You might also like
- Preventive Pediatrics 2016Document48 pagesPreventive Pediatrics 2016riz04_fortitudessa5178100% (9)
- Evidence-Based Public HealthDocument312 pagesEvidence-Based Public Healthnaravichandran3662100% (1)
- SSIE Homework 2 FinalDocument9 pagesSSIE Homework 2 FinalStephen WattNo ratings yet
- Interpretative Phenomenological AnalysisDocument28 pagesInterpretative Phenomenological AnalysisbexibexNo ratings yet
- UST Medicine I Schedule 2016-2017Document6 pagesUST Medicine I Schedule 2016-2017ina17_eaglerNo ratings yet
- Considerations For Ethics Review of Big Data Health Research: A Scoping ReviewDocument15 pagesConsiderations For Ethics Review of Big Data Health Research: A Scoping Reviewalemayehu badargaNo ratings yet
- Primary Health Care Literature ReviewDocument4 pagesPrimary Health Care Literature Reviewafdtbluwq100% (1)
- Information Needs and Sources of Information Among People With Depression and Anxiety: A Scoping ReviewDocument18 pagesInformation Needs and Sources of Information Among People With Depression and Anxiety: A Scoping ReviewVince MartinezNo ratings yet
- Evaluation of Flowsheet Documentation in The Electronic Health Record For Residence, Living Situation, and Living ConditionsDocument10 pagesEvaluation of Flowsheet Documentation in The Electronic Health Record For Residence, Living Situation, and Living Conditionsxcr66123No ratings yet
- 2013-Evidence Based Public HealthDocument15 pages2013-Evidence Based Public HealthEric Yesaya TanNo ratings yet
- Ocab 194Document9 pagesOcab 194xcr66123No ratings yet
- Representation of People S Decisions in Health Information SystemsDocument7 pagesRepresentation of People S Decisions in Health Information Systemsadriana.dawidowskiNo ratings yet
- Research in Health and Social Care - EditedDocument8 pagesResearch in Health and Social Care - EditedJannat ButtNo ratings yet
- HIS Lesson 5 - Health Informatics SystemDocument6 pagesHIS Lesson 5 - Health Informatics SystemHans Kimberly V. DavidNo ratings yet
- 1-S2.0-S2590229620300149-Main PT 4Document11 pages1-S2.0-S2590229620300149-Main PT 4Ridania CahyanegaraNo ratings yet
- Evidence-Based Public HealthDocument312 pagesEvidence-Based Public HealthBudi Lamaka100% (7)
- Lippincott Williams & WilkinsDocument12 pagesLippincott Williams & WilkinsZeno MunteanuNo ratings yet
- Health Information Seeking Behaviors Linked to HealthDocument6 pagesHealth Information Seeking Behaviors Linked to HealthC. R. PintoNo ratings yet
- Clinincal Decision Support SystemDocument10 pagesClinincal Decision Support Systemم. سهير عبد داؤد عسىNo ratings yet
- Dietary Ingredients as an Alternative Approach for Mitigating Chronic Musculoskeletal PainDocument12 pagesDietary Ingredients as an Alternative Approach for Mitigating Chronic Musculoskeletal PainThiago NylanderNo ratings yet
- Recommender Systems in The Healthcare Domain: State-Of-The-Art and Research IssuesDocument31 pagesRecommender Systems in The Healthcare Domain: State-Of-The-Art and Research IssuesJohn DoeNo ratings yet
- Doing Health Policy and Systems Research: Key Steps in The ProcessDocument20 pagesDoing Health Policy and Systems Research: Key Steps in The ProcessBelyaNo ratings yet
- Munro 2007Document17 pagesMunro 2007Jose RodriguezNo ratings yet
- Add 2Document15 pagesAdd 2diana.alyNo ratings yet
- Young Adults' Health Perceptions, Behaviors and Info SeekingDocument19 pagesYoung Adults' Health Perceptions, Behaviors and Info SeekingKITTIVONGSAK VONGSUTHEP KEITHNo ratings yet
- Hand Out - 2 Case Study + Elements of Strong JustificationDocument4 pagesHand Out - 2 Case Study + Elements of Strong JustificationasmexNo ratings yet
- Raghupathi-Raghupathi2014 Article BigDataAnalyticsInHealthcarePr PDFDocument10 pagesRaghupathi-Raghupathi2014 Article BigDataAnalyticsInHealthcarePr PDFCristian ZapataNo ratings yet
- 2017 Article 474Document15 pages2017 Article 474Rity Ames GuerreroNo ratings yet
- Health Affairs: For Reprints, Links & Permissions: E-Mail Alerts: To SubscribeDocument12 pagesHealth Affairs: For Reprints, Links & Permissions: E-Mail Alerts: To Subscribedheng05No ratings yet
- This Content Downloaded From 196.191.53.146 On Wed, 20 Jul 2022 06:06:21 UTCDocument5 pagesThis Content Downloaded From 196.191.53.146 On Wed, 20 Jul 2022 06:06:21 UTCAdane AbateNo ratings yet
- Public Health ResearchDocument34 pagesPublic Health ResearchPhong TrầnNo ratings yet
- Week 1 1Document8 pagesWeek 1 1R-jeyn TorresNo ratings yet
- iDSI Reference CaseDocument8 pagesiDSI Reference CaseZurNo ratings yet
- E-Mental HealthDocument9 pagesE-Mental HealthNabina Sharma JhaNo ratings yet
- Joint Statistical Meetings - Section On Health Policy Statistics (HPSS)Document5 pagesJoint Statistical Meetings - Section On Health Policy Statistics (HPSS)Lativa FauzaniNo ratings yet
- Gesundheitswesen Hta Kosten Nutzen Key Principles 2008 0Document15 pagesGesundheitswesen Hta Kosten Nutzen Key Principles 2008 0Stavros TheodoridisNo ratings yet
- Userdocs Documents Oct 2015Document9 pagesUserdocs Documents Oct 2015BrandonNo ratings yet
- Public Health Dissertation TitlesDocument7 pagesPublic Health Dissertation TitlesWriteMyPaperPleaseSingapore100% (1)
- A Machine Learning Approach For Identifying Disease-Treatment Relations in Short TextsDocument14 pagesA Machine Learning Approach For Identifying Disease-Treatment Relations in Short TextsShubhamNo ratings yet
- Oxman Et Al-2019-BMC Medical Informatics and Decision MakingDocument17 pagesOxman Et Al-2019-BMC Medical Informatics and Decision MakingsalemNo ratings yet
- Patient System Chapter 1Document4 pagesPatient System Chapter 1Ayinde AbiodunNo ratings yet
- Role of Health Surveys in National Health Information Systems: Best-Use ScenariosDocument28 pagesRole of Health Surveys in National Health Information Systems: Best-Use ScenariosazfarNo ratings yet
- Student's Copy - LESSON 2 Health Information SystemDocument4 pagesStudent's Copy - LESSON 2 Health Information SystemDOMILE, SAMANTHA RIANNENo ratings yet
- Online Healthcare Management SystemDocument4 pagesOnline Healthcare Management SystemAyinde AbiodunNo ratings yet
- (JURNAL, Eng) Reducing Potentially Inappropriate Prescriptions For Older Patients Using Computerized Decision Support Tools, Systematic ReviewDocument20 pages(JURNAL, Eng) Reducing Potentially Inappropriate Prescriptions For Older Patients Using Computerized Decision Support Tools, Systematic ReviewAurellia Annisa WulandariNo ratings yet
- The Role of Digital Health in Supporting Cancer PatientsDocument19 pagesThe Role of Digital Health in Supporting Cancer PatientsEduardoNo ratings yet
- The Role of Digital Health in Supporting Cancer Patients-1-8Document8 pagesThe Role of Digital Health in Supporting Cancer Patients-1-8EduardoNo ratings yet
- Eur J Clin Investigation - 2017 - Ioannidis - How To Survive The Medical Misinformation MessDocument8 pagesEur J Clin Investigation - 2017 - Ioannidis - How To Survive The Medical Misinformation MessPanosNo ratings yet
- Evidence-Based Health Policy: A Preliminary Systematic ReviewDocument5 pagesEvidence-Based Health Policy: A Preliminary Systematic ReviewAndre LanzerNo ratings yet
- Health Care Provider Adoption of Ehealth: Systematic Literature ReviewDocument19 pagesHealth Care Provider Adoption of Ehealth: Systematic Literature ReviewMaryamNo ratings yet
- Digital Drugs An Anatomy of New Medicines PDFDocument27 pagesDigital Drugs An Anatomy of New Medicines PDFshraddha5jNo ratings yet
- 1 19 Tech Assess ArticleDocument9 pages1 19 Tech Assess ArticleAmgad AlsisiNo ratings yet
- 07-Health Information and Biostatistics: November 2016Document32 pages07-Health Information and Biostatistics: November 2016Marium TNo ratings yet
- Barriers To The Evidence-Based Patient Choice (EBPC) Vs EBM. Paper Study. Evidence Based Medicine Interest.Document7 pagesBarriers To The Evidence-Based Patient Choice (EBPC) Vs EBM. Paper Study. Evidence Based Medicine Interest.Lourdes Fernandez CabreraNo ratings yet
- Effectiveness of Manual Therapies The UKDocument33 pagesEffectiveness of Manual Therapies The UKSimao GigiNo ratings yet
- Rating Satisfaction Research - Is It Poor, Fair, Good, Very Good, or Excellent - PDFDocument9 pagesRating Satisfaction Research - Is It Poor, Fair, Good, Very Good, or Excellent - PDFAr LynNo ratings yet
- Introduction To EIDMDocument45 pagesIntroduction To EIDMShahab UddinNo ratings yet
- Patient Engagement in Research: A Systematic Review: Researcharticle Open AccessDocument9 pagesPatient Engagement in Research: A Systematic Review: Researcharticle Open Accessv_ratNo ratings yet
- Data Driven Health Informatics Digital LDocument125 pagesData Driven Health Informatics Digital Lnarkhajid NEMUT100% (1)
- 02 01 Methodologies Realizing Potential Hia 2005Document8 pages02 01 Methodologies Realizing Potential Hia 2005Lidwina Margaretha LakaNo ratings yet
- 404 03 Mentalhealth ES ENGDocument9 pages404 03 Mentalhealth ES ENGritanlanskyNo ratings yet
- PublicDocument12 pagesPublicJayapriya jayaramanNo ratings yet
- Ethics, Qualitative And Quantitative Methods In Public Health ResearchFrom EverandEthics, Qualitative And Quantitative Methods In Public Health ResearchNo ratings yet
- IMRADDocument2 pagesIMRADDon Chiaw ManongdoNo ratings yet
- Capstone Project FormatDocument6 pagesCapstone Project FormatDon Chiaw ManongdoNo ratings yet
- Health Information ManagementDocument29 pagesHealth Information ManagementDon Chiaw Manongdo100% (1)
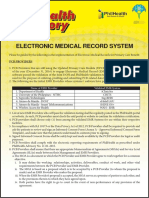
- EMRsDocument2 pagesEMRsDon Chiaw ManongdoNo ratings yet
- Nursing Research Methodology NotesDocument83 pagesNursing Research Methodology NotesDon Chiaw ManongdoNo ratings yet
- APA Referencing SummaryDocument18 pagesAPA Referencing SummaryDon Chiaw ManongdoNo ratings yet
- Employee InvolvementDocument29 pagesEmployee InvolvementAimee BerbaNo ratings yet
- TAIZENDocument16 pagesTAIZENNavneet SoniNo ratings yet
- References: Some More Basic Reference Page RulesDocument13 pagesReferences: Some More Basic Reference Page RulesDon Chiaw ManongdoNo ratings yet
- History of Total Quality ManagementDocument3 pagesHistory of Total Quality ManagementDon Chiaw ManongdoNo ratings yet
- Design Thinking Learning ToolDocument2 pagesDesign Thinking Learning ToolDon Chiaw ManongdoNo ratings yet
- TQMDocument16 pagesTQMHARITHA MADHUNo ratings yet
- The Health Promotion ModelDocument8 pagesThe Health Promotion ModelDon Chiaw Manongdo100% (1)
- Strategic Quality Planning GuideDocument10 pagesStrategic Quality Planning GuideDon Chiaw ManongdoNo ratings yet
- Reflections On Theory DevelopmentDocument3 pagesReflections On Theory DevelopmentDon Chiaw ManongdoNo ratings yet
- Filipino TheoristsDocument55 pagesFilipino TheoristsDon Chiaw Manongdo100% (5)
- Uv-Irb Pocedure Flowrevised 81417Document11 pagesUv-Irb Pocedure Flowrevised 81417Don Chiaw ManongdoNo ratings yet
- Notes On PhenomenologyDocument5 pagesNotes On PhenomenologyDon Chiaw ManongdoNo ratings yet
- The Case Study WayDocument30 pagesThe Case Study WayDon Chiaw ManongdoNo ratings yet
- Single Case Study Vs Multiple Case StudyDocument15 pagesSingle Case Study Vs Multiple Case StudyElvin Michaels100% (1)
- Health Promotion Model By: Nola J. Pender: Presented By: Mila MaruyaDocument24 pagesHealth Promotion Model By: Nola J. Pender: Presented By: Mila MaruyaDon Chiaw Manongdo100% (1)
- Uv-Irb Pocedure Flowrevised 81417Document6 pagesUv-Irb Pocedure Flowrevised 81417api-222431624No ratings yet
- Employee Retention Chapter 1 To 2Document30 pagesEmployee Retention Chapter 1 To 2Don Chiaw Manongdo100% (1)
- Narayan Kafle. Hermeneutic Phenomenological Research MethodDocument20 pagesNarayan Kafle. Hermeneutic Phenomenological Research MethodMhel Es QuiadNo ratings yet
- Narayan Kafle. Hermeneutic Phenomenological Research MethodDocument20 pagesNarayan Kafle. Hermeneutic Phenomenological Research MethodMhel Es QuiadNo ratings yet
- Related LiteratureDocument22 pagesRelated LiteratureDon Chiaw ManongdoNo ratings yet
- Review of Resubmitted Study Protocol FormDocument1 pageReview of Resubmitted Study Protocol FormDon Chiaw ManongdoNo ratings yet
- Case Study ResearchDocument8 pagesCase Study ResearchDon Chiaw ManongdoNo ratings yet
- Case Study FormatDocument6 pagesCase Study Formatjlhynn0% (1)
- Dwyer, AE (2016) - Oftalmología Práctica de Campo. Oftalmología Equina, 72-111.Document40 pagesDwyer, AE (2016) - Oftalmología Práctica de Campo. Oftalmología Equina, 72-111.Francisco JulianNo ratings yet
- Physical AssessmentDocument5 pagesPhysical AssessmentROGEN KATE AZARCONNo ratings yet
- Pre Employment Medical Check Up Form MalaysiaDocument3 pagesPre Employment Medical Check Up Form MalaysiaAmiraNo ratings yet
- Advances in The Diagnosis and Treatment of Extremity Vascular TraumaDocument17 pagesAdvances in The Diagnosis and Treatment of Extremity Vascular TraumaMerlin MuktialiNo ratings yet
- Practice Advisory For Preanesthesia Evaluation. An Updated Report by The American Society of Anesthesiologists Task Force On PreanesthesiaDocument12 pagesPractice Advisory For Preanesthesia Evaluation. An Updated Report by The American Society of Anesthesiologists Task Force On PreanesthesiaMadalina TalpauNo ratings yet
- NullDocument123 pagesNullARLibraryNo ratings yet
- Preschool Health Assessment FormDocument2 pagesPreschool Health Assessment FormSammi GuptaNo ratings yet
- Twelve Tips For Organizing An Objective Structured Clinical Examination (OSCE)Document6 pagesTwelve Tips For Organizing An Objective Structured Clinical Examination (OSCE)Anonymous wGAc8DYl3VNo ratings yet
- BACHELOR IN NURSING - Docx (Reflection)Document9 pagesBACHELOR IN NURSING - Docx (Reflection)siti husniNo ratings yet
- CPRS Handbook - 2023-2024 - 20240110Document94 pagesCPRS Handbook - 2023-2024 - 20240110kongchiyui000medNo ratings yet
- BREAST SELF EXA-WPS OfficeDocument16 pagesBREAST SELF EXA-WPS OfficeEra khanNo ratings yet
- Lesson Plan ON Seek Health Services For Routine Health Checkups, Immunization, Counseling, Diagnosis, Treatment, Follow UpDocument33 pagesLesson Plan ON Seek Health Services For Routine Health Checkups, Immunization, Counseling, Diagnosis, Treatment, Follow Uprevathidadam55555No ratings yet
- AMLS Provider Course ObjDocument5 pagesAMLS Provider Course ObjJim ThorntonNo ratings yet
- The Problem Oriented Medical RecordDocument3 pagesThe Problem Oriented Medical RecordPia Angelica DizonNo ratings yet
- LIC Rates List: Sr. No Descrition of Tests PSP RatesDocument5 pagesLIC Rates List: Sr. No Descrition of Tests PSP RatesLALIT MUNDENo ratings yet
- Kujdesi Antenatal - Anglisht (Per Web) 02Document53 pagesKujdesi Antenatal - Anglisht (Per Web) 02UNICEF KosovoNo ratings yet
- OSPE vs TPE: A Comparison of Objective Structured Practical Examination and Traditional Practical ExaminationDocument27 pagesOSPE vs TPE: A Comparison of Objective Structured Practical Examination and Traditional Practical Examinationsapna chauhan100% (1)
- COMSEP ProblemSetDocument29 pagesCOMSEP ProblemSettasha2gNo ratings yet
- Consultation Station Notes 20220919Document161 pagesConsultation Station Notes 20220919Jonathan TayNo ratings yet
- Assessment ReassessmentDocument2 pagesAssessment ReassessmentsunitapuniaNo ratings yet
- NURSFPX 4060 Assessment 4Document1 pageNURSFPX 4060 Assessment 4Adam JonesNo ratings yet
- Barangay Cabalaoangan Citizen's Charter ServicesDocument14 pagesBarangay Cabalaoangan Citizen's Charter Servicesdesiree joy corpuz100% (3)
- Nursing Assessment and Physical ExaminationDocument5 pagesNursing Assessment and Physical ExaminationTaufik Rohman0% (1)
- Mini Clinical Examination (Mini-CEX)Document21 pagesMini Clinical Examination (Mini-CEX)Jeffrey Dyer100% (1)
- Physical AssessmentDocument30 pagesPhysical AssessmentZanie CruzNo ratings yet
- Medical Examination Rules 2005Document12 pagesMedical Examination Rules 2005MutuajmNo ratings yet
- Fon Mcqs Whole BookDocument38 pagesFon Mcqs Whole BookRizwan EjazNo ratings yet