You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (842)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5806)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- How To Make HydroxychloroquineDocument2 pagesHow To Make HydroxychloroquineSue100% (2)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Tummo EssenceDocument7 pagesTummo EssenceJose AssuncaoNo ratings yet
- Periop TestsDocument13 pagesPeriop TestsJohn Lyndon SayongNo ratings yet
- User HF59R RollscanDocument37 pagesUser HF59R RollscanWiden Carreño50% (2)
- Robert W. Schrier - Atlas of Diseases of The Kidney Volume 01 PDFDocument316 pagesRobert W. Schrier - Atlas of Diseases of The Kidney Volume 01 PDFAtu Oana100% (3)
- Sample of mkt202 ProjectDocument16 pagesSample of mkt202 ProjectMohammad Sohan Khan 2121426630No ratings yet
- Harga KhususDocument16 pagesHarga KhususNoperitaNo ratings yet
- EFFECTS OF ALUGBATI (Basella Alba) On The Growth Performance of Mallard DuckDocument7 pagesEFFECTS OF ALUGBATI (Basella Alba) On The Growth Performance of Mallard DuckCyLo PatricioNo ratings yet
- Pentavitin - DSMDocument3 pagesPentavitin - DSMRnD Roi SuryaNo ratings yet
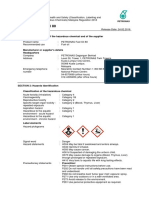
- PETRONAS Fuel Oil 80: Safety Data SheetDocument10 pagesPETRONAS Fuel Oil 80: Safety Data SheetJaharudin JuhanNo ratings yet
- T27208AQCDocument1 pageT27208AQCpiagiopersempreNo ratings yet
- Dry Lab Exercise 4 EndocrineDocument4 pagesDry Lab Exercise 4 Endocrine06Fajrian RidhatunnisaNo ratings yet
- Sleep Scale From The Medical Outcomes StudyDocument2 pagesSleep Scale From The Medical Outcomes StudyAbdullah TheNo ratings yet
- Tackling Addiction: From Belfast To Lisbon: An In-Depth InsightDocument32 pagesTackling Addiction: From Belfast To Lisbon: An In-Depth InsightSonia EstevesNo ratings yet
- Med OfficeDocument7 pagesMed OfficeAllana Millizenth C. LabasanNo ratings yet
- Psychosexual Stages of Development: Sigmund FreudDocument15 pagesPsychosexual Stages of Development: Sigmund FreudSmera NathaniNo ratings yet
- Chapter 22: The Thyroid Gland: by Marissa Grotzke, Dev AbrahamDocument21 pagesChapter 22: The Thyroid Gland: by Marissa Grotzke, Dev AbrahamJanielle FajardoNo ratings yet
- Pengaruh Senam Rematik Terhadap Skala Nyeri: Rheumatoid Arthritis Pada LansiaDocument7 pagesPengaruh Senam Rematik Terhadap Skala Nyeri: Rheumatoid Arthritis Pada LansiaDinaliza UtamiNo ratings yet
- School of Medical Sciences Kathmandu UniversityDocument6 pagesSchool of Medical Sciences Kathmandu Universitysuyog raj gautamNo ratings yet
- Gov. Youngkin's Final Budget Presentation Dec 15Document21 pagesGov. Youngkin's Final Budget Presentation Dec 15ABC7NewsNo ratings yet
- Spiritual CareDocument7 pagesSpiritual CareSyarief NurseNo ratings yet
- High Blood Pressure and DiabetesDocument4 pagesHigh Blood Pressure and DiabetesNizam HasniNo ratings yet
- 12 Lead Ecg Application FormDocument2 pages12 Lead Ecg Application Formmuzammil1No ratings yet
- Hospital Managment Unit 3Document62 pagesHospital Managment Unit 3seemantham123No ratings yet
- 7A Detailed Lesson Plan in Health 7 I. Content Standard: Teacher's Activity Students' ActivityDocument10 pages7A Detailed Lesson Plan in Health 7 I. Content Standard: Teacher's Activity Students' ActivityLeizel C. LeonidoNo ratings yet
- IGen Book ReviewDocument6 pagesIGen Book ReviewPedro RamosNo ratings yet
- Notice of Post DisqualificationDocument3 pagesNotice of Post DisqualificationMelody Frac ZapateroNo ratings yet
- New Grad Banner Cover Letter RevisedDocument1 pageNew Grad Banner Cover Letter Revisedapi-621660715No ratings yet
- LVL G-01 Sheet 1 of 6 - Drainage - Detail 2 SheetDocument1 pageLVL G-01 Sheet 1 of 6 - Drainage - Detail 2 SheetRajasekaran GunasekaranNo ratings yet
- NICU PPT Hypo and HyperthermiaDocument23 pagesNICU PPT Hypo and HyperthermiaelsawzgoodNo ratings yet