You might also like
- MAD Magazine 001Document36 pagesMAD Magazine 001ClarkcoffeyNo ratings yet
- Natural ResourcesDocument5 pagesNatural ResourcesAsrock Loop100% (1)
- General Internal Medicine Discharge SummaryDocument3 pagesGeneral Internal Medicine Discharge SummaryAnusha Bhandekar100% (1)
- 11 Biology Notes Ch10 Cell Cycle and Cell DevisionDocument7 pages11 Biology Notes Ch10 Cell Cycle and Cell DevisionRohit ThakranNo ratings yet
- PI734DDocument8 pagesPI734Deng_hopaNo ratings yet
- Heidegger and RhetoricDocument202 pagesHeidegger and RhetoricMagda AliNo ratings yet
- HYDROGEN - Anti-Oxidant and Anti-Inflammatory Effects of Hydr-Rich WaterDocument16 pagesHYDROGEN - Anti-Oxidant and Anti-Inflammatory Effects of Hydr-Rich WaterCarlos SilvaNo ratings yet
- 2019 Article 388Document5 pages2019 Article 388Natalie Sarah MoonNo ratings yet
- 10 A Case of Ethylene Glycol Intoxication With Acute Renal Injury Successful Recovery by Fomepizole and Renal Replacement TherapyDocument5 pages10 A Case of Ethylene Glycol Intoxication With Acute Renal Injury Successful Recovery by Fomepizole and Renal Replacement TherapyKarla Labbe RodriguezNo ratings yet
- Bab Ii-1Document17 pagesBab Ii-1BambangFitJøøzNo ratings yet
- 534 2006 Article 1156Document8 pages534 2006 Article 1156Ferry RusdiansaputraNo ratings yet
- TG 13 Updated Tokyo GuidelinesDocument8 pagesTG 13 Updated Tokyo GuidelinessamuelionardiNo ratings yet
- Jurnal 8Document6 pagesJurnal 8Tri UlfaNo ratings yet
- MainDocument3 pagesMainMila KarmilaNo ratings yet
- Nakazawa 2016Document7 pagesNakazawa 2016Yamila VicenteNo ratings yet
- Drug-Induced Liver Injury Associated With Complementary and Alternative MedicinesDocument8 pagesDrug-Induced Liver Injury Associated With Complementary and Alternative MedicinesTimotius Kevin NatanaelNo ratings yet
- The Practice Guidelines For Primary Care of Acute Abdomen 2015Document37 pagesThe Practice Guidelines For Primary Care of Acute Abdomen 2015tamiNo ratings yet
- Asia-Pacific Clinical Practice Guidelines On The Management of Hepatocellular Carcinoma: A 2017 UpdateDocument55 pagesAsia-Pacific Clinical Practice Guidelines On The Management of Hepatocellular Carcinoma: A 2017 UpdateNi Nyoman Indirawati KusumaNo ratings yet
- Yoshio Terada Takashi Wada Kent Doi Acute Kidney Injury and Regenerative Medicine Springer Singapore Springer 2020Document390 pagesYoshio Terada Takashi Wada Kent Doi Acute Kidney Injury and Regenerative Medicine Springer Singapore Springer 2020XtineNo ratings yet
- Radioiodine TherapyDocument5 pagesRadioiodine Therapyaccime24No ratings yet
- Management of Refractory Cirrhotic Ascites: Challenges and SolutionsDocument17 pagesManagement of Refractory Cirrhotic Ascites: Challenges and SolutionsNur InayahNo ratings yet
- Management of Liver Cirrhosis Between Primary Care PDFDocument11 pagesManagement of Liver Cirrhosis Between Primary Care PDFAnggi YnNo ratings yet
- Cytomegalovirus_gastritisDocument3 pagesCytomegalovirus_gastritisrenzoNo ratings yet
- A Liver Manifestation Hepatic CirrhosisDocument11 pagesA Liver Manifestation Hepatic CirrhosisAjit SinghNo ratings yet
- Efek Hepatoprotektif N-Asetilsistein Dalam Mencegah Drug-Induced Liver InjuDocument6 pagesEfek Hepatoprotektif N-Asetilsistein Dalam Mencegah Drug-Induced Liver InjuAndry Wahyudi AgusNo ratings yet
- Clinical Diagnostic Criteria of Autoimmune PancreatitisDocument6 pagesClinical Diagnostic Criteria of Autoimmune PancreatitisHesaNo ratings yet
- MedicineDocument5 pagesMedicineRoyd Jesse Kwibisa JrNo ratings yet
- A Randomized Clinical Trial ToDocument6 pagesA Randomized Clinical Trial Todella psNo ratings yet
- AsiaPacific 2017 Hepatocellular CarcinomaDocument55 pagesAsiaPacific 2017 Hepatocellular CarcinomaCecille ZacateNo ratings yet
- 30140-Article Text-56524-1-10-20201030Document11 pages30140-Article Text-56524-1-10-20201030melendezjmanuelNo ratings yet
- A Review On Hepatitis and Haemostasis: February 2018Document24 pagesA Review On Hepatitis and Haemostasis: February 2018Lydie Praxede EkoboNo ratings yet
- Leptospirosis CasosDocument2 pagesLeptospirosis CasosfelipeNo ratings yet
- Successful Outcome of Ineffective Infliximab Treated Autoimmune Enteropathy With Oral Budesonide 9800Document3 pagesSuccessful Outcome of Ineffective Infliximab Treated Autoimmune Enteropathy With Oral Budesonide 9800Desmo13No ratings yet
- Diagnosis of Liver DiseaseFrom EverandDiagnosis of Liver DiseaseEtsuko HashimotoNo ratings yet
- Cholangitis PDFDocument7 pagesCholangitis PDFWorku KifleNo ratings yet
- Updated Tokyo Guidelines for the management of acute cholangitis and cholecystitis (TG13Document109 pagesUpdated Tokyo Guidelines for the management of acute cholangitis and cholecystitis (TG13nostra83No ratings yet
- Definitions, Pathophysiology, and Epidemiology of Acute Cholangitis and Cholecystitis - Tokyo GuidelinesDocument13 pagesDefinitions, Pathophysiology, and Epidemiology of Acute Cholangitis and Cholecystitis - Tokyo GuidelinesNilamsari KurniasihNo ratings yet
- 2013 Basic Concepts of Fluid and Electrolyte TherapyDocument137 pages2013 Basic Concepts of Fluid and Electrolyte Therapytd5xb7w4dpNo ratings yet
- Negrini Ileoparaliticoeinsuffepaticafeb09Document6 pagesNegrini Ileoparaliticoeinsuffepaticafeb09jikhNo ratings yet
- GALAinpregnancyDocument6 pagesGALAinpregnancyumar faruqiNo ratings yet
- Intestinal Tuberculosis: A Diagnostic Challenge: Open Access Case DOI: 10.7759/cureus.13058Document4 pagesIntestinal Tuberculosis: A Diagnostic Challenge: Open Access Case DOI: 10.7759/cureus.13058ATIKA INDAH SARINo ratings yet
- Clinical Effect and Mechanism of Alkaline Reduced WaterDocument5 pagesClinical Effect and Mechanism of Alkaline Reduced Waterelalaoui25No ratings yet
- (Q1) Pone.0169593Document16 pages(Q1) Pone.0169593wiradewi lestariNo ratings yet
- 2008 RefeedingsyndromeDocument9 pages2008 RefeedingsyndromeMarinaNo ratings yet
- Hepatology - 2004 - Angulo - Medical Treatment For Primary Sclerosing Cholangitis Risk Versus BenefitDocument2 pagesHepatology - 2004 - Angulo - Medical Treatment For Primary Sclerosing Cholangitis Risk Versus BenefitRirinwianaNo ratings yet
- Effects of Drinking Hydrogen-Rich WaterDocument9 pagesEffects of Drinking Hydrogen-Rich WaterfooykokNo ratings yet
- Colonoscopy Report-1-Merged 22MBDocument84 pagesColonoscopy Report-1-Merged 22MBMilos AndjelovNo ratings yet
- The Effect of Smoking On Fertility Hormones in Male Adult Smokers in South-South NigeriaDocument7 pagesThe Effect of Smoking On Fertility Hormones in Male Adult Smokers in South-South NigeriaHenny WijayaNo ratings yet
- Larussa 2017Document25 pagesLarussa 2017alan.rangel.puenteNo ratings yet
- Sialadenosis in A Patient With Alcoholic Fatty Liv PDFDocument3 pagesSialadenosis in A Patient With Alcoholic Fatty Liv PDFPutri AmaliaNo ratings yet
- Yamaguchi 2015 CKDDocument9 pagesYamaguchi 2015 CKDWing Yee YuenNo ratings yet
- CMJ 130 2011Document2 pagesCMJ 130 2011studentstoma61No ratings yet
- 2016 Guidelines For The Management of Thyroid StorDocument41 pages2016 Guidelines For The Management of Thyroid StorStella Gracia OctaricaNo ratings yet
- Ozone Therapy Ameliorates Tubulointerstitial Inflammation by Regulating TLR4 in Adenine Induced CKD RatsDocument10 pagesOzone Therapy Ameliorates Tubulointerstitial Inflammation by Regulating TLR4 in Adenine Induced CKD RatsBoby FaesalNo ratings yet
- Medical Mycology Case ReportsDocument3 pagesMedical Mycology Case ReportsReza FaisalNo ratings yet
- 2 +Severe+LeptospirosisDocument6 pages2 +Severe+LeptospirosisYhuzz Toma5No ratings yet
- Tokyo Guidelines 2018 Initial Management of AcuteDocument11 pagesTokyo Guidelines 2018 Initial Management of Acutenova adiNo ratings yet
- BJSTR MS Id 001072Document4 pagesBJSTR MS Id 001072Jatin SinghNo ratings yet
- DITIADocument5 pagesDITIADian PertiwiNo ratings yet
- Alkalinisation of Urine in Patients With Infection of Urinary TractDocument4 pagesAlkalinisation of Urine in Patients With Infection of Urinary Tractbima-senaNo ratings yet
- Beneficial Biological Effects of Molecular Hydrogen - A Review of 321 ArticlesDocument21 pagesBeneficial Biological Effects of Molecular Hydrogen - A Review of 321 ArticlesfooykokNo ratings yet
- Incidence and Characteristics of Acute Kidney Injury in Severe Diabetic KetoacidosisDocument6 pagesIncidence and Characteristics of Acute Kidney Injury in Severe Diabetic KetoacidosisMarcelliaNo ratings yet
- Ala Cholecystitis FinalDocument20 pagesAla Cholecystitis FinalJessica RamosNo ratings yet
- Awuku 1552016 BJMMR26166Document4 pagesAwuku 1552016 BJMMR26166Kush GuptaNo ratings yet
- CP 108: Home Assignment Topics-2021Document2 pagesCP 108: Home Assignment Topics-2021Biswajit PaulNo ratings yet
- Bitterness Compounds in Coffee Brew Measured by Analytical Instruments and Taste Sensing SystemDocument34 pagesBitterness Compounds in Coffee Brew Measured by Analytical Instruments and Taste Sensing SystemSolisNo ratings yet
- Modul 1 - Pengantar Remote SensingDocument60 pagesModul 1 - Pengantar Remote SensingNgurah Ade KalyanaNo ratings yet
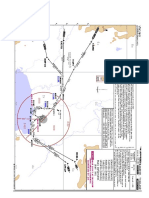
- VTBS 20-3DDocument1 pageVTBS 20-3Dwong keen faivNo ratings yet
- Nature 1Document6 pagesNature 1Susanty SainudinNo ratings yet
- CompressorsDocument20 pagesCompressorsCarlos Alberto Huamaní GonzalesNo ratings yet
- Environmental Accounting in The Philippines: by Romulo A. Virola, Sylvia M. de Perio and Eduardo T. AngelesDocument27 pagesEnvironmental Accounting in The Philippines: by Romulo A. Virola, Sylvia M. de Perio and Eduardo T. AngelesLaraNo ratings yet
- WB City GateDocument7 pagesWB City GateDiegoNo ratings yet
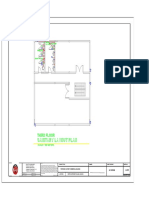
- Sanitary Layout Plan: Third FloorDocument1 pageSanitary Layout Plan: Third FloorFrancis KoNo ratings yet
- Chapter 17Document48 pagesChapter 17MahmoudKhedrNo ratings yet
- Rectal FluidtherapyDocument7 pagesRectal FluidtherapyIan SabogalNo ratings yet
- LinearDocument46 pagesLinearSheikh Riasat100% (1)
- Wall Mounted Wireless Air ConditionersDocument2 pagesWall Mounted Wireless Air ConditionerspenavicbNo ratings yet
- PSPD Activity 3Document4 pagesPSPD Activity 3laurynnaNo ratings yet
- 5 Commandments of DatingDocument8 pages5 Commandments of DatingBariki MwasagaNo ratings yet
- User Manual For Digital Logic Trainer KitDocument6 pagesUser Manual For Digital Logic Trainer KitHonnura HarijanaNo ratings yet
- MTD Big Bore Engines 78 277cc 83 357cc 90 420cc Repair Manual PDFDocument136 pagesMTD Big Bore Engines 78 277cc 83 357cc 90 420cc Repair Manual PDFGiedrius MalinauskasNo ratings yet
- Air Pollution Sources & EffectsDocument2 pagesAir Pollution Sources & EffectsJoanne Ash MajdaNo ratings yet
- The Volcanic Explosivity Index (VEI)Document8 pagesThe Volcanic Explosivity Index (VEI)Rakhmatul ArafatNo ratings yet
- Modeling Endocrine Control of The Pituitary-Ovarian Axis: Androgenic Influence and Chaotic DynamicsDocument22 pagesModeling Endocrine Control of The Pituitary-Ovarian Axis: Androgenic Influence and Chaotic DynamicsKerin ArdyNo ratings yet
- Panasonic DMP BDT230PDocument87 pagesPanasonic DMP BDT230PaldoNo ratings yet
- Interview Questions - Godrej Technical & HR Interview QuestionsDocument9 pagesInterview Questions - Godrej Technical & HR Interview Questionssasithar jaisankaranNo ratings yet
- Nireesh Kumar Paidi - Updated ResumeDocument5 pagesNireesh Kumar Paidi - Updated ResumeNikhil Reddy NamreddyNo ratings yet
- NCE - Lesson 61 (A)Document8 pagesNCE - Lesson 61 (A)Zahir Pacasum-OmarNo ratings yet
- Providence Anadime Chorus Adc3Document1 pageProvidence Anadime Chorus Adc3wplaisNo ratings yet