You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Barangay Health Care Services Sat - SurveyDocument8 pagesBarangay Health Care Services Sat - SurveyRoxanne L. Jaylo100% (1)
- Expert Consensus On Regenerative Endodontic ProceduresDocument13 pagesExpert Consensus On Regenerative Endodontic Procedures朱嘉琪No ratings yet
- Tilted or Parallel Implant Placement inDocument7 pagesTilted or Parallel Implant Placement in朱嘉琪No ratings yet
- Sis Cho 2011Document8 pagesSis Cho 2011朱嘉琪No ratings yet
- Dental Emergencies Management in COVID-19 Pandemic Peak: A Cohort StudyDocument9 pagesDental Emergencies Management in COVID-19 Pandemic Peak: A Cohort Study朱嘉琪No ratings yet
- PIIS0278239121000033Document8 pagesPIIS0278239121000033朱嘉琪No ratings yet
- Problem Statements - HackathonDocument5 pagesProblem Statements - HackathonmohanapriyamoorthyNo ratings yet
- University of TasmaniaDocument3 pagesUniversity of TasmaniaSleepingstar S.No ratings yet
- Residency Entrance ExaminationDocument3 pagesResidency Entrance Examinationzain zainNo ratings yet
- M3 Natural Law Ethics QuizDocument2 pagesM3 Natural Law Ethics QuizAlbert Dela CruzNo ratings yet
- Tigist BirhanuDocument54 pagesTigist BirhanuBiruk MesfinNo ratings yet
- Reproductive Health Strategic Plan 2007-2011Document109 pagesReproductive Health Strategic Plan 2007-2011Nana Adwoa Animah100% (2)
- Implementing Nursing Strategic Plan for Nursing Information SystemDocument7 pagesImplementing Nursing Strategic Plan for Nursing Information SystemMeiliany UniplaitaNo ratings yet
- India Pharma 2020 - Executive Summary - McKinseyDocument34 pagesIndia Pharma 2020 - Executive Summary - McKinseymaheshvtajaneNo ratings yet
- BPKIHS Nursing Certificate Program Entrance ExamDocument25 pagesBPKIHS Nursing Certificate Program Entrance Exammamannish7902No ratings yet
- 5 6186212241637901144Document72 pages5 6186212241637901144Silver lightNo ratings yet
- Andre SaineDocument4 pagesAndre Sainebuscador0077No ratings yet
- Introduction To The Special Issue On Cognitive-Behavioral Couple TherapyDocument3 pagesIntroduction To The Special Issue On Cognitive-Behavioral Couple TherapyMikey StanleyNo ratings yet
- Chapter 16. Architecture As A Creative Practice For Improving Living Conditions and Social Welfare For Alzheimer S PatientsDocument13 pagesChapter 16. Architecture As A Creative Practice For Improving Living Conditions and Social Welfare For Alzheimer S PatientsNishana ShajahanNo ratings yet
- For Prescribers - New Limits On Prescription Opioids For Acute PainDocument2 pagesFor Prescribers - New Limits On Prescription Opioids For Acute PainKyle HuaNo ratings yet
- Contact Us TableDocument10 pagesContact Us Tabletodd7547No ratings yet
- Dental FormDocument22 pagesDental FormJhon Niño BaguioNo ratings yet
- NHM Nagpur Recruitment 2022Document5 pagesNHM Nagpur Recruitment 2022Bappasaheb PanditNo ratings yet
- Drug and Cosmetic ActDocument6 pagesDrug and Cosmetic ActShelly BadialaNo ratings yet
- Health ArticleDocument2 pagesHealth ArticleJayson Gabriel ProtacioNo ratings yet
- Victoria F. StevensonDocument1 pageVictoria F. Stevensonapi-481977583No ratings yet
- ENDOCRINODocument14 pagesENDOCRINOreogomezNo ratings yet
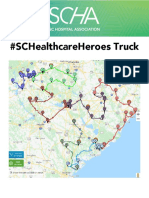
- SCHA SC Healthcare Heroes Truck Map 2020Document14 pagesSCHA SC Healthcare Heroes Truck Map 2020WIS NewsNo ratings yet
- CMC Vellore Guide History Facilities Services Departments MapDocument75 pagesCMC Vellore Guide History Facilities Services Departments MapSanjay Kumar SekhardeoNo ratings yet
- ICE Checklist #4: Cleaning and Disinfection of The Dialysis StationDocument1 pageICE Checklist #4: Cleaning and Disinfection of The Dialysis StationAbidi Hichem100% (2)
- Policy - Medical ExamDocument1 pagePolicy - Medical ExamEmma De La LunaNo ratings yet
- Nle NPDocument4 pagesNle NPHamad KristinNo ratings yet
- Integration of Nursing Informatics, Nursing Classification Systems, and Nursing Practice (Nur 603)Document56 pagesIntegration of Nursing Informatics, Nursing Classification Systems, and Nursing Practice (Nur 603)Topsider123No ratings yet
- How Devolution Has Shaped Health Financing in the PhilippinesDocument8 pagesHow Devolution Has Shaped Health Financing in the PhilippinesMaria Eufemia C YapNo ratings yet
- Megan Frano Current ResumeDocument1 pageMegan Frano Current Resumeapi-544878035No ratings yet