You might also like
- Substandard Neostigmindr Misal FinalDocument12 pagesSubstandard Neostigmindr Misal FinalusmisalNo ratings yet
- Convulsive Seizures With A Therapeutic Dose of Isoniazid: Case ReportDocument4 pagesConvulsive Seizures With A Therapeutic Dose of Isoniazid: Case ReportSeptira MurtiningsihNo ratings yet
- PracticeExam 2 QsDocument24 pagesPracticeExam 2 QsBehrouz YariNo ratings yet
- Adrenal Insufficiency: Grand RoundsDocument8 pagesAdrenal Insufficiency: Grand RoundsindahNo ratings yet
- 2018 Article 1648Document5 pages2018 Article 1648Dewi NurfadilahNo ratings yet
- Anafilactic ShockDocument2 pagesAnafilactic ShockprayogarathaNo ratings yet
- Topic 10 Internal Medicine Ali SaifDocument5 pagesTopic 10 Internal Medicine Ali SaifAnkit Kumar PatelNo ratings yet
- The American Board of Anesthesiology Practice Examination QuestionsDocument24 pagesThe American Board of Anesthesiology Practice Examination QuestionschossNo ratings yet
- Laporan Kasus Hipertensi Pulmonal-Ridha MardhatillahDocument3 pagesLaporan Kasus Hipertensi Pulmonal-Ridha MardhatillahAtunNo ratings yet
- Critical Illness Related Corticosteroid Insufficiency (CIRCI) - 1Document35 pagesCritical Illness Related Corticosteroid Insufficiency (CIRCI) - 1nathanaellee92No ratings yet
- When Past Is Prologue: Clinical Problem-SolvingDocument7 pagesWhen Past Is Prologue: Clinical Problem-SolvingJoni WitziNo ratings yet
- Transient Acute Decompensated Heart Failure Following Propofol and Fentanyl Administration in A Healthy 19-Year-Old PatientDocument2 pagesTransient Acute Decompensated Heart Failure Following Propofol and Fentanyl Administration in A Healthy 19-Year-Old PatientAchmad Ageng SeloNo ratings yet
- Ajmcr 10 9 10Document4 pagesAjmcr 10 9 10saNo ratings yet
- 00003Document8 pages00003Anonymous zPwXqwNo ratings yet
- Novi Terapijski Koncepti U Postresuscitacionom Lečenju: New Therapeutic Concepts in Post Resuscitation CareDocument5 pagesNovi Terapijski Koncepti U Postresuscitacionom Lečenju: New Therapeutic Concepts in Post Resuscitation CareMarija LazarevicNo ratings yet
- CCMDocument28 pagesCCMSwati Pathak GiriNo ratings yet
- Jurnal Blok 10Document3 pagesJurnal Blok 10Yunus Lumban RajaNo ratings yet
- Overdose and Cardiovascular In: Quinidine Jneurological Toxicity NormalDocument3 pagesOverdose and Cardiovascular In: Quinidine Jneurological Toxicity NormalNika QuinagonNo ratings yet
- Case ChallangeDocument11 pagesCase ChallangeAltaNo ratings yet
- Primary Aldosteronism Caused by Unilateral Adrenal Hyperplasia: Rethinking The Accuracy of Imaging StudiesDocument5 pagesPrimary Aldosteronism Caused by Unilateral Adrenal Hyperplasia: Rethinking The Accuracy of Imaging StudiesRonald DelosendoNo ratings yet
- Cardiopulmonary ResuscitationDocument3 pagesCardiopulmonary Resuscitationmerida_elinorNo ratings yet
- ESC Guidelines Implementation in Indonesian HospitalDocument7 pagesESC Guidelines Implementation in Indonesian HospitalJeffri GunawanNo ratings yet
- 10 Relato de Caso Acute CoronaryDocument4 pages10 Relato de Caso Acute CoronaryAsis FitrianaNo ratings yet
- Tutor PDFDocument10 pagesTutor PDFAlifia RahmiNo ratings yet
- Case 1 - Widuri - His Bundle Pacing in TAVBDocument17 pagesCase 1 - Widuri - His Bundle Pacing in TAVBW Wita SNo ratings yet
- Review Article: Review and Outcome of Prolonged Cardiopulmonary ResuscitationDocument9 pagesReview Article: Review and Outcome of Prolonged Cardiopulmonary Resuscitation28121998No ratings yet
- Diabetes InsipidusDocument5 pagesDiabetes InsipidusrchristevenNo ratings yet
- Massive Pulmonary Embolism Presenting As Seizures: December 2008 Vol 10 No 4Document4 pagesMassive Pulmonary Embolism Presenting As Seizures: December 2008 Vol 10 No 4BelladonnaRoxNo ratings yet
- Try Out NewDocument19 pagesTry Out NewIke AdrianaNo ratings yet
- Seronegative Myasthenia Gravis Presenting With PneumoniaDocument4 pagesSeronegative Myasthenia Gravis Presenting With PneumoniaJ. Ruben HermannNo ratings yet
- Articulo 6 FarmacoDocument8 pagesArticulo 6 FarmacoLiz Espinoza ZambranoNo ratings yet
- Soal Juni Beserta KunciDocument76 pagesSoal Juni Beserta Kuncirsiamb100% (1)
- Aortic dissection CT findings pathophysiologyDocument44 pagesAortic dissection CT findings pathophysiologyRoni ArmandaNo ratings yet
- Brain Injury Resuscitation 2009Document8 pagesBrain Injury Resuscitation 2009Dandy Azmi AzwirNo ratings yet
- Assessment of Pulse Transit Time To Indicate Cardiovascular Changes During Obstetric Spinal AnaesthesiaDocument6 pagesAssessment of Pulse Transit Time To Indicate Cardiovascular Changes During Obstetric Spinal AnaesthesiaprabuNo ratings yet
- Case Study On Critical CareDocument6 pagesCase Study On Critical CareJude Micko Bunyi AlipitNo ratings yet
- ModMed CardiologyDocument77 pagesModMed CardiologyLee Tzong YewNo ratings yet
- Emergency Management of Acute Myocardial Infarction: Simon MaxwellDocument15 pagesEmergency Management of Acute Myocardial Infarction: Simon MaxwellMaram AbdullahNo ratings yet
- A Pain in The Butt - A Case Series of Gluteal Compartment Syndrome - PMCDocument6 pagesA Pain in The Butt - A Case Series of Gluteal Compartment Syndrome - PMCchhabraanNo ratings yet
- Case History 33Document4 pagesCase History 33Hida KurticNo ratings yet
- Efficacy of Hyperventilation, Blood Pressure Elevation, and Metabolic Suppression Therapy in Controlling Intracranial Pressure After Head InjuryDocument9 pagesEfficacy of Hyperventilation, Blood Pressure Elevation, and Metabolic Suppression Therapy in Controlling Intracranial Pressure After Head InjuryAik NoeraNo ratings yet
- ClonidineDocument4 pagesClonidineDR RAVI ANANDNo ratings yet
- Upgrade Primary Care FNP Review 1250 TermsDocument7 pagesUpgrade Primary Care FNP Review 1250 TermsNEsreNo ratings yet
- DrHSMurthy HiPECDocument11 pagesDrHSMurthy HiPECReddyNo ratings yet
- PracticeExam 3 QsDocument17 pagesPracticeExam 3 QsBehrouz YariNo ratings yet
- Board Review: Nephrology: Wednesday, August 19Document65 pagesBoard Review: Nephrology: Wednesday, August 19Lina Abuarqoub67% (3)
- International Journal of Neurology and Neurotherapy Ijnn 2 030Document2 pagesInternational Journal of Neurology and Neurotherapy Ijnn 2 030Anis Rita PratiwiNo ratings yet
- Patient Diagnosed With Myocardial Infarct M006Document11 pagesPatient Diagnosed With Myocardial Infarct M006Kefix WritersHubNo ratings yet
- ENLS - V 4.0 Protocol - ICH - FinalDocument16 pagesENLS - V 4.0 Protocol - ICH - FinalR.M.C vivNo ratings yet
- Cardiovascular Medicine Questions: Risk Assessment, Heart Failure, Chest Pain, PalpitationsDocument102 pagesCardiovascular Medicine Questions: Risk Assessment, Heart Failure, Chest Pain, PalpitationsManisha DesaiNo ratings yet
- 2014 CCM Review Notes Jon-Emile S. Kenny M.D, 2014Document142 pages2014 CCM Review Notes Jon-Emile S. Kenny M.D, 2014PkernNo ratings yet
- Cardiovascular Medicine:Question 1Document101 pagesCardiovascular Medicine:Question 1abdullahmushlihNo ratings yet
- Globulin Thyroid Dialy-: TherapyDocument5 pagesGlobulin Thyroid Dialy-: TherapyNurdita KartikaNo ratings yet
- Acute Cardiac CareDocument42 pagesAcute Cardiac CareMarwa Elsayed Abuelnour100% (1)
- Cardiovascular Disease Case StudiesDocument6 pagesCardiovascular Disease Case StudiesShanica Paul-RichardsNo ratings yet
- Asymptomatic Aplastic Anemia Case Due to Anti-TB DrugsDocument4 pagesAsymptomatic Aplastic Anemia Case Due to Anti-TB DrugsayuNo ratings yet
- Case Study For Colon CancerDocument2 pagesCase Study For Colon Cancerrhimineecat7150% (2)
- Last Minute CPSDocument11 pagesLast Minute CPSnob2011nobNo ratings yet
- Vt900a User ManualDocument58 pagesVt900a User ManualdcgNo ratings yet
- Experience and RecollectionDocument316 pagesExperience and RecollectionPeter AgabaNo ratings yet
- Zampieri 2019Document8 pagesZampieri 2019Peter AgabaNo ratings yet
- Fluidos e Hipertonicos Neurocrit CareDocument5 pagesFluidos e Hipertonicos Neurocrit CareMiguelAngelEspinalLendofNo ratings yet
- Fluid Assessment by SonographyDocument58 pagesFluid Assessment by SonographyPeter AgabaNo ratings yet
- FCEM (SA) - Part - I - Past - Papers 4Document4 pagesFCEM (SA) - Part - I - Past - Papers 4matentenNo ratings yet
- Albumin Administration in The Acutely Ill: What Is New and Where Next?Document10 pagesAlbumin Administration in The Acutely Ill: What Is New and Where Next?Peter AgabaNo ratings yet
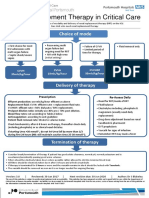
- Renal Replacement Therapy in Critical Care: Choice of ModeDocument15 pagesRenal Replacement Therapy in Critical Care: Choice of ModePeter AgabaNo ratings yet
- 2015 Resident ManualDocument850 pages2015 Resident ManualPeter AgabaNo ratings yet
- Receive Weekly Emails on Phantom Limb PainDocument7 pagesReceive Weekly Emails on Phantom Limb PainPeter AgabaNo ratings yet
- 321 Difficult Mask VentilationDocument7 pages321 Difficult Mask VentilationFajar SatriaNo ratings yet
- Sign up for weekly anaesthesia tutorial emailDocument8 pagesSign up for weekly anaesthesia tutorial emailAli AftabNo ratings yet
- 171 Vapour Is at Ion and VapourisersDocument9 pages171 Vapour Is at Ion and Vapourisersdrvinodg2000No ratings yet
- Educ 580 - Edpuzzle PD HandoutDocument3 pagesEduc 580 - Edpuzzle PD Handoutapi-548868233No ratings yet
- Strategic Management and Municipal Financial ReportingDocument38 pagesStrategic Management and Municipal Financial ReportingMarius BuysNo ratings yet
- List of Trigonometric IdentitiesDocument16 pagesList of Trigonometric IdentitiesArnab NandiNo ratings yet
- tmp82D3 TMPDocument12 pagestmp82D3 TMPFrontiersNo ratings yet
- Research Trends On Environmental Energy and Vulnerability - 2021 - Energy andDocument27 pagesResearch Trends On Environmental Energy and Vulnerability - 2021 - Energy andCynthia Mac-beathNo ratings yet
- Quiz - Limits and ContinuityDocument3 pagesQuiz - Limits and ContinuityAdamNo ratings yet
- Telangana Energy Dept Contact NumbersDocument27 pagesTelangana Energy Dept Contact Numbersstarpowerzloans rjyNo ratings yet
- Large Generators WEBDocument16 pagesLarge Generators WEBMaycon MaranNo ratings yet
- Manhole bill of materialsDocument1 pageManhole bill of materialsjalNo ratings yet
- SKM 4 - COCU - CU2 - Child - Care - Centre - HealthDocument14 pagesSKM 4 - COCU - CU2 - Child - Care - Centre - HealthShireen TahirNo ratings yet
- Effects of UrbanizationDocument17 pagesEffects of UrbanizationAriel EstigoyNo ratings yet
- ALGEBRA Groups 1Document34 pagesALGEBRA Groups 1bravemacnyNo ratings yet
- Diosdado MacapagalDocument13 pagesDiosdado MacapagalMermie ArmentaNo ratings yet
- Age Hardening Gold Alloys For JewelryDocument4 pagesAge Hardening Gold Alloys For JewelryReinol Eko SianturiNo ratings yet
- Understanding Income Statements EPS CalculationsDocument39 pagesUnderstanding Income Statements EPS CalculationsKeshav KaplushNo ratings yet
- Danh sách KH Biệt Thự Thảo Điền - Quận 2Document4 pagesDanh sách KH Biệt Thự Thảo Điền - Quận 2La TraNo ratings yet
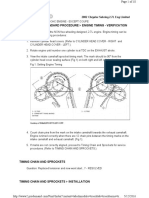
- 02+sebring+2.7+timing+chainDocument10 pages02+sebring+2.7+timing+chainMaushil Salman MarkNo ratings yet
- Improve Product Packaging at Annual Board MeetingDocument9 pagesImprove Product Packaging at Annual Board Meetingizzat89% (9)
- Familiarization With Apparatus and Equipment Used in Testing of MaterialsDocument5 pagesFamiliarization With Apparatus and Equipment Used in Testing of MaterialsEmanoAce33% (6)
- Falling Weight Deflectometer (FWD) Projects in IndiaDocument13 pagesFalling Weight Deflectometer (FWD) Projects in IndiaKaran Dave100% (1)
- January 2011Document64 pagesJanuary 2011sake1978No ratings yet
- Quantitative Data Analysis 2Document10 pagesQuantitative Data Analysis 2Rhona MaandalNo ratings yet
- ACP Programs ListDocument3 pagesACP Programs ListShreeya BhatNo ratings yet
- Audit Chapter 7Document5 pagesAudit Chapter 7Addi Såïñt George100% (2)
- Inv 069 1701757527Document1 pageInv 069 1701757527neetu9414576916No ratings yet
- Literature Review On Waste Management in NigeriaDocument9 pagesLiterature Review On Waste Management in NigeriajzneaqwgfNo ratings yet
- Bismillah Skripsi Herlina Rozaaaa-1Document57 pagesBismillah Skripsi Herlina Rozaaaa-1Saidi NetNo ratings yet
- OTISLINE QuestionsDocument5 pagesOTISLINE QuestionsArvind Gupta100% (1)
- 6 Thinking Hats Detailed Model - UpdatedDocument32 pages6 Thinking Hats Detailed Model - Updatedgeetanshi mittalNo ratings yet
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (14)
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (402)
- Techniques Exercises And Tricks For Memory ImprovementFrom EverandTechniques Exercises And Tricks For Memory ImprovementRating: 4.5 out of 5 stars4.5/5 (40)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 3.5 out of 5 stars3.5/5 (3)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeNo ratings yet
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 3.5 out of 5 stars3.5/5 (2)
- The Ultimate Guide To Memory Improvement TechniquesFrom EverandThe Ultimate Guide To Memory Improvement TechniquesRating: 5 out of 5 stars5/5 (34)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (78)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsRating: 5 out of 5 stars5/5 (1)
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 5 out of 5 stars5/5 (4)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsFrom EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo ratings yet
- The Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsFrom EverandThe Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsNo ratings yet
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsFrom EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsRating: 4.5 out of 5 stars4.5/5 (169)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingFrom EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingRating: 3.5 out of 5 stars3.5/5 (33)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisFrom EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisRating: 4.5 out of 5 stars4.5/5 (42)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeFrom EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeRating: 4.5 out of 5 stars4.5/5 (253)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisFrom EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (1)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessFrom EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessRating: 4.5 out of 5 stars4.5/5 (327)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.From EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Rating: 4.5 out of 5 stars4.5/5 (110)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingFrom EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingRating: 5 out of 5 stars5/5 (5)
- The Happiness Trap: How to Stop Struggling and Start LivingFrom EverandThe Happiness Trap: How to Stop Struggling and Start LivingRating: 4 out of 5 stars4/5 (1)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryFrom EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryRating: 4 out of 5 stars4/5 (44)
- Summary: It Didn't Start with You: How Inherited Family Trauma Shapes Who We Are and How to End the Cycle By Mark Wolynn: Key Takeaways, Summary & AnalysisFrom EverandSummary: It Didn't Start with You: How Inherited Family Trauma Shapes Who We Are and How to End the Cycle By Mark Wolynn: Key Takeaways, Summary & AnalysisRating: 5 out of 5 stars5/5 (3)