You might also like
- Primary Biliary CholangitisDocument12 pagesPrimary Biliary CholangitisJuan J. H. AzpeitiaNo ratings yet
- Ulcerative Colitis: An Update: Authors: Jonathan P SegalDocument5 pagesUlcerative Colitis: An Update: Authors: Jonathan P SegalManoel Victor Moreira MachadoNo ratings yet
- Otoimmun Hepatitis and Skin LesionDocument19 pagesOtoimmun Hepatitis and Skin LesionVedat KacarNo ratings yet
- Diagrama de VonDocument15 pagesDiagrama de VonDanny Cumpa CapuñayNo ratings yet
- Immunology of the Liver: Proceedings of an International Meeting Held at King's College Hospital Medical School London, on 6th and 7th July, 1970From EverandImmunology of the Liver: Proceedings of an International Meeting Held at King's College Hospital Medical School London, on 6th and 7th July, 1970No ratings yet
- Jurnal Pendukung Proposal 9Document4 pagesJurnal Pendukung Proposal 9Munawwar AweNo ratings yet
- Cirrosis Biliar PrimariaDocument10 pagesCirrosis Biliar PrimariaGerardo CorreaNo ratings yet
- Intestinal Tuberculosis: A Diagnostic Challenge: Open Access Case DOI: 10.7759/cureus.13058Document4 pagesIntestinal Tuberculosis: A Diagnostic Challenge: Open Access Case DOI: 10.7759/cureus.13058ATIKA INDAH SARINo ratings yet
- Case Report: Reynolds SyndromeDocument2 pagesCase Report: Reynolds SyndromePeertechz Publications Inc.No ratings yet
- EASL Clinical Practice Guidelines: Drug-Induced Liver InjuryDocument40 pagesEASL Clinical Practice Guidelines: Drug-Induced Liver InjuryAnisa Ayu AfridaNo ratings yet
- A Rare Case Presentation Diagnosing Primary Biliary Cholangitis in A Male Patient With Concomitant Type 1 DiabetesDocument8 pagesA Rare Case Presentation Diagnosing Primary Biliary Cholangitis in A Male Patient With Concomitant Type 1 DiabetesRatusweethella Intan Yudagrahania PuspitaNo ratings yet
- Apendicite 2Document6 pagesApendicite 2Dani SNo ratings yet
- Diagnosis Biomarkers in Acute Intestinal Ischemic InjuryDocument13 pagesDiagnosis Biomarkers in Acute Intestinal Ischemic InjuryrizkyNo ratings yet
- Care of The Critically Ill Patient: Jeffrey J. Presneill and John F. CadeDocument5 pagesCare of The Critically Ill Patient: Jeffrey J. Presneill and John F. CadeDataeka InfoNo ratings yet
- Practice: Ulcerative Colitis: Diagnosis and ManagementDocument4 pagesPractice: Ulcerative Colitis: Diagnosis and ManagementBryan NguyenNo ratings yet
- Angioedema HereditarioDocument13 pagesAngioedema HereditarioLUCIAMELENDEZSNo ratings yet
- 2 +Severe+LeptospirosisDocument6 pages2 +Severe+LeptospirosisYhuzz Toma5No ratings yet
- Drug Induced Pathology in The Large IntestineDocument9 pagesDrug Induced Pathology in The Large IntestineBlumeNo ratings yet
- The Histopathological Evaluation of Drug-Induced Liver InjuryDocument13 pagesThe Histopathological Evaluation of Drug-Induced Liver InjuryAnonymous 01bH8iNo ratings yet
- Ileitis When Is Not Chron DiseaseDocument16 pagesIleitis When Is Not Chron DiseasePablo Alejandro Reyes CárdenasNo ratings yet
- Extraintestinal Manifestationsassociated WithinflammatoryboweldiseaseDocument15 pagesExtraintestinal Manifestationsassociated WithinflammatoryboweldiseaseJEFFERSON MUÑOZNo ratings yet
- Coli TidesDocument11 pagesColi TidesAndrea Cayufilo CarmonaNo ratings yet
- Decompensated Liver Cirrhosis: Learning ObjectivesDocument6 pagesDecompensated Liver Cirrhosis: Learning ObjectivesAuliaNo ratings yet
- Functional Gastrointestinal Disorders 2: SeriesDocument14 pagesFunctional Gastrointestinal Disorders 2: SeriesStephani Fontinelli LeonardiNo ratings yet
- Autoimmune PancreatitisDocument7 pagesAutoimmune PancreatitisWinstonNo ratings yet
- Review: Liver Dysfunction in Critical IllnessDocument17 pagesReview: Liver Dysfunction in Critical IllnessRoger Ludeña SalazarNo ratings yet
- Drug Induced Liver Disease 2007Document226 pagesDrug Induced Liver Disease 2007Eric GibsonNo ratings yet
- Kolestasis SepsisDocument21 pagesKolestasis SepsisLilik NatasubrataNo ratings yet
- Celiac DiseaseDocument11 pagesCeliac DiseaseXela AviàNo ratings yet
- Jurnal Literatur Case Series 1Document4 pagesJurnal Literatur Case Series 1Debby LadadoNo ratings yet
- Primary Biliary ColangitisDocument18 pagesPrimary Biliary ColangitisAgustin Velez AcostaNo ratings yet
- Hiding in The Water: Clinical Problem-SolvingDocument6 pagesHiding in The Water: Clinical Problem-SolvingtabareeNo ratings yet
- Ijcmcr CP 00492Document2 pagesIjcmcr CP 00492Larissa CheckNo ratings yet
- The Heart and The GutDocument7 pagesThe Heart and The GutdeboraNo ratings yet
- Ulcerative ColitisDocument8 pagesUlcerative ColitispipotoNo ratings yet
- 69 Haines Ely-Is Psoriasis A Bowel DiseaseDocument14 pages69 Haines Ely-Is Psoriasis A Bowel DiseaseJoe DoeNo ratings yet
- Case PresentationDocument9 pagesCase Presentationmel aquinoNo ratings yet
- Acute Liver FailureDocument12 pagesAcute Liver FailureRodrigo BenitezNo ratings yet
- Clinical Assessment of Liver Disease: HistoryDocument4 pagesClinical Assessment of Liver Disease: HistorySanaNo ratings yet
- Crohns Epidemio Diagnositco y TratamientoDocument16 pagesCrohns Epidemio Diagnositco y TratamientoSantiago ZamudioNo ratings yet
- Acta Anaesthesiologica Taiwanica: Long Wang, Wei-Feng YuDocument8 pagesActa Anaesthesiologica Taiwanica: Long Wang, Wei-Feng Yusitoxpadang ceriaNo ratings yet
- Contents CLDDocument4 pagesContents CLDRezita RamadhaniNo ratings yet
- Treatment of DILIDocument6 pagesTreatment of DILIheroes GamesNo ratings yet
- UREMIANEJMDocument10 pagesUREMIANEJMGeral CocasNo ratings yet
- Manejo en Colangitis Aguda - Libro XDocument4 pagesManejo en Colangitis Aguda - Libro XRodrigo MartinezNo ratings yet
- Jejunojejunal Intussusception As Initial Presentation of Coeliac Disease: A Case Report and Review of LiteratureDocument6 pagesJejunojejunal Intussusception As Initial Presentation of Coeliac Disease: A Case Report and Review of Literatureellya theresiaNo ratings yet
- Walter H. Maloney, M.DDocument6 pagesWalter H. Maloney, M.DIvan DarioNo ratings yet
- Third Case Report Pseudomembranous Colitis Dr. Lisa FarianiDocument18 pagesThird Case Report Pseudomembranous Colitis Dr. Lisa FarianirizkyauliautamaNo ratings yet
- Decompensated Liver CirrhosisDocument6 pagesDecompensated Liver CirrhosisJulian HuningkorNo ratings yet
- Pediatric Gastritis, Gastropathy, and Peptic Ulcer Disease: Education GapDocument10 pagesPediatric Gastritis, Gastropathy, and Peptic Ulcer Disease: Education GapvgmanjunathNo ratings yet
- AngioedemaDocument13 pagesAngioedemaIdkNo ratings yet
- Week 5: Case Analysis Addison'S Disease: Omeprazole (Prilosec) 20 MG ODDocument23 pagesWeek 5: Case Analysis Addison'S Disease: Omeprazole (Prilosec) 20 MG ODMaica LectanaNo ratings yet
- Liver Histology in The Diagnosis and Prognosis of Drug-Induced Liver InjuryDocument5 pagesLiver Histology in The Diagnosis and Prognosis of Drug-Induced Liver InjuryShirleyNo ratings yet
- Cytomegalovirus Triggering Autoimmune Hepatitis: Case Report and Literature ReviewDocument3 pagesCytomegalovirus Triggering Autoimmune Hepatitis: Case Report and Literature ReviewRabiatul 'raney' AdawiyahNo ratings yet
- Practice Questions - Gastrointestinal Disorders 2Document5 pagesPractice Questions - Gastrointestinal Disorders 2Ian GarifeNo ratings yet
- 2003 Probiotic and IBDDocument5 pages2003 Probiotic and IBDsujata sharmaNo ratings yet
- Review: Irina Bancos, Stefanie Hahner, Jeremy Tomlinson, Wiebke ArltDocument11 pagesReview: Irina Bancos, Stefanie Hahner, Jeremy Tomlinson, Wiebke Arltinterna MANADONo ratings yet
- 93 TreaTmenT of AcuTe and Chronic RejecTionDocument12 pages93 TreaTmenT of AcuTe and Chronic RejecTionAbdulRehmanKhanNo ratings yet
- 6 Acute Liver FailureDocument7 pages6 Acute Liver FailureAnonymous ysrxggk21cNo ratings yet
- Economist Impact GFSI 2022 Indonesia Country Report Sep 2022Document4 pagesEconomist Impact GFSI 2022 Indonesia Country Report Sep 2022DewaNo ratings yet
- Impact Metrics - Brochure - 2022-05Document2 pagesImpact Metrics - Brochure - 2022-05DewaNo ratings yet
- Our Priorities: The FAO Strategic ObjectivesDocument16 pagesOur Priorities: The FAO Strategic ObjectivesDewaNo ratings yet
- NC 384 enDocument5 pagesNC 384 enDewaNo ratings yet
- WFP 0000119830Document85 pagesWFP 0000119830DewaNo ratings yet
- Near East Forestry and Range Commission Twenty-First Session Amman, Jordan, 26 - 30 January 2014 The New Strategic Framework For Fao Secretariat NoteDocument29 pagesNear East Forestry and Range Commission Twenty-First Session Amman, Jordan, 26 - 30 January 2014 The New Strategic Framework For Fao Secretariat NoteDewaNo ratings yet
- Coral Reef Habitat Mapping: How Much Detail Can Remote Sensing Provide?Document10 pagesCoral Reef Habitat Mapping: How Much Detail Can Remote Sensing Provide?DewaNo ratings yet
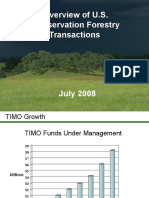
- Overview of U.S. Conservation Forestry TransactionsDocument8 pagesOverview of U.S. Conservation Forestry TransactionsDewaNo ratings yet
- RSugardiman CIFORDocument17 pagesRSugardiman CIFORDewaNo ratings yet
- REDD Safeguards Nov2011Document2 pagesREDD Safeguards Nov2011DewaNo ratings yet
- Agus Setyarso LEGAL CONTEXT FOR FOREST MANAGEMENTcDocument13 pagesAgus Setyarso LEGAL CONTEXT FOR FOREST MANAGEMENTcDewaNo ratings yet
- Bouman Etal 1999Document19 pagesBouman Etal 1999DewaNo ratings yet
- Open Data Program: Disaster Response Activation ProtocolDocument4 pagesOpen Data Program: Disaster Response Activation ProtocolDewaNo ratings yet
- FREL - RL - Julian FoxDocument26 pagesFREL - RL - Julian FoxDewaNo ratings yet
- Safeguards and Multiple Benefits in A REDD+ Mechanism: A Life Cycle Assessment StudyDocument37 pagesSafeguards and Multiple Benefits in A REDD+ Mechanism: A Life Cycle Assessment StudyDewaNo ratings yet
- Rsni2: Pertukaran Data Lintang, Bujur, Dan Tinggi Lokasi GeografisDocument12 pagesRsni2: Pertukaran Data Lintang, Bujur, Dan Tinggi Lokasi GeografisDewaNo ratings yet
- VFG 01 Forest Definition and ExtentDocument4 pagesVFG 01 Forest Definition and ExtentDewaNo ratings yet
- Peatland Conversation: Synthesis ReportDocument34 pagesPeatland Conversation: Synthesis ReportDewaNo ratings yet
- About This Information/Guidance Document: I/G-ActiveDocument2 pagesAbout This Information/Guidance Document: I/G-ActiveDewaNo ratings yet
- Carsjens Vanderknaap 2002Document9 pagesCarsjens Vanderknaap 2002DewaNo ratings yet
- Fact Sheet SVLDocument3 pagesFact Sheet SVLDewaNo ratings yet
- ComputersGeosciencesVol34No7July2008pp715 737Document23 pagesComputersGeosciencesVol34No7July2008pp715 737DewaNo ratings yet
- Course Syllabus: GEOG590 002/ EVPP741 005: Land-Use Modeling Techniques and ApplicationsDocument13 pagesCourse Syllabus: GEOG590 002/ EVPP741 005: Land-Use Modeling Techniques and ApplicationsDewaNo ratings yet
- CHN 211 Week 5 PPT Family Nursing and Nursing ProcessDocument63 pagesCHN 211 Week 5 PPT Family Nursing and Nursing ProcessAlyssa Marie SantosNo ratings yet
- 2021 - CHP - at - English AustriaDocument24 pages2021 - CHP - at - English AustriaElena BivolNo ratings yet
- Full Thesis PDFDocument68 pagesFull Thesis PDFJhomel MontenegroNo ratings yet
- Who Is DiagnosableDocument3 pagesWho Is DiagnosableHamna Shahid100% (1)
- Ascitic Fluid AnalysisDocument3 pagesAscitic Fluid AnalysisLohJNo ratings yet
- January:-: National Youth DayDocument12 pagesJanuary:-: National Youth DaySwadheen KapasiaNo ratings yet
- Biology of Sars-Cov-2Document4 pagesBiology of Sars-Cov-2J. L.No ratings yet
- Evaluasi Sistem Surveilans TB Di Dinas Kesehatan Kabupaten BloraDocument6 pagesEvaluasi Sistem Surveilans TB Di Dinas Kesehatan Kabupaten BloraCantika IkaNo ratings yet
- ADVIA Centaur XPT/XP/CP Immunoassay Systems: For Use Outside The U.S. OnlyDocument2 pagesADVIA Centaur XPT/XP/CP Immunoassay Systems: For Use Outside The U.S. OnlyBulgaru RodicaNo ratings yet
- 361 PDFDocument5 pages361 PDFAlyssa SagarioNo ratings yet
- Drug StudyDocument2 pagesDrug StudyAjay SupanNo ratings yet
- Biomedicine & Pharmacotherapy: A B C B B B BDocument8 pagesBiomedicine & Pharmacotherapy: A B C B B B BprayogarathaNo ratings yet
- Icici Lombard Complete Health Insurance Proposal FormDocument4 pagesIcici Lombard Complete Health Insurance Proposal FormMonal RajNo ratings yet
- Advances in Therapeutic Peptides Targeting G Protein-Coupled ReceptorsDocument25 pagesAdvances in Therapeutic Peptides Targeting G Protein-Coupled ReceptorsAyberk BinbayNo ratings yet
- PulmonologyDocument175 pagesPulmonologyJohanna GarciaNo ratings yet
- Case ReportDocument13 pagesCase ReportZaryab Waheed0% (1)
- OET WRITING EXAM Fast TrackDocument27 pagesOET WRITING EXAM Fast Tracksyed100% (2)
- Med Surg Bullets 1Document21 pagesMed Surg Bullets 1Jor GarciaNo ratings yet
- Antidiabetic Activity of Plants ThesisDocument8 pagesAntidiabetic Activity of Plants Thesisygsyoeikd100% (1)
- English: Fourth Quarter - Module 5Document14 pagesEnglish: Fourth Quarter - Module 5Nathalie Jefsieji Dela CruzNo ratings yet
- Fatty Acids and Glycerol - IIDocument25 pagesFatty Acids and Glycerol - IIwax walba haye mediaNo ratings yet
- Vulvar Melanosis: Two Case ReportDocument4 pagesVulvar Melanosis: Two Case ReportValentina AdindaNo ratings yet
- Porphyria Unsafe Drugs - Extensive ListDocument23 pagesPorphyria Unsafe Drugs - Extensive ListDorisStinson100% (1)
- Physical Education SbaDocument46 pagesPhysical Education SbaDaniel Dowding80% (5)
- 3rd Year SyllabusDocument37 pages3rd Year SyllabusDevid DinoNo ratings yet
- Cervical Disc ProlapseDocument27 pagesCervical Disc ProlapseMaroofAliNo ratings yet
- 8 Science Worksheet ch2 1Document3 pages8 Science Worksheet ch2 1KSP Classes GondiaNo ratings yet
- I. Overview of Abnormal PsychologyDocument55 pagesI. Overview of Abnormal PsychologyTori YamaNo ratings yet
- Aphasia Info Sheet From LingraphicaDocument1 pageAphasia Info Sheet From LingraphicaDonia ElshazlyNo ratings yet
- Revisiting Diuretic Choice in Chronic Kidney.4Document8 pagesRevisiting Diuretic Choice in Chronic Kidney.4FABIO JAVIER BRAVO SALDARRIAGANo ratings yet