap acidosis (formate and lactate)
Rare cases of laryngospasm have been reported. • Kidney: acute kidney injury (AKI)
In such cases, experts recommend administering Diagnostic Tests (if the patient is symptomatic or the ingestion is
an additional dose. intentional)
Contraindications include porphyria (almost never • Basic metabolic panel to screen for acidosis and AKI
a concern in the emergency department) and a • Osmol gap (insensitive)
known hypersensitivity to barbiturates. • Serum methanol level (>10 mg/dL)
Relative contraindications include cardiovascular Treatment and Disposition
disease, hypotension, respiratory disease, • Decontamination is ineffective.
respiratory depression, and hypotension. • Folinic (or folic) acid: 1 mg/kg (up to 50 mg)
Methohexital should be used only when • Fomepizole (15 mg/kg IV) for suspected ingestions in patients with:
continuous monitoring of respiratory (eg, pulse — Methanol level >20 mg/dL
oximetry) and cardiac function can be provided. — Osmol gap >10 mOsm/L
Resuscitative drugs and age- and size-appropriate — Serum bicarbonate <20 mmol/L
equipment for bag-valve-mask ventilation and • Hemodialysis in patients with:
intubation should be readily available as well — Severe refractory acidosis (pH <7.25)
as personnel skilled in airway management. — Methanol >50 mg/dL
Deeply sedated patients should be continuously — Visual complications
monitored by a designated clinician (other than
Disposition
the practitioner performing the procedure).
• Discharge 4-6 hours after ingestion if bicarbonate and osmol gap levels
Pregnancy Category B are normal. Admit if antidotal therapy or hemodialysis is required.
You might also like
- Cdem 19december WebDocument32 pagesCdem 19december WebRicardo Jonathan Ayala GarciaNo ratings yet
- Cdem 18august WebDocument32 pagesCdem 18august WebRicardo Jonathan Ayala GarciaNo ratings yet
- CDEM 18september WEBDocument28 pagesCDEM 18september WEBRicardo Jonathan Ayala GarciaNo ratings yet
- Cdem 20january WebDocument28 pagesCdem 20january WebRicardo Jonathan Ayala GarciaNo ratings yet
- Cdem 19may WebDocument32 pagesCdem 19may WebRicardo Jonathan Ayala GarciaNo ratings yet
- Cdem 19august WebDocument32 pagesCdem 19august WebRicardo Jonathan Ayala GarciaNo ratings yet
- Cdem 18june WebDocument32 pagesCdem 18june WebRicardo Jonathan Ayala GarciaNo ratings yet
- Cdem 18december WebDocument28 pagesCdem 18december WebRicardo Jonathan Ayala GarciaNo ratings yet
- Cdem 19june WebDocument28 pagesCdem 19june WebRicardo Jonathan Ayala GarciaNo ratings yet
- Cdem 19april WebDocument28 pagesCdem 19april WebRicardo Jonathan Ayala GarciaNo ratings yet
- CDEM 19september WEBDocument32 pagesCDEM 19september WEBRicardo Jonathan Ayala GarciaNo ratings yet
- Cdem 17march WebDocument24 pagesCdem 17march WebRicardo Jonathan Ayala GarciaNo ratings yet
- Cdem 16october Final (Web)Document28 pagesCdem 16october Final (Web)Ricardo Jonathan Ayala GarciaNo ratings yet
- CDEM 17oct WebDocument24 pagesCDEM 17oct WebRicardo Jonathan Ayala GarciaNo ratings yet
- CDEM 17sept CompleteDocument24 pagesCDEM 17sept CompleteRicardo Jonathan Ayala GarciaNo ratings yet
- CDEM 17jan Complete WEBDocument24 pagesCDEM 17jan Complete WEBRicardo Jonathan Ayala GarciaNo ratings yet
- CDEM 16december WebDocument24 pagesCDEM 16december WebRicardo Jonathan Ayala GarciaNo ratings yet
- CDEM 17august (Web)Document28 pagesCDEM 17august (Web)Ricardo Jonathan Ayala GarciaNo ratings yet
- Cdem 18feb WebDocument32 pagesCdem 18feb WebRicardo Jonathan Ayala GarciaNo ratings yet
- CDEM 17december WebDocument24 pagesCDEM 17december WebRicardo Jonathan Ayala GarciaNo ratings yet
- CDEM 18march WebDocument28 pagesCDEM 18march WebRicardo Jonathan Ayala GarciaNo ratings yet
- CDEM 18january WebDocument24 pagesCDEM 18january WebRicardo Jonathan Ayala GarciaNo ratings yet
- CDEM TraumaEdition WebDocument63 pagesCDEM TraumaEdition WebRicardo Jonathan Ayala GarciaNo ratings yet
- Pediatric Special Edition: Inside This IssueDocument79 pagesPediatric Special Edition: Inside This IssueRicardo Jonathan Ayala GarciaNo ratings yet
- Cdem 23june WebDocument32 pagesCdem 23june WebgomsuiNo ratings yet
- Guia Sindrome Ovario PoliquisticoDocument56 pagesGuia Sindrome Ovario Poliquisticopalomazul007No ratings yet
- Medical Student Educators HandbookDocument324 pagesMedical Student Educators HandbookRodrigo SanjinesNo ratings yet
- Download Neonatal Cardiology 3Rd Edition Michael Artman full chapterDocument67 pagesDownload Neonatal Cardiology 3Rd Edition Michael Artman full chapterjonathan.smith167100% (7)
- (Medical Radiology) Jonathan Strauss, William Small JR., Gayle E. Woloschak - Breast Cancer Biology For The Radiation Oncologist-Springer (2015)Document94 pages(Medical Radiology) Jonathan Strauss, William Small JR., Gayle E. Woloschak - Breast Cancer Biology For The Radiation Oncologist-Springer (2015)Piotr JankowskiNo ratings yet
- DNP Last-Manuscript Revision 6-26-2022Document72 pagesDNP Last-Manuscript Revision 6-26-2022api-577866488No ratings yet
- Hospital Medicine To CDocument12 pagesHospital Medicine To Ccloudman81No ratings yet
- Handbook 2019-2020Document24 pagesHandbook 2019-2020api-510203643No ratings yet
- Efficacy of PERT Care: Evidence: Yevgeniy Brailovsky, Vladimir Lakhter, Amir Darki, and Geoffrey D. BarnesDocument29 pagesEfficacy of PERT Care: Evidence: Yevgeniy Brailovsky, Vladimir Lakhter, Amir Darki, and Geoffrey D. Barnesnappi.teresaNo ratings yet
- Reference Range Values For Pediatric Care-2nd PDFDocument202 pagesReference Range Values For Pediatric Care-2nd PDFIvan Veriswan67% (3)
- Stem Capstone PaperDocument17 pagesStem Capstone Paperapi-484250989No ratings yet
- Anemia Prevention and Management Program Implementation GuideDocument60 pagesAnemia Prevention and Management Program Implementation GuideIchlasul MadriddistaNo ratings yet
- Pedsap 1 ImmunologyDocument96 pagesPedsap 1 ImmunologyNeha Oberoi100% (1)
- Full download book Surgery Pretest Self Assessment And Review 14E Pdf pdfDocument41 pagesFull download book Surgery Pretest Self Assessment And Review 14E Pdf pdfemilio.elliott723100% (14)
- Conceps in Clinical Pharmacokinetics PDFDocument294 pagesConceps in Clinical Pharmacokinetics PDFCareyTran100% (4)
- Japanese Encephalitis Vaccines: Morbidity and Mortality Weekly ReportDocument32 pagesJapanese Encephalitis Vaccines: Morbidity and Mortality Weekly Reportferi rambeNo ratings yet
- Download ebook Pharmacotherapy Casa Patient Focused Approach Eleventh Edition Pdf full chapter pdfDocument67 pagesDownload ebook Pharmacotherapy Casa Patient Focused Approach Eleventh Edition Pdf full chapter pdfmerlin.mitchell336100% (25)
- Jayson-Cagadas-Pasaol 1704101 Philippines ThesisDocument96 pagesJayson-Cagadas-Pasaol 1704101 Philippines ThesisIzel Monica Osorio BollonNo ratings yet
- ACS TQIP Palliative Care Best Practices GuidelinesDocument56 pagesACS TQIP Palliative Care Best Practices GuidelinesAgamdarya HembramNo ratings yet
- K-Medical Staffing: A Business PlanDocument57 pagesK-Medical Staffing: A Business PlanPrabha GuptaNo ratings yet
- Avoiding Common Errors in The Emergency Department-1-280Document280 pagesAvoiding Common Errors in The Emergency Department-1-280Hernando Castrillón0% (1)
- Human Papillomavirus (HPV) Infection and Vaccine Knowledge and atDocument72 pagesHuman Papillomavirus (HPV) Infection and Vaccine Knowledge and atHimanshu ShahNo ratings yet
- Pharmacotherapy Casa Patient Focused Approach Eleventh Edition Terry L Schwinghammer download pdf chapterDocument51 pagesPharmacotherapy Casa Patient Focused Approach Eleventh Edition Terry L Schwinghammer download pdf chaptergloria.lovins597100% (4)
- SMITH, T. J. SAIKI, C. B. Cancer Pain Management. Symposium On Pain Medicine. Mayo Clin Proc, v. 90, P. 1428-1439, 2015.Document12 pagesSMITH, T. J. SAIKI, C. B. Cancer Pain Management. Symposium On Pain Medicine. Mayo Clin Proc, v. 90, P. 1428-1439, 2015.Fran WermannNo ratings yet
- Caregiver PDFDocument15 pagesCaregiver PDFNurul ShahirahNo ratings yet
- Download Case Files Family Medicine 5E Nov 6 2020_1260468593_Mcgraw Hill Eugene C Toy full chapterDocument67 pagesDownload Case Files Family Medicine 5E Nov 6 2020_1260468593_Mcgraw Hill Eugene C Toy full chaptermarion.wade943100% (3)
- Atlas de Patología de Los MaxilaresDocument28 pagesAtlas de Patología de Los MaxilaresLuis H. NarváezNo ratings yet
- 2014 ART National Summary Report Highlights Key FindingsDocument78 pages2014 ART National Summary Report Highlights Key Findingsmeltwithsnow163.comNo ratings yet
- Download Schwartzs Principles Of Surgery 11Th Edition F Charles Brunicardi all chapterDocument67 pagesDownload Schwartzs Principles Of Surgery 11Th Edition F Charles Brunicardi all chapterroy.nogle598100% (7)
- ACIP Recommendations for Use of Ebola Vaccine in the U.SDocument16 pagesACIP Recommendations for Use of Ebola Vaccine in the U.SworksheetbookNo ratings yet
- Clinical PKDocument296 pagesClinical PKodimuthuNo ratings yet
- SCCM Clinical - Practice - Guideline Safe Medication Use in ICUDocument6 pagesSCCM Clinical - Practice - Guideline Safe Medication Use in ICULuciana OliveiraNo ratings yet
- Download Schwartzs Principles Of Surgery 11Th Edition Volume 1 F Charles Brunicardi all chapterDocument67 pagesDownload Schwartzs Principles Of Surgery 11Th Edition Volume 1 F Charles Brunicardi all chapterroy.nogle598100% (7)
- Emra Medical Student Survival Guide 2edDocument288 pagesEmra Medical Student Survival Guide 2edtamikanji50% (2)
- Pediatric Special Edition: Inside This IssueDocument79 pagesPediatric Special Edition: Inside This IssueRicardo Jonathan Ayala GarciaNo ratings yet
- CDEM TraumaEdition WebDocument63 pagesCDEM TraumaEdition WebRicardo Jonathan Ayala GarciaNo ratings yet
- Cdem 19march WebDocument28 pagesCdem 19march WebRicardo Jonathan Ayala GarciaNo ratings yet
- Cdem 19october WebDocument24 pagesCdem 19october WebRicardo Jonathan Ayala GarciaNo ratings yet
- Cdem 19february WebDocument28 pagesCdem 19february WebRicardo Jonathan Ayala GarciaNo ratings yet
- CDEM 19september WEBDocument32 pagesCDEM 19september WEBRicardo Jonathan Ayala GarciaNo ratings yet
- Cdem 19november WebDocument28 pagesCdem 19november WebRicardo Jonathan Ayala GarciaNo ratings yet
- Cdem 19august WebDocument32 pagesCdem 19august WebRicardo Jonathan Ayala GarciaNo ratings yet
- Cdem 18feb WebDocument32 pagesCdem 18feb WebRicardo Jonathan Ayala GarciaNo ratings yet
- Cdem 19april WebDocument28 pagesCdem 19april WebRicardo Jonathan Ayala GarciaNo ratings yet
- Cdem 19june WebDocument28 pagesCdem 19june WebRicardo Jonathan Ayala GarciaNo ratings yet
- Cdem 19january WebDocument28 pagesCdem 19january WebRicardo Jonathan Ayala GarciaNo ratings yet
- Cdem 18may WebDocument32 pagesCdem 18may WebRicardo Jonathan Ayala GarciaNo ratings yet
- CDEM 18january WebDocument24 pagesCDEM 18january WebRicardo Jonathan Ayala GarciaNo ratings yet
- CDEM 18march WebDocument28 pagesCDEM 18march WebRicardo Jonathan Ayala GarciaNo ratings yet
- Cdem 18november WebDocument28 pagesCdem 18november WebRicardo Jonathan Ayala GarciaNo ratings yet
- CDEM 17sept CompleteDocument24 pagesCDEM 17sept CompleteRicardo Jonathan Ayala GarciaNo ratings yet
- Cdem 18december WebDocument28 pagesCdem 18december WebRicardo Jonathan Ayala GarciaNo ratings yet
- Cdem 18july WebDocument28 pagesCdem 18july WebRicardo Jonathan Ayala GarciaNo ratings yet
- Cdem 18october WebDocument24 pagesCdem 18october WebRicardo Jonathan Ayala Garcia100% (1)
- CDEM 17oct WebDocument24 pagesCDEM 17oct WebRicardo Jonathan Ayala GarciaNo ratings yet
- CDEM 17nov Complete WebDocument24 pagesCDEM 17nov Complete WebRicardo Jonathan Ayala GarciaNo ratings yet
- Cdem 17march WebDocument24 pagesCdem 17march WebRicardo Jonathan Ayala GarciaNo ratings yet
- CDEM 18april WebDocument28 pagesCDEM 18april WebRicardo Jonathan Ayala GarciaNo ratings yet
- Data Sheet Dump ValveDocument2 pagesData Sheet Dump ValveVlade NaumovskiNo ratings yet
- Mesfin A. Agri. Econ. - 2005Document129 pagesMesfin A. Agri. Econ. - 2005Rafez JoneNo ratings yet
- Corticosteroid: Saut Samuel Simamora Department Ophthalmology Diponegoro University-Kariadi HospitalDocument21 pagesCorticosteroid: Saut Samuel Simamora Department Ophthalmology Diponegoro University-Kariadi HospitalSania NadianisaNo ratings yet
- May 4-22 Culinary 1 Lesson Plans PDFDocument4 pagesMay 4-22 Culinary 1 Lesson Plans PDFesefsdfsfNo ratings yet
- Music and Therapy Bun2Document17 pagesMusic and Therapy Bun2PanteaAlisaNo ratings yet
- Asia Pacific College of Advanced StudiesDocument4 pagesAsia Pacific College of Advanced StudiesRussel QuinonesNo ratings yet
- IRC Girl Shine Part 4 DigitalDocument124 pagesIRC Girl Shine Part 4 DigitalMónica SalesNo ratings yet
- Mill Housings Mangal SinghDocument5 pagesMill Housings Mangal SinghGun SmithNo ratings yet
- D 1123 - 99 Rdexmjmtotk - PDFDocument5 pagesD 1123 - 99 Rdexmjmtotk - PDFFrancisco GuerraNo ratings yet
- Indian Pharmacopiea 2007Document73 pagesIndian Pharmacopiea 2007Deepak ShahNo ratings yet
- Manoshe Street Takeaway MenuDocument9 pagesManoshe Street Takeaway MenuimaddakrNo ratings yet
- Counter-pressure filler valve for beveragesDocument3 pagesCounter-pressure filler valve for beveragesbimalishaNo ratings yet
- Queuing System Optimization for Mercury Drug StoreDocument17 pagesQueuing System Optimization for Mercury Drug StoreAllen Agno llNo ratings yet
- Role of Drugs That Affect Renin Angiotensin SystemDocument22 pagesRole of Drugs That Affect Renin Angiotensin Systemash ashNo ratings yet
- 2020 End Year 6 PenulisanDocument8 pages2020 End Year 6 PenulisanZulhillmi ZainuddinNo ratings yet
- D754te3 VMDocument37 pagesD754te3 VMGurpreet SinghNo ratings yet
- Herbal MedicineDocument38 pagesHerbal MedicineBurei KouNo ratings yet
- How To Judge A Dasha in JyotishDocument2 pagesHow To Judge A Dasha in JyotishRavan SharmaNo ratings yet
- Development Team: Analytical Chemistry PolarographyDocument18 pagesDevelopment Team: Analytical Chemistry PolarographyKanchanNo ratings yet
- Fosfomycin: Review and Use Criteria BackgroundDocument12 pagesFosfomycin: Review and Use Criteria BackgroundAbu Azzam Al-Hadi100% (1)
- Dahong PalayDocument2 pagesDahong PalayAngela MontenegroNo ratings yet
- PackageCare Maintenance ChecklistDocument1 pagePackageCare Maintenance ChecklistBùi ViệtNo ratings yet
- Shandong Lingong Wheel Loader LG956l Operation & Maintenance Manual Final 10.3.23Document130 pagesShandong Lingong Wheel Loader LG956l Operation & Maintenance Manual Final 10.3.23mliugong94% (16)
- NCERT Class 6 Geography Chapter 1 YouTube Lecture HandoutsDocument5 pagesNCERT Class 6 Geography Chapter 1 YouTube Lecture Handoutskalasri100% (1)
- Winged Scapula Caused by Dorsal Scapular.21Document4 pagesWinged Scapula Caused by Dorsal Scapular.21emilio9fernandez9gatNo ratings yet
- STC Bec Wir Plu D 0209 01 PDFDocument10 pagesSTC Bec Wir Plu D 0209 01 PDFAdel MorsyNo ratings yet
- Johnson Et Al.2006. Felidae PhylogenyDocument6 pagesJohnson Et Al.2006. Felidae Phylogenyaspergillus_jallNo ratings yet
- OTC Drug ListDocument7 pagesOTC Drug ListHong Diem100% (1)
- An Experimental Study of AcidizingDocument11 pagesAn Experimental Study of Acidizinggigi17No ratings yet
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (17)
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 4 out of 5 stars4/5 (3)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (78)
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 4 out of 5 stars4/5 (5)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsFrom EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo ratings yet
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (403)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisFrom EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisRating: 4.5 out of 5 stars4.5/5 (42)
- 12 Rules for Life by Jordan B. Peterson - Book Summary: An Antidote to ChaosFrom Everand12 Rules for Life by Jordan B. Peterson - Book Summary: An Antidote to ChaosRating: 4.5 out of 5 stars4.5/5 (207)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsRating: 5 out of 5 stars5/5 (1)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeNo ratings yet
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 3.5 out of 5 stars3.5/5 (3)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsFrom EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsRating: 4.5 out of 5 stars4.5/5 (169)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaFrom EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaRating: 4.5 out of 5 stars4.5/5 (266)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryFrom EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryRating: 4 out of 5 stars4/5 (44)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessFrom EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessRating: 4.5 out of 5 stars4.5/5 (328)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.From EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Rating: 4.5 out of 5 stars4.5/5 (110)
- The Happiness Trap: How to Stop Struggling and Start LivingFrom EverandThe Happiness Trap: How to Stop Struggling and Start LivingRating: 4 out of 5 stars4/5 (1)
- Algorithms to Live By: The Computer Science of Human DecisionsFrom EverandAlgorithms to Live By: The Computer Science of Human DecisionsRating: 4.5 out of 5 stars4.5/5 (722)
- Summary: How to Be an Adult in Relationships: The Five Keys to Mindful Loving by David Richo: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: How to Be an Adult in Relationships: The Five Keys to Mindful Loving by David Richo: Key Takeaways, Summary & Analysis IncludedRating: 4 out of 5 stars4/5 (11)
- Gut: the new and revised Sunday Times bestsellerFrom EverandGut: the new and revised Sunday Times bestsellerRating: 4 out of 5 stars4/5 (392)
- When the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisFrom EverandWhen the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisRating: 3.5 out of 5 stars3.5/5 (2)
- Secure Love: Create a Relationship That Lasts a LifetimeFrom EverandSecure Love: Create a Relationship That Lasts a LifetimeRating: 5 out of 5 stars5/5 (18)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisFrom EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (1)