You might also like
- Values of NursingDocument27 pagesValues of NursingJay-l Escuadra82% (22)
- The Great Psychotherapy Debate PDFDocument223 pagesThe Great Psychotherapy Debate PDFCasey Lewis100% (10)
- Digest of Philippine Association of Service Exporters, Inc. v. Torres (G.R. No. 101279)Document2 pagesDigest of Philippine Association of Service Exporters, Inc. v. Torres (G.R. No. 101279)Rafael Pangilinan83% (12)
- Treatment Planning from a Reality Therapy PerspectiveFrom EverandTreatment Planning from a Reality Therapy PerspectiveNo ratings yet
- Clinical FormulationDocument24 pagesClinical Formulationaimee2oo8100% (2)
- DefinitionDocument5 pagesDefinitionEmma Taylor100% (1)
- Week 6 Psych 655Document5 pagesWeek 6 Psych 655KimMorganNo ratings yet
- Final Draft Tomas SebastianDocument5 pagesFinal Draft Tomas Sebastianapi-457468406No ratings yet
- Alternative Approaches To TherapyDocument53 pagesAlternative Approaches To Therapyemilythorne1688No ratings yet
- Ethical Dilemmas in PsychotherapyDocument3 pagesEthical Dilemmas in PsychotherapykokostarkNo ratings yet
- Portfolio Psychology Career Reflection PaperDocument7 pagesPortfolio Psychology Career Reflection Paperapi-579574346No ratings yet
- Sociocultural PerspectiveDocument11 pagesSociocultural PerspectiveadeshNo ratings yet
- Troi LuonDocument5 pagesTroi LuonwanNo ratings yet
- Nancy McWilliams - Beyond Traits - Personality As Intersubjective ThemesDocument30 pagesNancy McWilliams - Beyond Traits - Personality As Intersubjective Themesmeditationinstitute.netNo ratings yet
- Critique of Humanistic PsychotherapyDocument31 pagesCritique of Humanistic PsychotherapyumetaniNo ratings yet
- Termino Na Psicoterpia2Document3 pagesTermino Na Psicoterpia2Mariana MartinsNo ratings yet
- Ethical Components of The Professional RoleDocument11 pagesEthical Components of The Professional Roleapi-414663729No ratings yet
- Integrating Spirituality and Religion Into PsychotherapyDocument7 pagesIntegrating Spirituality and Religion Into PsychotherapyDanielNo ratings yet
- Two Ethics Case ScenariosDocument3 pagesTwo Ethics Case ScenariosEguia NielNo ratings yet
- Gale Researcher Guide for: Overview of Behavioral and Mental Disorders in PsychologyFrom EverandGale Researcher Guide for: Overview of Behavioral and Mental Disorders in PsychologyNo ratings yet
- SOCE Journal Club FINAL - Cormac MaguireDocument32 pagesSOCE Journal Club FINAL - Cormac Maguirecmaguire92No ratings yet
- Ethical and Professional Issues in Clinical PsychologyDocument6 pagesEthical and Professional Issues in Clinical Psychologymughaltalha01249212015No ratings yet
- CBT Gay LesbiansDocument15 pagesCBT Gay Lesbianschristof75No ratings yet
- Psychology Plays An Important Role in Addiction CoDocument8 pagesPsychology Plays An Important Role in Addiction CoAlfee KariukiNo ratings yet
- Introduction To The Main Theories and Key DebatesDocument18 pagesIntroduction To The Main Theories and Key DebatesGeorge VarvatsouliasNo ratings yet
- Brief Humanistic and Existential TherapiesDocument17 pagesBrief Humanistic and Existential TherapiesSanchez Roman100% (1)
- Van Scoyoc, S. (2017) - The Use and Misuse of Psychometrics in Clinical Settings. in B. Cripps (Ed.)Document17 pagesVan Scoyoc, S. (2017) - The Use and Misuse of Psychometrics in Clinical Settings. in B. Cripps (Ed.)susanvanscoyoc9870No ratings yet
- Importance of PsychologyDocument8 pagesImportance of PsychologyAlfee KariukiNo ratings yet
- Clinical Case Studies-LibreDocument12 pagesClinical Case Studies-LibreCazimir SaftuNo ratings yet
- Types of PsychotherapyDocument4 pagesTypes of Psychotherapyanti100% (1)
- Research LectureDocument5 pagesResearch LectureKassandra CatNo ratings yet
- Week 6 Review Challenge-SMEDocument4 pagesWeek 6 Review Challenge-SMEPylorikNo ratings yet
- Navigating Personal Values and Client-Centered Care: An Analysis of A Psychologist's Dilemma - Mohamedh MazinDocument7 pagesNavigating Personal Values and Client-Centered Care: An Analysis of A Psychologist's Dilemma - Mohamedh MazinzinstudiesNo ratings yet
- Brief Humanistic and Existential TherapyDocument16 pagesBrief Humanistic and Existential TherapyKrishnapriya T SNo ratings yet
- Characteristics of Clinical PsychologistDocument6 pagesCharacteristics of Clinical PsychologistMahnoor MalikNo ratings yet
- Psychosocial NursingDocument21 pagesPsychosocial NursingAngeline Angeles100% (1)
- Hayes HofmannDocument13 pagesHayes HofmannNinoska Benites RamosNo ratings yet
- Dr. J.I. Nwapi,: MBBS, Fwacp, FMCFM Lecturer I/Consultant Family PhysicianDocument46 pagesDr. J.I. Nwapi,: MBBS, Fwacp, FMCFM Lecturer I/Consultant Family PhysicianjaphetnwapiNo ratings yet
- C-Self-Reflection Paper (Peter 2)Document9 pagesC-Self-Reflection Paper (Peter 2)Ras Jemoh100% (1)
- Significant Variables That Influence Psychotherapy PDFDocument38 pagesSignificant Variables That Influence Psychotherapy PDFIqbal BaryarNo ratings yet
- Characteristics of Good PsychologistDocument3 pagesCharacteristics of Good PsychologistJavedNo ratings yet
- 04-EPPT-Course-Unit-5 Caring Honesty and Conflict of InterestDocument7 pages04-EPPT-Course-Unit-5 Caring Honesty and Conflict of InterestGuillana Mae CastellonNo ratings yet
- Setonion Seminar Code of Ethics OtDocument4 pagesSetonion Seminar Code of Ethics Otapi-704038777No ratings yet
- Clinical Assessment Introduction LectureDocument34 pagesClinical Assessment Introduction Lecture-sparkle1234No ratings yet
- General Principles of The InterviewDocument76 pagesGeneral Principles of The InterviewEdi DrimaNo ratings yet
- Supplemental-Guide GenderQuestWkbkTeensDocument9 pagesSupplemental-Guide GenderQuestWkbkTeensPaula ZuccoloNo ratings yet
- End of Life - CareDocument1 pageEnd of Life - CareRosell NavajaNo ratings yet
- Indications and Contraindications For Couples TherapyDocument10 pagesIndications and Contraindications For Couples TherapyVartika jainNo ratings yet
- Person Centred TheoryDocument7 pagesPerson Centred TheoryWendy Tate100% (2)
- Herbal Formularies For Health Professionals, Volume 4 - IntroductionDocument9 pagesHerbal Formularies For Health Professionals, Volume 4 - IntroductionChelsea Green Publishing33% (3)
- ROLE of AssingmentDocument7 pagesROLE of AssingmentMaleeha AyubNo ratings yet
- Counseling and Psychotherapy-1Document40 pagesCounseling and Psychotherapy-1Sara Kaleem100% (1)
- Motivated Moral Reasoning in PsychotherapyDocument4 pagesMotivated Moral Reasoning in PsychotherapyJohn GavazziNo ratings yet
- Thesis Proposal On Spirituality and Psyc PDFDocument16 pagesThesis Proposal On Spirituality and Psyc PDFAnonymous Dq88vO7aNo ratings yet
- wp2 - Lit ReviewDocument11 pageswp2 - Lit Reviewapi-544582640No ratings yet
- The Efficacy of Psychodynamic Psychotherapy: American Psychologist, in PressDocument25 pagesThe Efficacy of Psychodynamic Psychotherapy: American Psychologist, in PressHPS_orgNo ratings yet
- Nature, Scope, Role, History and Current Status of Clinical Psychology and AssessmentsDocument15 pagesNature, Scope, Role, History and Current Status of Clinical Psychology and Assessmentsabisha.angeline22No ratings yet
- Research ProposalDocument8 pagesResearch ProposalEngrAbeer ArifNo ratings yet
- Medicina 5Document14 pagesMedicina 5romulus nicoaraNo ratings yet
- The Ethical Decision-Making ModelDocument2 pagesThe Ethical Decision-Making ModelkokostarkNo ratings yet
- The Ethical Decision Making ModelDocument2 pagesThe Ethical Decision Making ModelkokostarkNo ratings yet
- Listen and Talk (Benefits of Soliciting Input) : Examples of Involving PatientsDocument2 pagesListen and Talk (Benefits of Soliciting Input) : Examples of Involving PatientskokostarkNo ratings yet
- Ethical Dilemmas in PsychotherapyDocument3 pagesEthical Dilemmas in PsychotherapykokostarkNo ratings yet
- GC1 Q1 Week-5ab PDFDocument12 pagesGC1 Q1 Week-5ab PDFLovely MavilNo ratings yet
- ODLI20161010 - 035-UPD-es - AR-FastFlex-LED-module 2x8 - 740-Gen-Ficha-TécnicaDocument11 pagesODLI20161010 - 035-UPD-es - AR-FastFlex-LED-module 2x8 - 740-Gen-Ficha-TécnicamyryqNo ratings yet
- Chemistry Investigatory Project Class 12Document18 pagesChemistry Investigatory Project Class 12Tushar ChopraNo ratings yet
- Role of Fdi in Indian EconomyDocument13 pagesRole of Fdi in Indian EconomyAmit PatelNo ratings yet
- Project Management TeamDocument9 pagesProject Management TeamFrancis Jerome CuarterosNo ratings yet
- A Commerce in ButterfliesDocument6 pagesA Commerce in ButterfliesJenika Jean ReanzaresNo ratings yet
- Psalm 110 The King and The PriestDocument19 pagesPsalm 110 The King and The Priestanibal_santelizNo ratings yet
- Nursing EducationDocument31 pagesNursing EducationArlyn Biton SantiagoNo ratings yet
- 1 - Macro Perspective of Tourism and Hospitality 3Document4 pages1 - Macro Perspective of Tourism and Hospitality 3Alex YbanezNo ratings yet
- Deputation/Assignment Abroad: Copy of CSIR O.M.No.21/Dir/97-ISTAD Dated 15.10.1997Document5 pagesDeputation/Assignment Abroad: Copy of CSIR O.M.No.21/Dir/97-ISTAD Dated 15.10.1997Anonymous H0Cv2Gts6kNo ratings yet
- President Joe Biden's Stimulus PlanDocument19 pagesPresident Joe Biden's Stimulus PlanThe College FixNo ratings yet
- Cisco Unified IP Phone Release Notes For Firmware Release 9.2 (3) (SCCP and SIP)Document14 pagesCisco Unified IP Phone Release Notes For Firmware Release 9.2 (3) (SCCP and SIP)teju_scribddownloadNo ratings yet
- Ozone Mag Super Bowl 2006 Special EditionDocument49 pagesOzone Mag Super Bowl 2006 Special EditionOzone MagazineNo ratings yet
- Party Planning Checklist: DetailsDocument1 pageParty Planning Checklist: DetailslauveromNo ratings yet
- Blackstonian Theory, Retrospective, and Prospective OverrulingDocument6 pagesBlackstonian Theory, Retrospective, and Prospective OverrulingAbdul NihalNo ratings yet
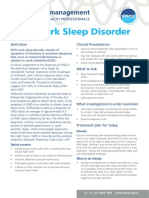
- Shiftwork Disorder - 0617Document2 pagesShiftwork Disorder - 0617hector ignacio CastellucciNo ratings yet
- Muhajir DiasporaDocument10 pagesMuhajir DiasporaneoindusNo ratings yet
- Thesis Proposal FinalDocument5 pagesThesis Proposal FinalRian Binte KamalNo ratings yet
- Muhammad Zahid Farid - Resume PDFDocument2 pagesMuhammad Zahid Farid - Resume PDFMuhammad Zahid FaridNo ratings yet
- Century Textile Mills, Inc. vs. NLRCDocument5 pagesCentury Textile Mills, Inc. vs. NLRCRaymarc Elizer AsuncionNo ratings yet
- Dell EMC Unity: Unisphere OverviewDocument41 pagesDell EMC Unity: Unisphere OverviewJim SmithNo ratings yet
- ECSS v3 BrochureDocument39 pagesECSS v3 BrochureMahesh BhatNo ratings yet
- G2 Quick Start Tutorial PDFDocument19 pagesG2 Quick Start Tutorial PDFEmanuel GutierrezNo ratings yet
- Egyptian Dance Pe 1Document21 pagesEgyptian Dance Pe 1Jysn JsNo ratings yet
- Moodle - Copy - SQLDocument184 pagesMoodle - Copy - SQL'Aan AndriaNo ratings yet
- Failure Modes Introduction: LandslidesDocument6 pagesFailure Modes Introduction: LandslidesSEDIMNo ratings yet
- Tamesol Projects (En)Document16 pagesTamesol Projects (En)Ara AkramNo ratings yet
- Reviews for finalDocument7 pagesReviews for finalantt234111eNo ratings yet
- Greenwood High Unit Test-I (2020 - 21) Subject: History & Civics Grade: VII Duration: 40 Min Date:27/07/20 Max Marks: 25Document3 pagesGreenwood High Unit Test-I (2020 - 21) Subject: History & Civics Grade: VII Duration: 40 Min Date:27/07/20 Max Marks: 25Akshitaa PandeyNo ratings yet