You might also like
- Ats Waveform Slideshow v5MACDocument72 pagesAts Waveform Slideshow v5MACSaumil100% (1)
- Ermhs Assessment Template - SelpaDocument8 pagesErmhs Assessment Template - Selpaapi-41786760350% (2)
- List of Herbs and PropertiesDocument21 pagesList of Herbs and PropertieswisnuNo ratings yet
- Complete Guide To Physical ExamDocument19 pagesComplete Guide To Physical ExamSeff Causapin100% (2)
- Nur1 230 Fundamentals of Canadian NursingDocument1,666 pagesNur1 230 Fundamentals of Canadian NursingSamantha Lau100% (4)
- First Principles of Gastroenterology and HepatologyDocument826 pagesFirst Principles of Gastroenterology and HepatologyDiana Iordache100% (1)
- CVS Heart MurmursDocument2 pagesCVS Heart MurmursIamTineshNo ratings yet
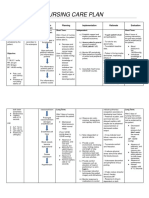
- Nursing Care Plan For Ineffective Airway ClearanceDocument7 pagesNursing Care Plan For Ineffective Airway Clearancearlee marquez96% (117)
- Anatomy Revision Slides PDFDocument133 pagesAnatomy Revision Slides PDFAbhijit0% (1)
- Blood Pressure Regulation MechanismsDocument68 pagesBlood Pressure Regulation MechanismsPhysiology by Dr RaghuveerNo ratings yet
- Nelson MCQ PDFDocument595 pagesNelson MCQ PDFPavan Kumar100% (5)
- Three Approaches To Psychotherapy GloriaDocument41 pagesThree Approaches To Psychotherapy GloriaLuisa Hernandezy67% (3)
- Nursing Care Plan For HELLP SyndromeDocument17 pagesNursing Care Plan For HELLP SyndromeRosemarie Carpio75% (4)
- Hypertension Concept MapDocument1 pageHypertension Concept Mapashleydean100% (7)
- GP33 Manual ClsiDocument3 pagesGP33 Manual ClsiGonzalez ArturoNo ratings yet
- Chapter 1 - Cellular Injury, Cell Adaptation & Cell Death (Robbins and Cotran Pathologic Basis of Disease)Document3 pagesChapter 1 - Cellular Injury, Cell Adaptation & Cell Death (Robbins and Cotran Pathologic Basis of Disease)Ernie G. Bautista II, RN, MD91% (34)
- Sheet - Respiratory ExaminationDocument11 pagesSheet - Respiratory ExaminationbakesamiNo ratings yet
- Physical Diagnosis of The ThoraxDocument3 pagesPhysical Diagnosis of The ThoraxSeff Causapin100% (1)
- Chapter 8 Infectious Diseases Robbins and Cotran Pathologic Basis of Disease PDFDocument12 pagesChapter 8 Infectious Diseases Robbins and Cotran Pathologic Basis of Disease PDFRitz Celso100% (1)
- Chapter 8 Infectious Diseases Robbins and Cotran Pathologic Basis of Disease PDFDocument12 pagesChapter 8 Infectious Diseases Robbins and Cotran Pathologic Basis of Disease PDFRitz Celso100% (1)
- Congenital Heart DiseasesDocument1 pageCongenital Heart DiseasesEmily AnnNo ratings yet
- Advanced Trauma Life SupportDocument8 pagesAdvanced Trauma Life SupportAbouzr Mohammed ElsaidNo ratings yet
- Advanced Trauma Life Support RevisedDocument7 pagesAdvanced Trauma Life Support RevisedpaveethrahNo ratings yet
- ATLSDocument29 pagesATLSmasriemarshalyNo ratings yet
- Biology 3Document1 pageBiology 3KacperCoghenNo ratings yet
- 00063Document3 pages00063Nica Lopez FernandezNo ratings yet
- Kami Export - Cardiovascular System Lecture Outline 1st PeriodDocument16 pagesKami Export - Cardiovascular System Lecture Outline 1st PeriodJada NovakNo ratings yet
- Managing Shortness of Breath in Rheumatic Heart DiseaseDocument3 pagesManaging Shortness of Breath in Rheumatic Heart DiseaseGail NamangdanNo ratings yet
- Pneumothorax Key PointsDocument2 pagesPneumothorax Key PointsJose UringNo ratings yet
- Evaluate PDFDocument3 pagesEvaluate PDFMc SantosNo ratings yet
- PleurallungdiseasesDocument1 pagePleurallungdiseasesCaroNo ratings yet
- Heart Lung InteractionDocument39 pagesHeart Lung InteractionziadNo ratings yet
- EAC BASIC Respiratory Pharmacology DrugsDocument130 pagesEAC BASIC Respiratory Pharmacology DrugsMARK RYAN HERNANDEZNo ratings yet
- Respiring processes and lung diseasesDocument20 pagesRespiring processes and lung diseasesAisyah AlviNo ratings yet
- 10 Respiratory System 2Document73 pages10 Respiratory System 2Angel BumanglagNo ratings yet
- 6.6 CardiovascularDocument9 pages6.6 CardiovascularGhianx Carlox PioquintoxNo ratings yet
- Z-05 Class Slide EVDocument40 pagesZ-05 Class Slide EVXaveer AzadNo ratings yet
- Tao Le, Vikas Bhushan - First Aid For The USMLE Step 1 2020, 30th Anniversary Edition-McGraw-Hill Education (2020) (1) - 1Document9 pagesTao Le, Vikas Bhushan - First Aid For The USMLE Step 1 2020, 30th Anniversary Edition-McGraw-Hill Education (2020) (1) - 1Nanjit SharmaNo ratings yet
- Pneumo Tot MergedDocument103 pagesPneumo Tot MergedAndra BauerNo ratings yet
- ParadwergfewigmDocument6 pagesParadwergfewigmCelline Isabelle ReyesNo ratings yet
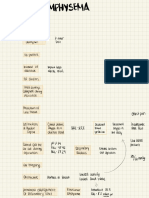
- PathophysiologyDocument1 pagePathophysiologyChua CandiceNo ratings yet
- Ficsher 2Document15 pagesFicsher 2ryan.chow.95No ratings yet
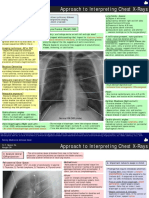
- CR InterpretationDocument2 pagesCR InterpretationDokdem AjaNo ratings yet
- 1 - 2020-Cardiovascular PhysiologyDocument53 pages1 - 2020-Cardiovascular PhysiologyEdward XiamNo ratings yet
- PT - CardiopulmonaryDocument72 pagesPT - CardiopulmonaryLeandrew MagistradoNo ratings yet
- Breathing and Exchange of Gases Part 5Document17 pagesBreathing and Exchange of Gases Part 5GAURANSH AlaghNo ratings yet
- MED2 - Spirometry: Key Parameters and Patterns (Restrictive vs ObstructiveDocument3 pagesMED2 - Spirometry: Key Parameters and Patterns (Restrictive vs ObstructivessasianNo ratings yet
- Chest TraumaDocument4 pagesChest TraumaTrishia GuillermoNo ratings yet
- COPD Harrisons NotesDocument2 pagesCOPD Harrisons NotesJoanna ValenciaNo ratings yet
- Printable Flash CardsDocument29 pagesPrintable Flash CardsBuster-b KhanNo ratings yet
- Nursing Care Plan For Ineffective Airway ClearanceDocument7 pagesNursing Care Plan For Ineffective Airway Clearancepeter_degamo20000% (1)
- Physiology Revision CVS Part 3Document20 pagesPhysiology Revision CVS Part 3Gauri BendreNo ratings yet
- Nursing Care PlanDocument20 pagesNursing Care PlanmelliaiNo ratings yet
- ADAZA BSND 3 OR REQS Concept MAP 3 PDFDocument1 pageADAZA BSND 3 OR REQS Concept MAP 3 PDFKrizle AdazaNo ratings yet
- TIKI: Titles for Treating Hypoxemia with Non-Invasive VentilationDocument8 pagesTIKI: Titles for Treating Hypoxemia with Non-Invasive Ventilationcharlyn206No ratings yet
- Inhalasipolusiudara, Merokok, debu, dan bahan kimia berbahaya menyebabkan Kerusakan paru-paru dan penyakit pernapasan kronisDocument2 pagesInhalasipolusiudara, Merokok, debu, dan bahan kimia berbahaya menyebabkan Kerusakan paru-paru dan penyakit pernapasan kronispetriNo ratings yet
- BBMS2004 L13 Respiratory System - Thoracic Cavity and Respiration 2022Document26 pagesBBMS2004 L13 Respiratory System - Thoracic Cavity and Respiration 2022JinyoungNo ratings yet
- Cardiac PhysioDocument9 pagesCardiac Physiosakuragi jakeNo ratings yet
- BRONCHO ALVEOLAR CARCINOMA DIFFERENTIAL DIAGNOSISDocument3 pagesBRONCHO ALVEOLAR CARCINOMA DIFFERENTIAL DIAGNOSISmarielleaudreeyNo ratings yet
- Summarized MsDocument2 pagesSummarized MssooyahNo ratings yet
- Management of TraumaDocument21 pagesManagement of Traumablazingdk sriNo ratings yet
- Detresa Respiratorie NeonatalaDocument2 pagesDetresa Respiratorie NeonatalaAndrada CatrinoiuNo ratings yet
- Cardiac Assessment ChecklistDocument25 pagesCardiac Assessment ChecklistLovely GopezNo ratings yet
- Monitoring Mechanical Ventilation Using Ventilator WaveformsFrom EverandMonitoring Mechanical Ventilation Using Ventilator WaveformsNo ratings yet
- Multimorbidity: Technical Series On Safer Primary Care. Geneva: World Health Organization 2016. Licence: CC BY-NC-SA 3.0 IGODocument29 pagesMultimorbidity: Technical Series On Safer Primary Care. Geneva: World Health Organization 2016. Licence: CC BY-NC-SA 3.0 IGOMarian Joyce Princess YuqueNo ratings yet
- World Patient Safety Day: Health Worker Safety: A Priority For Patient SafetyDocument8 pagesWorld Patient Safety Day: Health Worker Safety: A Priority For Patient SafetyMarian Joyce Princess YuqueNo ratings yet
- Neck + Benign Neck MassesDocument3 pagesNeck + Benign Neck MassesMarian Joyce Princess YuqueNo ratings yet
- Char Ter: Health Worker Safety: A Priority For Patient SafetyDocument8 pagesChar Ter: Health Worker Safety: A Priority For Patient SafetyMarian Joyce Princess YuqueNo ratings yet
- Triage: Principles and Practice: E. R. FrykbergDocument7 pagesTriage: Principles and Practice: E. R. FrykbergMonyet...No ratings yet
- Tube Thoracostomy Procedure and IndicationsDocument1 pageTube Thoracostomy Procedure and IndicationsMarian Joyce Princess YuqueNo ratings yet
- An Investigation of Attention-Seeking Behavior Through Social Media Post FramingDocument20 pagesAn Investigation of Attention-Seeking Behavior Through Social Media Post FramingMarian Joyce Princess YuqueNo ratings yet
- Understanding Uveitis: Causes, Symptoms, and TreatmentDocument21 pagesUnderstanding Uveitis: Causes, Symptoms, and TreatmentMarian Joyce Princess Yuque100% (1)
- Anesthesia Notes on Respiration and Airway ObstructionDocument36 pagesAnesthesia Notes on Respiration and Airway ObstructionAnil SathyadasNo ratings yet
- Bio-Synthesis of Silver Nanoparticles (Agnp'S) Using Extract Ofputay-Putay (Clitoriaternatea) Flower: Antibacterial and Antioxidant ActivitiesDocument22 pagesBio-Synthesis of Silver Nanoparticles (Agnp'S) Using Extract Ofputay-Putay (Clitoriaternatea) Flower: Antibacterial and Antioxidant ActivitiesMarian Joyce Princess YuqueNo ratings yet
- Krimel SDocument2 pagesKrimel SBords ApaleNo ratings yet
- Case Vignette: CIM Junior ClerksDocument8 pagesCase Vignette: CIM Junior ClerksMarian Joyce Princess YuqueNo ratings yet
- Henoch-Scholein Purpura (HSP) : A Clinico-Etiological Study: Original ArticleDocument6 pagesHenoch-Scholein Purpura (HSP) : A Clinico-Etiological Study: Original ArticleMarian Joyce Princess YuqueNo ratings yet
- Hpim 20e TocDocument15 pagesHpim 20e TocCarlBuscato0% (1)
- FamEd Measles Cases Cogon PardoDocument8 pagesFamEd Measles Cases Cogon PardoMarian YuqueNo ratings yet
- LN Phys Diagnosis FinalDocument165 pagesLN Phys Diagnosis FinalgaasheNo ratings yet
- 3373 Hagnaya Port MOA - 2019Document8 pages3373 Hagnaya Port MOA - 2019Marian Joyce Princess YuqueNo ratings yet
- Weekly Progress PCR Crime Scene InvestigationDocument2 pagesWeekly Progress PCR Crime Scene InvestigationMarian Joyce Princess YuqueNo ratings yet
- Sec 08 ExamDocument1 pageSec 08 ExamMarian Joyce Princess YuqueNo ratings yet
- Sec 05 ExamDocument1 pageSec 05 ExamMarian Joyce Princess YuqueNo ratings yet
- CABS BiosummitDocument2 pagesCABS BiosummitMarian Joyce Princess YuqueNo ratings yet
- Front PageDocument1 pageFront PageMarian Joyce Princess YuqueNo ratings yet
- 3rd Annual Biology Conference PresentationDocument2 pages3rd Annual Biology Conference PresentationMarian Joyce Princess YuqueNo ratings yet
- Pacing Guide hs3 Spring2017Document3 pagesPacing Guide hs3 Spring2017api-319728952No ratings yet
- Group 5 Leadership and TeamworkDocument4 pagesGroup 5 Leadership and TeamworkRanets MamondoleNo ratings yet
- Paracetamol Use Dec 2008Document30 pagesParacetamol Use Dec 2008Nararto PrijogoNo ratings yet
- 2020 Dental-CertificateDocument2 pages2020 Dental-CertificateReygine RamosNo ratings yet
- Mem671 Case Study March 2023Document11 pagesMem671 Case Study March 2023AIMAN ASYRAAF BIN ROSLANNo ratings yet
- Insecticides in IPMDocument17 pagesInsecticides in IPMAsif AzizNo ratings yet
- Lucrare Stiintifica ParodontologieDocument4 pagesLucrare Stiintifica ParodontologieReduceriAvonNo ratings yet
- CDB OilDocument6 pagesCDB Oilmohansid8554No ratings yet
- When Learning and Remembering Compete: A Functional MRI StudyDocument5 pagesWhen Learning and Remembering Compete: A Functional MRI Studyclaire_thixtonNo ratings yet
- Environmental Problem - Test.9 FormDocument2 pagesEnvironmental Problem - Test.9 FormЛетта КошельNo ratings yet
- Catalogo Accesorios MINDRAYDocument64 pagesCatalogo Accesorios MINDRAYitalo100% (2)
- UMK Walk-In Interviews Academic & Support Staff PositionsDocument5 pagesUMK Walk-In Interviews Academic & Support Staff PositionsMuis MuliaNo ratings yet
- Project ManagementDocument54 pagesProject ManagementJustin PauNo ratings yet
- Stakeholder Analysis of Solid Waste Management Schemes in HyderabadDocument24 pagesStakeholder Analysis of Solid Waste Management Schemes in HyderabadJoniJaoNo ratings yet
- Reflection'brain On FireDocument2 pagesReflection'brain On FireJevelyn AgdolNo ratings yet
- Rheumatic Heart DiseaseDocument3 pagesRheumatic Heart DiseasearyshamyleeNo ratings yet
- Matte Last Dc-9509Document2 pagesMatte Last Dc-9509icraoNo ratings yet
- Original Research Paper: ProsthodonticsDocument3 pagesOriginal Research Paper: ProsthodonticsAbdulghny AlshoaibiNo ratings yet
- Rtog 9003Document10 pagesRtog 9003pavanNo ratings yet
- Internship Report of Global Insurance Ltd. by M A Muhaimin Alveen Batch-XIIDocument16 pagesInternship Report of Global Insurance Ltd. by M A Muhaimin Alveen Batch-XIIKIRAN BHATTARAINo ratings yet
- How To Talk To Doctors - A Guide For Effective CommunicationsDocument6 pagesHow To Talk To Doctors - A Guide For Effective Communicationsapi-283596053No ratings yet
- Source 3R Medical Disposable Circumcision Staplers On PDFDocument1 pageSource 3R Medical Disposable Circumcision Staplers On PDFdr_hotNo ratings yet
- College of Nursing and School of Midwifery: Baguio Central UniversityDocument4 pagesCollege of Nursing and School of Midwifery: Baguio Central UniversityKarlNo ratings yet
- 1 Swot Analysis of The Priority Training Programs: Its Implication To Policy Formulation Gulf College, Muscat, OmanDocument5 pages1 Swot Analysis of The Priority Training Programs: Its Implication To Policy Formulation Gulf College, Muscat, OmanGajendra AudichyaNo ratings yet
- M24L40Document7 pagesM24L40Andenet AshagrieNo ratings yet