You might also like
- Physiologic Basis For Hemodynamic MonitoringDocument36 pagesPhysiologic Basis For Hemodynamic MonitoringEshwar Chandra VidyasagarNo ratings yet
- Clinical Review - Update On Hemodynamic Monitoring - A Consensus of 16 - PMCDocument15 pagesClinical Review - Update On Hemodynamic Monitoring - A Consensus of 16 - PMCV ANo ratings yet
- Haemodynamic Monitoring With Pulse-Induced Contour Cardiac Output (PiCCO) in Critical CareDocument7 pagesHaemodynamic Monitoring With Pulse-Induced Contour Cardiac Output (PiCCO) in Critical CareClaudia IsabelNo ratings yet
- Hemodynamic MonitoringDocument65 pagesHemodynamic MonitoringrrthamadNo ratings yet
- 05.monitoring Hemodinamik AG SHANGRILLA SBY 2018Document65 pages05.monitoring Hemodinamik AG SHANGRILLA SBY 2018syafeiNo ratings yet
- Picco Technology Clinical Evidence Brochure en Non - UsDocument25 pagesPicco Technology Clinical Evidence Brochure en Non - UsRichard DaiNo ratings yet
- IraposopemidososDocument9 pagesIraposopemidososjoseNo ratings yet
- Evaluate My LungDocument57 pagesEvaluate My LungSantosNo ratings yet
- Bedside Preload Assessment CVP, PLR and USG Guided JCCA Bali 2016Document36 pagesBedside Preload Assessment CVP, PLR and USG Guided JCCA Bali 2016Ari YudhaNo ratings yet
- 9 - Role of Non InvasiveDocument46 pages9 - Role of Non InvasiveHavara Kausar AkbarNo ratings yet
- Inferior Vena Cava Diameter and Collapsibility IndexDocument9 pagesInferior Vena Cava Diameter and Collapsibility IndexmalisalukmanNo ratings yet
- PhysioFlow Non Invasive Hemodynamic Monitoring GeneralDocument28 pagesPhysioFlow Non Invasive Hemodynamic Monitoring GeneralPritam HiraNo ratings yet
- Wu 2018Document8 pagesWu 2018Karel ZertucheNo ratings yet
- Cardiogenic Shock: Updated Approach To ManagementDocument49 pagesCardiogenic Shock: Updated Approach To ManagementelsarahmiNo ratings yet
- Advance in Haemodynamic Monitoring CompressedDocument66 pagesAdvance in Haemodynamic Monitoring Compressedmeta ikaNo ratings yet
- Non Invasive Cardiac Output MonitoringDocument69 pagesNon Invasive Cardiac Output MonitoringAlexNo ratings yet
- Webinar1 Presentation HMforNEXTDocument130 pagesWebinar1 Presentation HMforNEXTAdrian BălanNo ratings yet
- Ron Pi CCODocument28 pagesRon Pi CCOroonnie2017No ratings yet
- How To Perform Left Ventricular Assistance in The CathlabDocument104 pagesHow To Perform Left Ventricular Assistance in The CathlabUmar UsmanNo ratings yet
- Emergency MedicineDocument28 pagesEmergency Medicineshilpa sekhar278No ratings yet
- Wjem 23 358Document10 pagesWjem 23 358drsubramanianNo ratings yet
- Principles of Continuous Renal Replacement Therapy For AkiDocument43 pagesPrinciples of Continuous Renal Replacement Therapy For AkiFelicia Risca RyandiniNo ratings yet
- Fluid-Responsiveness: An ICU Phoenix: Darryl Stewart Regional ICM Study Day 07/11/2013 Altnagelvin Area HospitalDocument29 pagesFluid-Responsiveness: An ICU Phoenix: Darryl Stewart Regional ICM Study Day 07/11/2013 Altnagelvin Area HospitalAnnushika PalanichamyNo ratings yet
- 01 - ICON Englisch WebDocument4 pages01 - ICON Englisch WebaldyNo ratings yet
- Clinical Case February 14 2024 Isis Daniela RojasDocument23 pagesClinical Case February 14 2024 Isis Daniela Rojasapi-725651063No ratings yet
- Coronary Angiography and AngioplastyDocument24 pagesCoronary Angiography and AngioplastySemina Gazepi100% (2)
- Central Venous Pressure (CVP)Document27 pagesCentral Venous Pressure (CVP)Danial Hassan100% (1)
- Angina PostprandialDocument10 pagesAngina PostprandialJoaquín SosaNo ratings yet
- The PCQP Score For Volume Status of Acutely Ill Patients - Integrating Vascular Pedicle Width, Caval Index, Respiratory Variability of The QRS Complex and R Wave AmplitudeDocument8 pagesThe PCQP Score For Volume Status of Acutely Ill Patients - Integrating Vascular Pedicle Width, Caval Index, Respiratory Variability of The QRS Complex and R Wave AmplitudeSoftwarebolivia EnriqueNo ratings yet
- Cardiogenic Shock: Look, Listen and Treat Class Code: 220: Intra-Aortic Balloon CounterpulsationDocument30 pagesCardiogenic Shock: Look, Listen and Treat Class Code: 220: Intra-Aortic Balloon CounterpulsationSlaviša KovačevićNo ratings yet
- Baker 2013Document6 pagesBaker 2013Moni-k GuarnerosNo ratings yet
- Effects of AlirocumabDocument32 pagesEffects of Alirocumabsoleiman.ariaNo ratings yet
- 10 1378@chest 09-2690Document9 pages10 1378@chest 09-2690Alvaro Andres Flores JimenezNo ratings yet
- 4.massive HemorrhageDocument44 pages4.massive HemorrhageyeabsraNo ratings yet
- Antiplatelet and Anticoagulation Regimen in Patients WithDocument30 pagesAntiplatelet and Anticoagulation Regimen in Patients Withfelipe duarteNo ratings yet
- HD Moniroriz Reviw 2023Document17 pagesHD Moniroriz Reviw 2023DanaNo ratings yet
- Share RateDocument26 pagesShare Ratevirtualpop3No ratings yet
- Effects of Cardiopulmonary Bypass On Mediastinal Drainage and The Use of Blood Products in The Intensive Care Unit in 60-To 80-Year-Old Patients Who Have Undergone Coronary Artery Bypass GraftingDocument8 pagesEffects of Cardiopulmonary Bypass On Mediastinal Drainage and The Use of Blood Products in The Intensive Care Unit in 60-To 80-Year-Old Patients Who Have Undergone Coronary Artery Bypass GraftingYogi TrilaksonoNo ratings yet
- Transpulmonary Dilution Methods GHALEBDocument49 pagesTranspulmonary Dilution Methods GHALEBGHALEB A. AlmekhlafiNo ratings yet
- Advance in Haemodynamic Monitoring CompressedDocument72 pagesAdvance in Haemodynamic Monitoring CompressedMuh Irfan YusnurliantoNo ratings yet
- Hasanin 2021Document8 pagesHasanin 2021Ammon10famNo ratings yet
- Materi - Advanced HFDocument34 pagesMateri - Advanced HFPutra AchmadNo ratings yet
- Platelet CountsDocument35 pagesPlatelet Countsshikhar623No ratings yet
- Unit II (B) Intra-Aortic Balloon Pump Counter PulsationDocument24 pagesUnit II (B) Intra-Aortic Balloon Pump Counter PulsationUmme HabibaNo ratings yet
- Fluid Management in HFDocument47 pagesFluid Management in HFPandu AnggoroNo ratings yet
- Bai 7 - BS Hien - HirrtDocument28 pagesBai 7 - BS Hien - HirrtTấn Phát NguyễnNo ratings yet
- Fluid Resuscitation and Volume Assessment: - Does This Patient Have Adequate Organ Perfusion?Document24 pagesFluid Resuscitation and Volume Assessment: - Does This Patient Have Adequate Organ Perfusion?RichardNo ratings yet
- Laparoscopy Morbid ThyroidDocument155 pagesLaparoscopy Morbid ThyroidparuNo ratings yet
- Anesthesia Considerations During Cytoreductive SurDocument9 pagesAnesthesia Considerations During Cytoreductive Surdrardigustian2986No ratings yet
- Hypertensive Vascular DiseaseDocument61 pagesHypertensive Vascular DiseaseFedelyn Mae AcaylarNo ratings yet
- Prosedur Diagnostik KardiovaskulerDocument43 pagesProsedur Diagnostik Kardiovaskulernurrahmi auliaNo ratings yet
- 0256 Version 2019Document66 pages0256 Version 2019vanessa armeliaNo ratings yet
- What Is New in Microcirculation and Tissue Oxygenation Monitoring?Document9 pagesWhat Is New in Microcirculation and Tissue Oxygenation Monitoring?evernotegeniusNo ratings yet
- Sepsis Update 2019Document44 pagesSepsis Update 2019Yeshwanth Umapathi100% (1)
- Mechanical Ventilation: Weaning From Mechanical Ventilation Kathia Ortiz-Cantillo, MDDocument25 pagesMechanical Ventilation: Weaning From Mechanical Ventilation Kathia Ortiz-Cantillo, MDsarevNo ratings yet
- Update On Hemodynamic MonitoringDocument66 pagesUpdate On Hemodynamic Monitoringl1o2stNo ratings yet
- Which Echocardiographic Parameter Is A Better Marker of Volume Status in Hemodialysis PatientsDocument7 pagesWhich Echocardiographic Parameter Is A Better Marker of Volume Status in Hemodialysis PatientsmalisalukmanNo ratings yet
- Clinical Case February 21 2024 Isis Daniela RojasDocument24 pagesClinical Case February 21 2024 Isis Daniela Rojasapi-725651063No ratings yet
- Monitor Bedside BSM-3000 SeriesDocument8 pagesMonitor Bedside BSM-3000 SeriesDouglas Gaitan PotosmeNo ratings yet
- Experience and RecollectionDocument316 pagesExperience and RecollectionPeter AgabaNo ratings yet
- Zampieri 2019Document8 pagesZampieri 2019Peter AgabaNo ratings yet
- Albumin Administration in The Acutely Ill: What Is New and Where Next?Document10 pagesAlbumin Administration in The Acutely Ill: What Is New and Where Next?Peter AgabaNo ratings yet
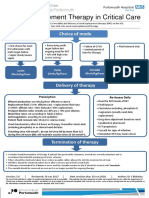
- Renal Replacement Therapy in Critical Care: Choice of ModeDocument15 pagesRenal Replacement Therapy in Critical Care: Choice of ModePeter AgabaNo ratings yet
- 2015 Resident ManualDocument850 pages2015 Resident ManualPeter AgabaNo ratings yet
- Peri-Operative Cardiac Arrest Secondary To Adrenal InsufficiencyDocument3 pagesPeri-Operative Cardiac Arrest Secondary To Adrenal InsufficiencyPeter AgabaNo ratings yet
- Phantom Limb Pain Anaesthesia Tutorial of The Week 229 27 JUNE 2011Document7 pagesPhantom Limb Pain Anaesthesia Tutorial of The Week 229 27 JUNE 2011Peter AgabaNo ratings yet
- Inferior Vena Cava Diameter and Collapsibility IndexDocument9 pagesInferior Vena Cava Diameter and Collapsibility IndexmalisalukmanNo ratings yet
- Dr. Abdul Rashad Senior Lecturer DPT, Mphill (Opt), Mppta, MMTC (NZ), MSTC (Aus), Iastm (Greece) United College of Physical TherapyDocument41 pagesDr. Abdul Rashad Senior Lecturer DPT, Mphill (Opt), Mppta, MMTC (NZ), MSTC (Aus), Iastm (Greece) United College of Physical TherapypashaNo ratings yet
- Radiology of The RetroperitoneumDocument4 pagesRadiology of The RetroperitoneumHugo FreitasNo ratings yet
- Abd AortaDocument48 pagesAbd AortaSanjib NepramNo ratings yet
- Prof. Ghabisha Saif Posterior Abdominal Wall AnatomyDocument36 pagesProf. Ghabisha Saif Posterior Abdominal Wall AnatomyAzizNo ratings yet
- Circulatory System TurtleDocument32 pagesCirculatory System TurtleVillamorchardNo ratings yet
- Assessment of The Heart and Neck VesselsDocument25 pagesAssessment of The Heart and Neck VesselsCuenca LanceNo ratings yet
- Rsik of ICH in Anticoagulation Primary Brain Tumor PatientDocument7 pagesRsik of ICH in Anticoagulation Primary Brain Tumor PatientFithry RahmaNo ratings yet
- DMV Cipe Di AtriaDocument6 pagesDMV Cipe Di AtriaAngélica ContrerasNo ratings yet
- EMRCS Abdomin AnatomyDocument54 pagesEMRCS Abdomin AnatomyShakirNo ratings yet
- Vi. Anatomy and Physiology: Anatomical Structures and Physiology of The Affected Body Organ/ SystemsDocument18 pagesVi. Anatomy and Physiology: Anatomical Structures and Physiology of The Affected Body Organ/ SystemsZhailyn Joy DumlaoNo ratings yet
- Angiology: Sanqiang Pan Department of Anatomy Medical College of Jinan UniversityDocument34 pagesAngiology: Sanqiang Pan Department of Anatomy Medical College of Jinan UniversityKw ChanNo ratings yet
- Monitoreo Hemodinamico Funcional PinskyDocument23 pagesMonitoreo Hemodinamico Funcional PinskyJuan CarrascoNo ratings yet
- Heldt (2013) - Chapter 2 Mathematical Modeling of Physiological SystemsDocument21 pagesHeldt (2013) - Chapter 2 Mathematical Modeling of Physiological SystemsVint PineNo ratings yet
- Vascular Technology Content OutlineDocument5 pagesVascular Technology Content OutlineJing CruzNo ratings yet
- Umbilical Catheterization in ServiceDocument11 pagesUmbilical Catheterization in ServiceLucian CaelumNo ratings yet
- Tsktccts 8800 Plus EngDocument13 pagesTsktccts 8800 Plus EngRandom ProjectNo ratings yet
- Artifacts in Diagnostic UltrasoundDocument20 pagesArtifacts in Diagnostic UltrasoundFranciscoNo ratings yet
- NBME 19 ExplanationsDocument96 pagesNBME 19 Explanationsmed student100% (2)
- BCS InterventionDocument14 pagesBCS InterventiondrrochanNo ratings yet
- Med SurgDocument4 pagesMed SurgGeraldine MaeNo ratings yet
- Revision Notes On FRCRDocument385 pagesRevision Notes On FRCRObaidy Albushaher100% (2)
- Atlas of Endovascular Venous Surgery 2Nd Ed Edition Almeida Full ChapterDocument67 pagesAtlas of Endovascular Venous Surgery 2Nd Ed Edition Almeida Full Chaptergreg.vasquez490100% (7)
- Ivc FilterDocument15 pagesIvc FilterashishNo ratings yet
- Renal Cell Carcinoma: Diagnosis, Staging, and SurveillanceDocument18 pagesRenal Cell Carcinoma: Diagnosis, Staging, and SurveillanceMutia IsanaNo ratings yet
- Urologic Principles and Practice 2nd EditionDocument692 pagesUrologic Principles and Practice 2nd EditionRonuve RonuveNo ratings yet
- Acodaduras Ureterales (Kinking)Document7 pagesAcodaduras Ureterales (Kinking)Clínica CIPRONo ratings yet
- Stephen Hobbs - Thoracic Imaging - A Core Review-Lippincott Williams & Wilkins (2015)Document564 pagesStephen Hobbs - Thoracic Imaging - A Core Review-Lippincott Williams & Wilkins (2015)hüseyin vururNo ratings yet
- Comparative Circulatory SystemDocument15 pagesComparative Circulatory SystemSmartcool SoNo ratings yet
- Anatomy of The LiverDocument34 pagesAnatomy of The LiverOmiko Fidelis NnamdiNo ratings yet