You might also like
- Pitch-Side Management of Acute Shoulder Dislocations: A Conceptual ReviewDocument9 pagesPitch-Side Management of Acute Shoulder Dislocations: A Conceptual ReviewElan R.S.No ratings yet
- Luxaciones Cadera 3Document11 pagesLuxaciones Cadera 3Sammy FarahNo ratings yet
- Subaxial Cervical Spine Trauma: Evaluation and Surgical Decision-MakingDocument8 pagesSubaxial Cervical Spine Trauma: Evaluation and Surgical Decision-Makingvicky174No ratings yet
- Distal Radius Fractures in The Elderly: Review ArticleDocument17 pagesDistal Radius Fractures in The Elderly: Review ArticleBli PutuNo ratings yet
- Luthringer 2019Document14 pagesLuthringer 2019Cristian Diaz KooNo ratings yet
- Jurnal 5Document16 pagesJurnal 5Melinia Almha RamadhaniNo ratings yet
- Care For Spinal ImobilizationDocument20 pagesCare For Spinal ImobilizationRhyal MudatsirNo ratings yet
- Splints and Casts Indications and MethodsDocument10 pagesSplints and Casts Indications and MethodsManish MauryaNo ratings yet
- Manejo Inicial Trauma EspinalDocument7 pagesManejo Inicial Trauma EspinalJuan MVNo ratings yet
- Moore 2019Document5 pagesMoore 2019Tania salais obregonNo ratings yet
- Spinal ImmobilisationDocument34 pagesSpinal ImmobilisationGunther BielenNo ratings yet
- Cervical Spine InjuriesDocument11 pagesCervical Spine InjuriesPrakarsa Adi Daya NusantaraNo ratings yet
- Management of Acute Spinal Cord Injury - A Summary of The Evidence Pertaining To The Acute Management, Operative and Non-Operative ManagementDocument12 pagesManagement of Acute Spinal Cord Injury - A Summary of The Evidence Pertaining To The Acute Management, Operative and Non-Operative Managementzee zeeNo ratings yet
- Trauma C1 C2Document8 pagesTrauma C1 C2Karen OrtizNo ratings yet
- Preoperative Planning in Total Knee Arthroplasty PDFDocument11 pagesPreoperative Planning in Total Knee Arthroplasty PDFElmer NarvaezNo ratings yet
- Preoperative Planning in Total Knee Arthroplasty PDFDocument11 pagesPreoperative Planning in Total Knee Arthroplasty PDFElmer NarvaezNo ratings yet
- Orthopaedic_Knowledge_Update_13_Ebook_Without_Mult..._----_(Section_3_Trauma)Document13 pagesOrthopaedic_Knowledge_Update_13_Ebook_Without_Mult..._----_(Section_3_Trauma)2wk8cr7rmdNo ratings yet
- Fractures of Humerus and Their Treatment ModalitiesDocument4 pagesFractures of Humerus and Their Treatment ModalitiesRhizka djitmauNo ratings yet
- Pre-Hospital Spinal Immobilisation - An Initial Consensus StatementDocument4 pagesPre-Hospital Spinal Immobilisation - An Initial Consensus StatementJade OttoniNo ratings yet
- Surat KuasaDocument9 pagesSurat KuasarifkizidnyNo ratings yet
- Lumbar Spine Fusion What Is The EvidenceDocument5 pagesLumbar Spine Fusion What Is The EvidencecsdNo ratings yet
- 2021 - Damage Control Orthopaedics in Spinal TraumaDocument12 pages2021 - Damage Control Orthopaedics in Spinal TraumaJimena BetancurNo ratings yet
- Spinal Cord Injury PDFDocument14 pagesSpinal Cord Injury PDFNiaNo ratings yet
- Current Concepts in Upper-Extremity Amputation: Key WordsDocument10 pagesCurrent Concepts in Upper-Extremity Amputation: Key WordsCarlos GonzalesNo ratings yet
- Anaesthesia For Hip Fracture Repair: C. Shelton and S. WhiteDocument8 pagesAnaesthesia For Hip Fracture Repair: C. Shelton and S. WhiteAlexeyBobNo ratings yet
- Management of Degenerative Lumbar Spinal Stenosis in The ElderlyDocument7 pagesManagement of Degenerative Lumbar Spinal Stenosis in The ElderlySandroNo ratings yet
- Anky Losing SpondylitisDocument5 pagesAnky Losing SpondylitisdevanbalukhNo ratings yet
- Update On Traumatic Acute Spinal Cord Injury.: DOI: 10.1016/j.medine.2016.11.007Document38 pagesUpdate On Traumatic Acute Spinal Cord Injury.: DOI: 10.1016/j.medine.2016.11.007witwiiwNo ratings yet
- Managementofdistal Femurfracturesinadults: An Overview of OptionsDocument12 pagesManagementofdistal Femurfracturesinadults: An Overview of OptionsDoctor's BettaNo ratings yet
- Distal Humerus Fractures: J. Whitcomb Pollock, MD, FRCSC, Kenneth J. Faber, MD, MHPE, FRCSC, George S. Athwal, MD, FRCSCDocument14 pagesDistal Humerus Fractures: J. Whitcomb Pollock, MD, FRCSC, Kenneth J. Faber, MD, MHPE, FRCSC, George S. Athwal, MD, FRCSCRadu UrcanNo ratings yet
- Axillary Nerve Palsy and Deltoid Muscle AtonyDocument12 pagesAxillary Nerve Palsy and Deltoid Muscle AtonyLaura CandussiNo ratings yet
- 266 Full PDFDocument7 pages266 Full PDFannisaNo ratings yet
- Guideline Reino Unido - Pre-Hospital Spinal Immobilisation, An Initial Consensus StatementDocument4 pagesGuideline Reino Unido - Pre-Hospital Spinal Immobilisation, An Initial Consensus StatementTriz BeaNo ratings yet
- Final ProtocolDocument24 pagesFinal Protocolnayem hossainNo ratings yet
- Hemiarthroplasty For Unstable Intertrochanteric Hip Fractures - A Matched Cohort StudyDocument6 pagesHemiarthroplasty For Unstable Intertrochanteric Hip Fractures - A Matched Cohort StudyNetepPalpatineNo ratings yet
- Treatment of Thoracolumbar FractureDocument14 pagesTreatment of Thoracolumbar FractureLaela LathifatunNo ratings yet
- Classification of Pelvic Fractures and Its Clinical RelevanceDocument6 pagesClassification of Pelvic Fractures and Its Clinical RelevanceMohamed AzeemNo ratings yet
- Diagnosis and Management of Partial Thickness Rotator Cuff Tears_ A Comprehensive ReviewDocument13 pagesDiagnosis and Management of Partial Thickness Rotator Cuff Tears_ A Comprehensive ReviewKarim SabaNo ratings yet
- Surgical Management of Posterior Ligament Complex Stri 2024 International JoDocument5 pagesSurgical Management of Posterior Ligament Complex Stri 2024 International JoRonald QuezadaNo ratings yet
- 1 s2.0 S0020138323006873 MainDocument6 pages1 s2.0 S0020138323006873 MainAliif MaulanaNo ratings yet
- The Influence of Cervical Spondylolisthesis On CliDocument8 pagesThe Influence of Cervical Spondylolisthesis On CliReyhan Diaz SaputraNo ratings yet
- Patients Immobilized With A Long Spine Board Rarely Have Unstable Thoracolumbar InjuriesDocument8 pagesPatients Immobilized With A Long Spine Board Rarely Have Unstable Thoracolumbar InjuriesJade OttoniNo ratings yet
- Distal Femur Fractures. Surgical Techniques and A Review of The LiteratureDocument8 pagesDistal Femur Fractures. Surgical Techniques and A Review of The Literaturerifqi13No ratings yet
- 2.Fx cadera-NEJM 2019Document10 pages2.Fx cadera-NEJM 2019Nico GonzálezNo ratings yet
- Rockwood and Green's Fractures in Adultes: Chapter 37 Scapular FracturesDocument23 pagesRockwood and Green's Fractures in Adultes: Chapter 37 Scapular FracturesPermata GBKP Runggun SurabayaNo ratings yet
- Posterior Shoulder Fracture-Dislocation A SystematDocument7 pagesPosterior Shoulder Fracture-Dislocation A SystematMarcos Burón100% (1)
- Mar2012 CC SkendzelDocument9 pagesMar2012 CC SkendzelJavierLarenasNo ratings yet
- Subaxial Cervical Spine Trauma: Cervical Injuries and Treatment (HJ Kim, Section Editor)Document9 pagesSubaxial Cervical Spine Trauma: Cervical Injuries and Treatment (HJ Kim, Section Editor)renonauvalNo ratings yet
- Periprosthetic Acetabular Fracture PDFDocument9 pagesPeriprosthetic Acetabular Fracture PDFBoz LuNo ratings yet
- Acomparative Study of The Functional Andradiological Outcome of Displaced Mid Shaft Clavicle Fracture Managed With Intramedullary Nailing and PlatingDocument9 pagesAcomparative Study of The Functional Andradiological Outcome of Displaced Mid Shaft Clavicle Fracture Managed With Intramedullary Nailing and PlatingIJAR JOURNALNo ratings yet
- Perumal 2020Document12 pagesPerumal 2020andiNo ratings yet
- Guidelines For The Management of Acute Cervical Spine and SCI 2013Document10 pagesGuidelines For The Management of Acute Cervical Spine and SCI 2013Tâm NguyễnNo ratings yet
- Management of Acute Hip Fracture - NEJM PDFDocument10 pagesManagement of Acute Hip Fracture - NEJM PDFRui ViegasNo ratings yet
- Treatment of Humeral Shaft Fractures: A Critical Analysis ReviewDocument9 pagesTreatment of Humeral Shaft Fractures: A Critical Analysis ReviewRafaelAntonioNarvaezAguirreNo ratings yet
- SMR Resource Document FINAL Publication 6-28-14Document5 pagesSMR Resource Document FINAL Publication 6-28-14Carlos SantosNo ratings yet
- Decision en FX CervicalesDocument7 pagesDecision en FX CervicalesM Joaquin Robles OrtizNo ratings yet
- Biological Plating Osteosynthesis in Comminuted Subtrochanteric Fractures With Dynamic Hip ScrewDocument12 pagesBiological Plating Osteosynthesis in Comminuted Subtrochanteric Fractures With Dynamic Hip ScrewIJAR JOURNALNo ratings yet
- ODONTOIDESDocument11 pagesODONTOIDESElianaNo ratings yet
- Surgical ICU-AWDocument28 pagesSurgical ICU-AWArmi ZakaNo ratings yet
- Proximal Humerus Fractures: Evaluation and ManagementFrom EverandProximal Humerus Fractures: Evaluation and ManagementLynn A. CrosbyNo ratings yet
- Comparative Efficacy of Clindamycin Versus Erythromycin in Eradication of AntenatalDocument7 pagesComparative Efficacy of Clindamycin Versus Erythromycin in Eradication of AntenatalSamuel ManurungNo ratings yet
- EUA 105 Pfizer Paxlovid FS For HCPs (12222021) - 0Document29 pagesEUA 105 Pfizer Paxlovid FS For HCPs (12222021) - 0Samuel ManurungNo ratings yet
- Anemia in Children: Causes, Types and TreatmentDocument61 pagesAnemia in Children: Causes, Types and TreatmentSamuel ManurungNo ratings yet
- WHO 2019 nCoV IHR - Quarantine 2020.3 EngDocument6 pagesWHO 2019 nCoV IHR - Quarantine 2020.3 EngkimNo ratings yet
- TEACHING PLAN FOR Varicose VeinsDocument5 pagesTEACHING PLAN FOR Varicose Veinscertified_maharot_ako2828No ratings yet
- Risk Assessment Matrix (ISO) - 3Document1 pageRisk Assessment Matrix (ISO) - 3Verina GaldasNo ratings yet
- Nursing Care Plan Urinary Tract Infection (UTI)Document2 pagesNursing Care Plan Urinary Tract Infection (UTI)deric95% (97)
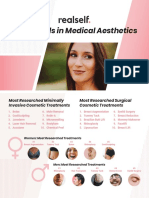
- RealSelf YearInReview OneSheetDocument2 pagesRealSelf YearInReview OneSheetDominico Adityo RaharjoNo ratings yet
- Forensic PathologyDocument3 pagesForensic PathologyjmosserNo ratings yet
- 5 1 1113Document7 pages5 1 1113Adhitya Rizky IsnandyaNo ratings yet
- Mzuzu UniversityDocument4 pagesMzuzu UniversityBamusi ChimwemweNo ratings yet
- Oral & Maxillofacial Surgery Medical Emergencies GuideDocument7 pagesOral & Maxillofacial Surgery Medical Emergencies GuidedrpnnreddyNo ratings yet
- Nursing Care in Clients With General Disturbance inDocument48 pagesNursing Care in Clients With General Disturbance inJADE MAIKHA A. MIERGASNo ratings yet
- Viruses: Serge Stroobandt and Roland StroobandtDocument3 pagesViruses: Serge Stroobandt and Roland StroobandtPuskesmas selongNo ratings yet
- Caso Clinico 5Document5 pagesCaso Clinico 5Manuel IbarraNo ratings yet
- 2020 Vision Without Glasses PDFDocument340 pages2020 Vision Without Glasses PDFJacklynlim Lkc100% (3)
- Intro To HematologyDocument9 pagesIntro To HematologyDayledaniel SorvetoNo ratings yet
- Tattoo AllergyDocument1 pageTattoo Allergyjorgeroca2009No ratings yet
- Rapid HIV Test Detects Antibodies in BloodDocument4 pagesRapid HIV Test Detects Antibodies in Bloodkbl27No ratings yet
- Effects of Correction of Metabolic Acidosis On Blood Urea and Bone Metabolism in Patients With Mild To Moderate Chronic Kidney Disease A ProspectiveDocument7 pagesEffects of Correction of Metabolic Acidosis On Blood Urea and Bone Metabolism in Patients With Mild To Moderate Chronic Kidney Disease A ProspectiveHigh LowNo ratings yet
- Austin Journal of Invitro FertilizationDocument5 pagesAustin Journal of Invitro FertilizationAustin Publishing GroupNo ratings yet
- PankreatitisDocument107 pagesPankreatitisIlmiah BagusNo ratings yet
- Amsa232 PDFDocument4 pagesAmsa232 PDFSunny KumarNo ratings yet
- Knowledge of Chemotherapy and Occupational Safety Measures Among Nurses in Oncology UnitsDocument7 pagesKnowledge of Chemotherapy and Occupational Safety Measures Among Nurses in Oncology UnitsIOM BNSNo ratings yet
- Guidelines For The Management of Severe Traumatic Brain Injury 4th EditionDocument52 pagesGuidelines For The Management of Severe Traumatic Brain Injury 4th EditionAnish H DaveNo ratings yet
- Forensic PsychiatryDocument5 pagesForensic PsychiatrySheba Dan de WiseNo ratings yet
- Intracranial Brain TumorDocument24 pagesIntracranial Brain TumorheruNo ratings yet
- Kelengkapan Tas On Call-NEWDocument11 pagesKelengkapan Tas On Call-NEWqcomsamedicNo ratings yet
- Care of The Older Adult Handouts PrelimsDocument7 pagesCare of The Older Adult Handouts PrelimsAmanda Joy TuizaNo ratings yet
- Case Study On Acute Gastroenteritis and Acid Peptic-2Document15 pagesCase Study On Acute Gastroenteritis and Acid Peptic-2FHAMITHANo ratings yet
- Draping The Client For DeliveryDocument4 pagesDraping The Client For DeliveryKristil Chavez100% (1)
- Pelvic Inflammatory Disease: Dr. Indah Meyliza, M. KesDocument13 pagesPelvic Inflammatory Disease: Dr. Indah Meyliza, M. KesIndah MeylizaNo ratings yet
- The Dangers of Cigarette SmokingDocument6 pagesThe Dangers of Cigarette SmokingEdelmar BenosaNo ratings yet
- Descriptive Study On Malignant Otitis Externa in Diabetic Patients at A Tertiary Care Hospital at MadurandhagamDocument5 pagesDescriptive Study On Malignant Otitis Externa in Diabetic Patients at A Tertiary Care Hospital at MadurandhagamAditya HendraNo ratings yet