You might also like
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Marfan'sDocument39 pagesMarfan'sRavin DebieNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Tachycardia Algorithm 2021Document1 pageTachycardia Algorithm 2021Ravin DebieNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Sepsis Quick Reference GuideDocument1 pageSepsis Quick Reference GuideRavin DebieNo ratings yet
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- IJC Heart & VasculatureDocument7 pagesIJC Heart & VasculatureRavin DebieNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Atrial Fibrillation: Management Atrial Fibrillation: ManagementDocument47 pagesAtrial Fibrillation: Management Atrial Fibrillation: ManagementRavin DebieNo ratings yet
- Aorticemergencies: Kathleen WittelsDocument12 pagesAorticemergencies: Kathleen WittelsRavin DebieNo ratings yet
- Filbin 2019Document7 pagesFilbin 2019Ravin DebieNo ratings yet
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Case Report Euglycaemic DkaDocument4 pagesCase Report Euglycaemic DkaRavin DebieNo ratings yet
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Diagnosis and Management of Acute Gastroenteritis in The Emergency DepartmentDocument24 pagesDiagnosis and Management of Acute Gastroenteritis in The Emergency DepartmentRavin Debie100% (1)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Immune Related Adverse EventsDocument11 pagesImmune Related Adverse EventsRavin DebieNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Basic Epidemiology (E-Book)Document226 pagesBasic Epidemiology (E-Book)Ing Ching100% (12)
- High Alert-Long Term Care SettingDocument1 pageHigh Alert-Long Term Care SettingRuuNataNo ratings yet
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- General PharmacologyDocument32 pagesGeneral PharmacologyAlphahin 17No ratings yet
- Chapter 1. Intro To DrugsDocument10 pagesChapter 1. Intro To DrugsLyka Milo AvilaNo ratings yet
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Drug Interactions of Veterinary Importance With Reference To Fluid TherapyDocument29 pagesDrug Interactions of Veterinary Importance With Reference To Fluid TherapySunil67% (3)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Practice Drug CalculationsDocument11 pagesPractice Drug Calculationskijeramustapha23No ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Modes of Mechanical VentilationDocument4 pagesModes of Mechanical VentilationDuy ThanhNo ratings yet
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Pharmaceutical Equivalence of Generic Essential DrugsDocument15 pagesPharmaceutical Equivalence of Generic Essential DrugsLiiz PinedaNo ratings yet
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Phytopharmaceuticals - A New Drug Class Regulated in IndiaDocument3 pagesPhytopharmaceuticals - A New Drug Class Regulated in IndiaHadrian Sjah RazadNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Bali Spa Overseas Prices Update1Document5 pagesBali Spa Overseas Prices Update1Dian WijayantiNo ratings yet
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Metformin GlucophageDocument2 pagesMetformin GlucophageCassie100% (4)
- Web Marketed 20220408Document494 pagesWeb Marketed 20220408Darwiche DarwicheNo ratings yet
- Usmani 2021 AerosphereDocument12 pagesUsmani 2021 AerosphereRadu CiprianNo ratings yet
- Drug-Induced Memory DisordersDocument1 pageDrug-Induced Memory DisordersNeeru KaulNo ratings yet
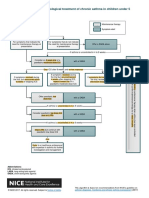
- Algorithm D: Pharmacological Treatment of Chronic Asthma in Children Under 5Document1 pageAlgorithm D: Pharmacological Treatment of Chronic Asthma in Children Under 5samNo ratings yet
- The Role of The Pharmacist in The Control of Acute PoisoningDocument6 pagesThe Role of The Pharmacist in The Control of Acute PoisoningJayrine MonteroNo ratings yet
- Prescription Insert: Unit 20 PresentationDocument31 pagesPrescription Insert: Unit 20 PresentationQuang HuyNo ratings yet
- Editorial: History PharmacokineticsDocument2 pagesEditorial: History PharmacokineticsvladymirNo ratings yet
- Chart FastingDocument1 pageChart FastingGary S75% (4)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Format Rko 2024Document44 pagesFormat Rko 2024Muhammad_Azzam_BNo ratings yet
- Iqvia Institute Global Oncology Trends 2022 ForwebDocument65 pagesIqvia Institute Global Oncology Trends 2022 ForwebYefinadya MfNo ratings yet
- Wound Care ManagementDocument32 pagesWound Care ManagementEko JatiNo ratings yet
- Raphael Sevilla, PT, DPT: Student Physical TherapistDocument1 pageRaphael Sevilla, PT, DPT: Student Physical TherapistRaphael SevillaNo ratings yet
- Glyburide (Glibenclamide) : Drug Information: Brand Names: USDocument17 pagesGlyburide (Glibenclamide) : Drug Information: Brand Names: USAnonymous wmF9p2ejNo ratings yet
- Fortified Drops Chart A4 Modified 1pdfpdf 2Document1 pageFortified Drops Chart A4 Modified 1pdfpdf 2Rubén SepúlvedaNo ratings yet
- Daftar Obat IGD Dan Poli UmumDocument2 pagesDaftar Obat IGD Dan Poli UmumPku Aisyiyah JeparaNo ratings yet
- Naranjo AlgorithmDocument3 pagesNaranjo AlgorithmmilkymilkyNo ratings yet
- Diphenhydramine AHFSDocument18 pagesDiphenhydramine AHFSDymas PrayogaNo ratings yet
- Methods of Detoxification and Their Role in Treating Patients With Opioid DependenceDocument3 pagesMethods of Detoxification and Their Role in Treating Patients With Opioid DependenceAndy PurnomoNo ratings yet
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- VasopressinDocument3 pagesVasopressinChristian Dave EndinoNo ratings yet
- Anticonvulsant Quiz AnswersDocument26 pagesAnticonvulsant Quiz AnswersRammy KhanNo ratings yet