You might also like
- CS AlgorithmDocument1 pageCS AlgorithmDraalexNo ratings yet
- Neonatal Sepsis Algorithm2Document1 pageNeonatal Sepsis Algorithm2CHIERBEENo ratings yet
- Waqas Ahmed Usmani ROLL NO 17-78Document41 pagesWaqas Ahmed Usmani ROLL NO 17-78Waqas Ahmed UsmaniNo ratings yet
- F Psuneo NasDocument1 pageF Psuneo Nasalvin septianoNo ratings yet
- Assessment of A Pregnant FamilyDocument4 pagesAssessment of A Pregnant FamilyLuna Sang-anNo ratings yet
- Case Study in ObwardDocument6 pagesCase Study in Obwardcharles_florendo25100% (3)
- Diabetes in PregnancyDocument1 pageDiabetes in Pregnancycatcat669111No ratings yet
- Eposter Infants of Mothers With Syphilis Glabela CPDocument1 pageEposter Infants of Mothers With Syphilis Glabela CPGlabela Christiana PandangoNo ratings yet
- Pediatric Bacterial Meningitis Case PresentationDocument22 pagesPediatric Bacterial Meningitis Case Presentationapi-602288180No ratings yet
- Postterm PregnancyDocument2 pagesPostterm PregnancyicNo ratings yet
- Duty Report RIWDocument41 pagesDuty Report RIWRiyan W. PratamaNo ratings yet
- Cleft Lip or PalateDocument19 pagesCleft Lip or PalateAnonymous LCLG7siTYnNo ratings yet
- Fetal MonitoringDocument6 pagesFetal MonitoringRraouzmaaliNo ratings yet
- Finals - MCN RLEDocument6 pagesFinals - MCN RLEKorean GirlNo ratings yet
- Post Term PregnancyDocument12 pagesPost Term PregnancyRizky Putra Ismeldi100% (1)
- Neonatal Jaundice PathwayDocument35 pagesNeonatal Jaundice Pathwaypragita ayu100% (1)
- Acute Abnormal Uterine Bleeding (Aub) : AlgorithmDocument8 pagesAcute Abnormal Uterine Bleeding (Aub) : AlgorithmPhiyaNo ratings yet
- 84 - UTI Ed and Uc Culture Results Decision TreeDocument1 page84 - UTI Ed and Uc Culture Results Decision TreeShimelis TadesseNo ratings yet
- CHN FinalsDocument15 pagesCHN FinalsLuna sibilityNo ratings yet
- Heartworm Disease: What To Do With Your SNAP ResultDocument1 pageHeartworm Disease: What To Do With Your SNAP ResultIantela AlexNo ratings yet
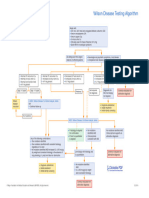
- Wilson Disease Testing AlgorithmDocument1 pageWilson Disease Testing Algorithmbassam alharaziNo ratings yet
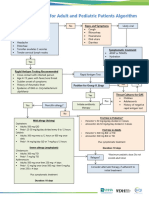
- Outpatient Acute Pharyngitis For Adults and Pediatric Patients Algorithm - FinalDocument1 pageOutpatient Acute Pharyngitis For Adults and Pediatric Patients Algorithm - Finaljmor.3009No ratings yet
- Women's HealthDocument44 pagesWomen's HealthKylie ElaineNo ratings yet
- Acute Abdominal Pain Pathway: Management - Primary Care and Community SettingsDocument2 pagesAcute Abdominal Pain Pathway: Management - Primary Care and Community Settingsshella1selinaNo ratings yet
- CPG CroupDocument4 pagesCPG CroupMarvin M PulaoNo ratings yet
- ImmunoSeroLab M4Document3 pagesImmunoSeroLab M4ela kikayNo ratings yet
- ch2 fs1Document2 pagesch2 fs1ry beNo ratings yet
- Management of Normal LaborDocument98 pagesManagement of Normal LaborGoogle SecurityNo ratings yet
- 2nd Preceptorials FinalDocument14 pages2nd Preceptorials FinalGabriel MillaNo ratings yet
- $RQMTW24Document1 page$RQMTW24akxerox47No ratings yet
- F Seizures AssessDocument1 pageF Seizures Assessmahmudajannatul.7No ratings yet
- Pulmonary EmbolismDocument23 pagesPulmonary EmbolismAkhilesh TiwariNo ratings yet
- Obstetrics PDFDocument14 pagesObstetrics PDFKatheryn100% (1)
- Acute Low Back Pain Flowchart January 2017Document1 pageAcute Low Back Pain Flowchart January 20171234chocoNo ratings yet
- Induction of Labour: Maternity and Neonatal Clinical GuidelineDocument30 pagesInduction of Labour: Maternity and Neonatal Clinical GuidelineFino GunnersNo ratings yet
- Bahan Tugas Tokolitik Ulfadiya Putri 1Document25 pagesBahan Tugas Tokolitik Ulfadiya Putri 1hopa shopNo ratings yet
- Syphilis Screening Testing and TreatmentDocument2 pagesSyphilis Screening Testing and TreatmentMoeed Iqbal100% (1)
- Late Preterm Early Term EOS - Neonatal ManualDocument2 pagesLate Preterm Early Term EOS - Neonatal ManualsumantamohammedNo ratings yet
- Care During 1st Stage of LabourDocument27 pagesCare During 1st Stage of LabourCHARLOTTE DU PREEZNo ratings yet
- PQCNC ASNS Learning Session - DataDocument28 pagesPQCNC ASNS Learning Session - DatakcochranNo ratings yet
- Evaluation and Diagnosis: New York State Department of HealthDocument2 pagesEvaluation and Diagnosis: New York State Department of HealthNisa Annisa ArfiyantiNo ratings yet
- This Study Resource Was Shared Via: Template: SBAR - Postpartum Care SDocument2 pagesThis Study Resource Was Shared Via: Template: SBAR - Postpartum Care SAira Leigh MoralesNo ratings yet
- PromDocument1 pagePromwedishaNo ratings yet
- NCP - Placenta PreviaDocument3 pagesNCP - Placenta PreviaJulianna Alex ConopioNo ratings yet
- Perinatal SbarDocument1 pagePerinatal SbarGlendy DelrioNo ratings yet
- Cesarean Section Audit FormatDocument6 pagesCesarean Section Audit FormatRahul JalauniaNo ratings yet
- Non-Modifiable Risk Factors: Modifiable Risk Factors: EtiologyDocument1 pageNon-Modifiable Risk Factors: Modifiable Risk Factors: EtiologyDenise FranciscoNo ratings yet
- PaedsDocument72 pagesPaedsOlivia Genevieve El JassarNo ratings yet
- Righ Choise TrialDocument17 pagesRigh Choise TrialOscar FloresNo ratings yet
- Pedia NCPDocument8 pagesPedia NCPFrancheska Nicole Delos SantosNo ratings yet
- Neurodevelopmental Assessments For Prediction of Cerebral Palsy - From Brazelton, Hine To General Movements: The EvidenceDocument39 pagesNeurodevelopmental Assessments For Prediction of Cerebral Palsy - From Brazelton, Hine To General Movements: The Evidencekawaljit000No ratings yet
- MODULE 2.3 Antepartum - Pregnancy Module NURSING NOTESDocument11 pagesMODULE 2.3 Antepartum - Pregnancy Module NURSING NOTESQwer TyNo ratings yet
- G JaundiceDocument40 pagesG JaundiceRedina Tuya RamirezNo ratings yet
- Gynae SNI Final Print VersionDocument34 pagesGynae SNI Final Print VersionMr Soman Nadim IqbalNo ratings yet
- G NewexamDocument25 pagesG NewexamvineelainjetyNo ratings yet
- What You Should Know Before The PnleDocument6 pagesWhat You Should Know Before The PnleNicole OrtegaNo ratings yet
- Management of Covid HRPB - 22 March 2020Document1 pageManagement of Covid HRPB - 22 March 2020Kok Hui DiongNo ratings yet
- Newborn AssessmentDocument3 pagesNewborn AssessmentMimie CaliNo ratings yet
- Prenatal Chromosomal Microarray Nov2015-3Document34 pagesPrenatal Chromosomal Microarray Nov2015-3suryasivNo ratings yet
- 5 Facts You Should Know About The Green MarchDocument7 pages5 Facts You Should Know About The Green MarchDriss Baouche100% (1)
- Annual 2005Document128 pagesAnnual 2005KarredeLeonNo ratings yet
- Doanh Nghiep Viet Nam Quang CaoDocument1 pageDoanh Nghiep Viet Nam Quang Caodoanhnghiep100% (1)
- Effects of Monetory PolicyDocument5 pagesEffects of Monetory PolicyMoniya SinghNo ratings yet
- Out To Lunch: © This Worksheet Is FromDocument1 pageOut To Lunch: © This Worksheet Is FromResian Garalde BiscoNo ratings yet
- Kumpulan Soal UPDocument16 pagesKumpulan Soal UPTriono SusantoNo ratings yet
- MSPM Clark UniversityDocument27 pagesMSPM Clark Universitytushar gargNo ratings yet
- Manual GPS Trimble Portugues CFX-750 / FM-750Document246 pagesManual GPS Trimble Portugues CFX-750 / FM-750José Luis Mailkut Pires100% (5)
- Theories of EmotionDocument11 pagesTheories of EmotionNoman ANo ratings yet
- Data Communication and Networks Syllabus PDFDocument2 pagesData Communication and Networks Syllabus PDFgearlaluNo ratings yet
- Emilio Aguinaldo: The First Philippine Republic The Malolos CongressDocument3 pagesEmilio Aguinaldo: The First Philippine Republic The Malolos CongressLIEZLE ANN EROYNo ratings yet
- Rationale of Labour Welfare To Employers and EmployeesDocument20 pagesRationale of Labour Welfare To Employers and Employeesajit yadav100% (1)
- Lesson Plan Design: Ccss - Ela-Literacy - Rf.2.3Document6 pagesLesson Plan Design: Ccss - Ela-Literacy - Rf.2.3api-323520361No ratings yet
- Week 1Document34 pagesWeek 1Mitchie Faustino100% (1)
- Friday Night Mishaps, Listening Plus TasksDocument3 pagesFriday Night Mishaps, Listening Plus TasksCristina Stoian100% (1)
- QinQ Configuration PDFDocument76 pagesQinQ Configuration PDF_kochalo_100% (1)
- Short Question: Computer Science For 9 Class (Unit # 3)Document5 pagesShort Question: Computer Science For 9 Class (Unit # 3)Yasir MehmoodNo ratings yet
- We Don't Need No MBADocument9 pagesWe Don't Need No MBAsharad_khandelwal_2No ratings yet
- Brochure For New HiresDocument11 pagesBrochure For New HiresroseNo ratings yet
- Canada Immigration Forms: E33106Document6 pagesCanada Immigration Forms: E33106Oleksiy Kovyrin100% (1)
- The Board-Management RelationshipDocument32 pagesThe Board-Management RelationshipAlisha SthapitNo ratings yet
- Karbohidrat: Gula, Pati & SeratDocument20 pagesKarbohidrat: Gula, Pati & SeratAlfi Syahrin SiregarNo ratings yet
- List of Mines in IndiaDocument4 pagesList of Mines in IndiaNAMISH MAHAKULNo ratings yet
- HOPE 2A MODULE 1 Introduction To SportsDocument11 pagesHOPE 2A MODULE 1 Introduction To SportsChristian Ray Lucnagan ReyesNo ratings yet
- Kuis 4Document10 pagesKuis 4Deri AntoNo ratings yet
- Machine Tools Design: InstructorsDocument31 pagesMachine Tools Design: InstructorsAladdin AdelNo ratings yet
- All This Comand Use To Type in NotepadDocument9 pagesAll This Comand Use To Type in NotepadBiloul ShirazNo ratings yet
- Broken Squares - Unfreezing Team Building ExerciseDocument4 pagesBroken Squares - Unfreezing Team Building Exerciselilywhite786No ratings yet
- Coles Stategic AssessmentDocument10 pagesColes Stategic AssessmentRichardNo ratings yet
- How To Perform A Financial Institution Risk Assessment: Quick Reference GuideDocument15 pagesHow To Perform A Financial Institution Risk Assessment: Quick Reference GuideYasmeen AbdelAleemNo ratings yet