You might also like
- Nontuberculous Mycobacteria (NTM): Microbiological, Clinical and Geographical DistributionFrom EverandNontuberculous Mycobacteria (NTM): Microbiological, Clinical and Geographical DistributionNo ratings yet
- Study of Antibiotic-Resistance and Sensitivity Pattern in A Tertiary Care Teaching HospitalDocument8 pagesStudy of Antibiotic-Resistance and Sensitivity Pattern in A Tertiary Care Teaching HospitalIJAR JOURNALNo ratings yet
- Hospital Management: Bacterial InfectionDocument21 pagesHospital Management: Bacterial Infectionapadanainst7372No ratings yet
- Antimicrobial Sensitivity Pattern in The Mixed Intensive Care Unit in A Tertiary Care Hospital of Eastern NepalDocument7 pagesAntimicrobial Sensitivity Pattern in The Mixed Intensive Care Unit in A Tertiary Care Hospital of Eastern NepalNilisha PradhanNo ratings yet
- Document 4Document9 pagesDocument 4นันทสิทธิ์ ศิริวิชญ์ไมตรีNo ratings yet
- Emergence of Multidrug Resistant Acinetobacter Baumannii As Nosocomial Pathogen: Clinical Significance and Antimicrobial SensitivityDocument5 pagesEmergence of Multidrug Resistant Acinetobacter Baumannii As Nosocomial Pathogen: Clinical Significance and Antimicrobial SensitivityIOSRjournalNo ratings yet
- The Foot: Original ArticleDocument5 pagesThe Foot: Original ArticleKarinaayu SerinNo ratings yet
- Current Senerio of Antimicrobial Resistance Patterns of Pseudomonas Aeruginosa Clinical Isolates in East Uttar Pradesh, IndiaDocument4 pagesCurrent Senerio of Antimicrobial Resistance Patterns of Pseudomonas Aeruginosa Clinical Isolates in East Uttar Pradesh, IndiaPraveen GautamNo ratings yet
- Bacteriological Profile and Drug Susceptibility Patterns in Dacryocystitis Patients Attending Gondar University Teaching Hospital, Northwest EthiopiaDocument17 pagesBacteriological Profile and Drug Susceptibility Patterns in Dacryocystitis Patients Attending Gondar University Teaching Hospital, Northwest EthiopiaDaisa RosianaNo ratings yet
- Accepted ManuscriptDocument23 pagesAccepted ManuscriptMrcom HvqyNo ratings yet
- Multiple Colony Antifungal Susceptibility Testing Detects PolyresistanceDocument7 pagesMultiple Colony Antifungal Susceptibility Testing Detects PolyresistanceZaenab AzzahraNo ratings yet
- Bacteria Found in UrineDocument7 pagesBacteria Found in UrineAria DomingoNo ratings yet
- Zahedan J Res Med Sci 2012 14 8 74 76Document3 pagesZahedan J Res Med Sci 2012 14 8 74 76yudhit bessieNo ratings yet
- Antibiotic Susceptibility Patterns of Methicillin Resistant Staphyl - PDF NIHDocument5 pagesAntibiotic Susceptibility Patterns of Methicillin Resistant Staphyl - PDF NIHzia ul RahmanNo ratings yet
- Antibiogram of Gram Negative Uropathogens in A TerDocument5 pagesAntibiogram of Gram Negative Uropathogens in A TerDumitraNo ratings yet
- What's New in Antimicrobial Susceptibility Testing?: Dilution MIC Test Broth DilutionDocument3 pagesWhat's New in Antimicrobial Susceptibility Testing?: Dilution MIC Test Broth DilutionViswanathan AnanthanarayananNo ratings yet
- Dont KnowDocument5 pagesDont KnownawarajNo ratings yet
- Journal of Clinical Immunology and MicrobiologyDocument10 pagesJournal of Clinical Immunology and MicrobiologyAthenaeum Scientific PublishersNo ratings yet
- Jurnal Kedokteran Dan Kesehatan IndonesiaDocument7 pagesJurnal Kedokteran Dan Kesehatan IndonesiaReffy AdhaNo ratings yet
- Drug Resistance and Plasmid Profile of Uropathogenic Escherichia Coli Among Urinary Tract Infection Patients in Addis AbebaDocument8 pagesDrug Resistance and Plasmid Profile of Uropathogenic Escherichia Coli Among Urinary Tract Infection Patients in Addis AbebaOm ParkashNo ratings yet
- Jurnal Mikro 1Document6 pagesJurnal Mikro 1Elang SudewaNo ratings yet
- Clinico-Microbiological Study of Pyodermas: Research Article Janardhan. B, Prasad - GK, Nandeshwar - AJ and Vidyavathi.NDocument5 pagesClinico-Microbiological Study of Pyodermas: Research Article Janardhan. B, Prasad - GK, Nandeshwar - AJ and Vidyavathi.NradiNo ratings yet
- Gevher Nesibe Journal of Medical & Health SciencesDocument8 pagesGevher Nesibe Journal of Medical & Health SciencesTrengginas AjiNo ratings yet
- Clinical Spectrum and Antibiogram of Acinetobacter Infections in Children Study From A Tertiary Care Centre, IndiaDocument12 pagesClinical Spectrum and Antibiogram of Acinetobacter Infections in Children Study From A Tertiary Care Centre, IndiaInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Children KantiDocument5 pagesChildren KantiPiyush AcharyaNo ratings yet
- Antibiotic Sensitivity Pattern of Gram Negative BaDocument4 pagesAntibiotic Sensitivity Pattern of Gram Negative BaRaffaharianggaraNo ratings yet
- Paper02 Jan2012Document5 pagesPaper02 Jan2012Bharani ChanderNo ratings yet
- Multidrug Resistant Uropathogens in Urinary Tract Infections and Their Antibiotic Susceptibility PatternsDocument4 pagesMultidrug Resistant Uropathogens in Urinary Tract Infections and Their Antibiotic Susceptibility PatternsCERCEL ALESIA IOANANo ratings yet
- Antibiotic Resistance Pattern in Pseudomonas Aeruginosa Species Isolated at A Tertiary Care Hospital, AhmadabadDocument4 pagesAntibiotic Resistance Pattern in Pseudomonas Aeruginosa Species Isolated at A Tertiary Care Hospital, AhmadabadDrashua AshuaNo ratings yet
- Conquering Methicillin Resistant Staphylococcus Aureus: Perspectives and Treatment OptionsDocument7 pagesConquering Methicillin Resistant Staphylococcus Aureus: Perspectives and Treatment OptionsInternational Medical PublisherNo ratings yet
- Antimicrobial Resistance Patterns Among Acinetobacter Baumannii Isolated From Burn Intensive Care Unit in Tripoli, LibyDocument5 pagesAntimicrobial Resistance Patterns Among Acinetobacter Baumannii Isolated From Burn Intensive Care Unit in Tripoli, LibyInternational Medical PublisherNo ratings yet
- Isolation and Characterization of Actinomycetes From Soil and Evaluation of Antibacterial Activities of Actinomycetes Against PathogensDocument9 pagesIsolation and Characterization of Actinomycetes From Soil and Evaluation of Antibacterial Activities of Actinomycetes Against PathogensTrương Tấn SangNo ratings yet
- Jurnal Interna 123456Document9 pagesJurnal Interna 123456vonnyandira28No ratings yet
- Antimicrobial Susceptibility Testing - Primer For CliniciansDocument20 pagesAntimicrobial Susceptibility Testing - Primer For Cliniciansdipzhit100% (1)
- Susceptibility of Gram-Positive Cocci From 25 UK Hospitals To Antimicrobial Agents Including LinezolidDocument0 pagesSusceptibility of Gram-Positive Cocci From 25 UK Hospitals To Antimicrobial Agents Including LinezolidGabriel MataNo ratings yet
- Antimicrobial Resistance of Escherichia Coli IsolaDocument10 pagesAntimicrobial Resistance of Escherichia Coli IsolaRaffaharianggaraNo ratings yet
- Use and Quality of Point-Of-Care Microscopy Urine Culture and Susceptibility Testing For Urinalysis in General PracticeDocument9 pagesUse and Quality of Point-Of-Care Microscopy Urine Culture and Susceptibility Testing For Urinalysis in General Practicemicrobehunter007No ratings yet
- Risk Profile and Antimicrobial Susceptibility Pattern of Acinetobacter Baumanniiclinical Isolates in A Teaching Hospital in HyderabadDocument8 pagesRisk Profile and Antimicrobial Susceptibility Pattern of Acinetobacter Baumanniiclinical Isolates in A Teaching Hospital in HyderabadIJAR JOURNALNo ratings yet
- EwswsawnDocument5 pagesEwswsawnProbioticsAnywhereNo ratings yet
- Bacteriological Profile and Antibiotic Sensitivity Pattern of Clinical Isolates in A Tertiary Cancer Care Center in The Northeast IndiaDocument5 pagesBacteriological Profile and Antibiotic Sensitivity Pattern of Clinical Isolates in A Tertiary Cancer Care Center in The Northeast IndiaAtul Kumar GoyalNo ratings yet
- In Vitro Susceptibility of Four Antimicrobials AgaDocument8 pagesIn Vitro Susceptibility of Four Antimicrobials Agathanh ba matNo ratings yet
- HJNHNNDocument9 pagesHJNHNNProbioticsAnywhereNo ratings yet
- Prevalence of Methicillinresistant Staphylococcus Aureus Andor Intermediate Susceptibility To Vancomycin Isolated From PDocument7 pagesPrevalence of Methicillinresistant Staphylococcus Aureus Andor Intermediate Susceptibility To Vancomycin Isolated From Pعالمي الجميلNo ratings yet
- Assessment of Susceptibility To Five Common Antibiotics and Their Resistance Pattern in Clinical Enterococcus IsolatesDocument10 pagesAssessment of Susceptibility To Five Common Antibiotics and Their Resistance Pattern in Clinical Enterococcus IsolatesIsidora NikolicNo ratings yet
- Prevalence and Antimicrobial Resistance Pattern of Methicillin Resistant Staphylococcus Aureus (MRSA) Strains..Document7 pagesPrevalence and Antimicrobial Resistance Pattern of Methicillin Resistant Staphylococcus Aureus (MRSA) Strains..Andi EsSeNo ratings yet
- Shalamar Medical & Dental College, Lahore: Research TopicDocument12 pagesShalamar Medical & Dental College, Lahore: Research Topicdr ibtahajNo ratings yet
- Prevalence of Multidrug Resistance in Enterococci Isolates From Different Clinical Sources in Al-Diwaniyah CityDocument9 pagesPrevalence of Multidrug Resistance in Enterococci Isolates From Different Clinical Sources in Al-Diwaniyah CityCentral Asian StudiesNo ratings yet
- Masyeni S Et Al 2018 - Antimicrobial Susceptibility Pattern of Pathogens Isolated From Various Specimens in Denpasar-BaliDocument10 pagesMasyeni S Et Al 2018 - Antimicrobial Susceptibility Pattern of Pathogens Isolated From Various Specimens in Denpasar-BaliGilbert LazarusNo ratings yet
- Gastric Acid SuppressionDocument11 pagesGastric Acid SuppressionRizki AmeliaNo ratings yet
- Title: Culture and Sensitivity Pattern of Urinary Tract Infection Among Women of Reproductive Age GroupDocument4 pagesTitle: Culture and Sensitivity Pattern of Urinary Tract Infection Among Women of Reproductive Age GroupFatima MNo ratings yet
- Recent Sensitivity Pattern of Escherichia Coli in Urinary Tract Infection - Open Access JournalsDocument3 pagesRecent Sensitivity Pattern of Escherichia Coli in Urinary Tract Infection - Open Access JournalsWahyunita Fauzi CahyantiNo ratings yet
- Article PDFDocument8 pagesArticle PDFSipkhotunWindayaniNo ratings yet
- Pathogens 11 01092 v2Document12 pagesPathogens 11 01092 v2nabilla putriNo ratings yet
- Art 5 PDFDocument10 pagesArt 5 PDFpaola lopezNo ratings yet
- An Evaluation of Multidrug Resistant From Aguascalientes, Mexico: Cross Sectional StudyDocument13 pagesAn Evaluation of Multidrug Resistant From Aguascalientes, Mexico: Cross Sectional StudyMidnightNo ratings yet
- Tmp5a61 TMPDocument8 pagesTmp5a61 TMPFrontiersNo ratings yet
- Characteristics and Antibiotic Resistance of Urinary Tract Pathogens Isolated From Punjab, PakistanDocument5 pagesCharacteristics and Antibiotic Resistance of Urinary Tract Pathogens Isolated From Punjab, Pakistanaasi121No ratings yet
- Main Work Co-WriterDocument12 pagesMain Work Co-WriterBoateng JoeNo ratings yet
- A Study of Sensitivity and Resistance of Pathogenic Micro Organisms Causing UTI in Kathmandu ValleyDocument7 pagesA Study of Sensitivity and Resistance of Pathogenic Micro Organisms Causing UTI in Kathmandu ValleypharmaabhishekpandeyNo ratings yet
- Vancomycin Resistance Among Isolates in A Rural Setting, EgyptDocument6 pagesVancomycin Resistance Among Isolates in A Rural Setting, EgyptRidho WahyutomoNo ratings yet
- Job Satisfaction, Organizational Commitment and Job Involvement: The Mediating Role of Job InvolvementDocument12 pagesJob Satisfaction, Organizational Commitment and Job Involvement: The Mediating Role of Job InvolvementmehakNo ratings yet
- A Review of The Challenge-Hindrance Stress Model: Recent Advances, Expanded Paradigms, and Recommendations For Future ResearchDocument12 pagesA Review of The Challenge-Hindrance Stress Model: Recent Advances, Expanded Paradigms, and Recommendations For Future ResearchmehakNo ratings yet
- BoswellOlson BuchananLePine2004JVBStressDocument18 pagesBoswellOlson BuchananLePine2004JVBStressmehakNo ratings yet
- Hobfoll Et Al., 2018 PDFDocument28 pagesHobfoll Et Al., 2018 PDFQundeel HaiderNo ratings yet
- The Relationship Between Challenge and Hindrance Stressors and Emotional Exhaustion: The Moderating Role of Perceived Servant LeadershipDocument15 pagesThe Relationship Between Challenge and Hindrance Stressors and Emotional Exhaustion: The Moderating Role of Perceived Servant LeadershipmehakNo ratings yet
- Corporate Governance Integration With Sustainability: A Systematic Literature ReviewDocument15 pagesCorporate Governance Integration With Sustainability: A Systematic Literature ReviewmehakNo ratings yet
- Impact of Corporate Governance On Corporate Sustainable GrowthDocument18 pagesImpact of Corporate Governance On Corporate Sustainable GrowthmehakNo ratings yet
- Ijbel22 204Document9 pagesIjbel22 204mehakNo ratings yet
- Journal of Cleaner Production: Marco Formentini, Paolo TaticchiDocument14 pagesJournal of Cleaner Production: Marco Formentini, Paolo TaticchiJuan AlmeydaNo ratings yet
- The Corporate Governance of Environmental Sustainability: A Review and Proposal For More Integrated ResearchDocument30 pagesThe Corporate Governance of Environmental Sustainability: A Review and Proposal For More Integrated ResearchmehakNo ratings yet
- A Review Corporate Governance and SustainabilityDocument11 pagesA Review Corporate Governance and SustainabilitymehakNo ratings yet
- Corporate Governance Integration With Sustainability: A Systematic Literature ReviewDocument15 pagesCorporate Governance Integration With Sustainability: A Systematic Literature ReviewmehakNo ratings yet
- Ijbel22 204Document9 pagesIjbel22 204mehakNo ratings yet
- A Review Corporate Governance and SustainabilityDocument11 pagesA Review Corporate Governance and SustainabilitymehakNo ratings yet
- The Corporate Governance of Environmental Sustainability: A Review and Proposal For More Integrated ResearchDocument30 pagesThe Corporate Governance of Environmental Sustainability: A Review and Proposal For More Integrated ResearchmehakNo ratings yet
- A Review Corporate Governance and SustainabilityDocument11 pagesA Review Corporate Governance and SustainabilitymehakNo ratings yet
- Impact of Corporate Governance On Corporate Sustainable GrowthDocument18 pagesImpact of Corporate Governance On Corporate Sustainable GrowthmehakNo ratings yet
- Journal of Cleaner Production: Marco Formentini, Paolo TaticchiDocument14 pagesJournal of Cleaner Production: Marco Formentini, Paolo TaticchiJuan AlmeydaNo ratings yet
- Journal of Cleaner Production: Marco Formentini, Paolo TaticchiDocument14 pagesJournal of Cleaner Production: Marco Formentini, Paolo TaticchiJuan AlmeydaNo ratings yet
- Corporate Governance Integration With Sustainability: A Systematic Literature ReviewDocument15 pagesCorporate Governance Integration With Sustainability: A Systematic Literature ReviewmehakNo ratings yet
- Ijbel22 204Document9 pagesIjbel22 204mehakNo ratings yet
- The Corporate Governance of Environmental Sustainability: A Review and Proposal For More Integrated ResearchDocument30 pagesThe Corporate Governance of Environmental Sustainability: A Review and Proposal For More Integrated ResearchmehakNo ratings yet
- Michel On 2010Document33 pagesMichel On 2010Tawsif HasanNo ratings yet
- Impact of Corporate Governance On Corporate Sustainable GrowthDocument18 pagesImpact of Corporate Governance On Corporate Sustainable GrowthmehakNo ratings yet
- Relationship Between Corporate Governance, Corporate Sustainability and Financial PerformanceDocument21 pagesRelationship Between Corporate Governance, Corporate Sustainability and Financial PerformancemehakNo ratings yet
- Governance and SustainabilityDocument17 pagesGovernance and SustainabilitymehakNo ratings yet
- Current Management of Hepatocellular Carcinoma: Ana Maria Crissien, MD, and Catherine Frenette, MDDocument9 pagesCurrent Management of Hepatocellular Carcinoma: Ana Maria Crissien, MD, and Catherine Frenette, MDmehakNo ratings yet
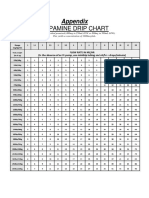
- Dopamine Drip ChartDocument1 pageDopamine Drip ChartmehakNo ratings yet
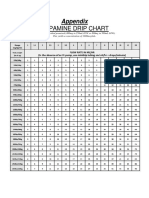
- Dopamine Drip ChartDocument1 pageDopamine Drip ChartmehakNo ratings yet
- Guias Del Uso de Albumina e IgGDocument19 pagesGuias Del Uso de Albumina e IgGRonny Muñoz AcuñaNo ratings yet
- Skenario A Blok 24Document45 pagesSkenario A Blok 24Dita MariscaNo ratings yet
- Kelly 2005 British Journal of Oral and Maxillofacial SurgeryDocument1 pageKelly 2005 British Journal of Oral and Maxillofacial SurgerylalajanNo ratings yet
- Permanent Fixation System: Instructions For UseDocument60 pagesPermanent Fixation System: Instructions For UseAlexandra constantinNo ratings yet
- Health PromotionDocument47 pagesHealth PromotionPauline IntiaNo ratings yet
- NebulizationDocument2 pagesNebulizationArmie Joy Embat CariazoNo ratings yet
- UFO Reporter - Volume 2, Number 1 (March 1993)Document28 pagesUFO Reporter - Volume 2, Number 1 (March 1993)UFO Research (NSW) Incorporated, Australia100% (2)
- Clinico Social CaseDocument6 pagesClinico Social CaseNakshatra ReddyNo ratings yet
- SCE ED Sample QuestionsDocument25 pagesSCE ED Sample QuestionsZoya Annam100% (2)
- Pertemuan 3Document8 pagesPertemuan 3Berkah Tania Sawitri PasaribuNo ratings yet
- The Structure and Function of The Respiratory SystemDocument18 pagesThe Structure and Function of The Respiratory SystemVykin OngNo ratings yet
- Megha Kulkarni: Dept of PharmacologyDocument51 pagesMegha Kulkarni: Dept of PharmacologyMegha Kulkarni FPS PES UniversityNo ratings yet
- Help Pedsurgeryafrica38Document6 pagesHelp Pedsurgeryafrica38madalinamihailescuNo ratings yet
- Complete Drug FormularyDocument96 pagesComplete Drug FormularyRPh Krishna Chandra JagritNo ratings yet
- WHLP in Science 6 Q2 Week 1Document4 pagesWHLP in Science 6 Q2 Week 1ROVELYNE DE LUNANo ratings yet
- Antenatal CareDocument30 pagesAntenatal CareMrs RehanNo ratings yet
- Vivar CG-Putting Conflict ManagementDocument6 pagesVivar CG-Putting Conflict ManagementlemootpNo ratings yet
- Pelvic Inflammatory Disease (Pid)Document42 pagesPelvic Inflammatory Disease (Pid)Aruna PoovalingamNo ratings yet
- Community Development ProjectDocument12 pagesCommunity Development ProjectSwethaNo ratings yet
- International Marketing-PG-III Sem-Marketing 3Document3 pagesInternational Marketing-PG-III Sem-Marketing 3Ankit KumarNo ratings yet
- Netra Kriya KalpamDocument33 pagesNetra Kriya KalpamVineethJoseph67% (3)
- Abc Ved PDFDocument4 pagesAbc Ved PDFRiki DarwisNo ratings yet
- What Is The Best Method To Remove Pearly Papules Easily and Quickly at Home in 2019 PDFDocument3 pagesWhat Is The Best Method To Remove Pearly Papules Easily and Quickly at Home in 2019 PDFElizabeth KingsleyNo ratings yet
- Negative AutopsyDocument21 pagesNegative Autopsydr rizwanNo ratings yet
- The 11 Healing Arts Systems of ThailandDocument15 pagesThe 11 Healing Arts Systems of ThailandShama Kern100% (1)
- NCDPD Script Implementation Recommendations V 127Document102 pagesNCDPD Script Implementation Recommendations V 127john mullerNo ratings yet
- MM 2012 Ghana Presentation PackageDocument25 pagesMM 2012 Ghana Presentation PackageParoubkův PrďákNo ratings yet
- Ericksonian Approaches To Pain ManagementDocument6 pagesEricksonian Approaches To Pain Managementosher2650% (2)
- Cephalometrics For Orthognathic SurgeryDocument11 pagesCephalometrics For Orthognathic SurgeryGowri ShankarNo ratings yet
- Brinda Garikapati Senior Project Acorn Press ReleaseDocument1 pageBrinda Garikapati Senior Project Acorn Press Releaseapi-654010039No ratings yet
- Nursing OB Exam Q & ADocument173 pagesNursing OB Exam Q & Ajoerobinson8889323100% (8)
- Monkeys, Myths, and Molecules: Separating Fact from Fiction, and the Science of Everyday LifeFrom EverandMonkeys, Myths, and Molecules: Separating Fact from Fiction, and the Science of Everyday LifeRating: 4 out of 5 stars4/5 (1)
- Organic Chemistry for Schools: Advanced Level and Senior High SchoolFrom EverandOrganic Chemistry for Schools: Advanced Level and Senior High SchoolNo ratings yet
- Periodic Tales: A Cultural History of the Elements, from Arsenic to ZincFrom EverandPeriodic Tales: A Cultural History of the Elements, from Arsenic to ZincRating: 3.5 out of 5 stars3.5/5 (137)
- Is That a Fact?: Frauds, Quacks, and the Real Science of Everyday LifeFrom EverandIs That a Fact?: Frauds, Quacks, and the Real Science of Everyday LifeRating: 4.5 out of 5 stars4.5/5 (3)
- The Disappearing Spoon: And Other True Tales of Madness, Love, and the History of the World from the Periodic Table of the ElementsFrom EverandThe Disappearing Spoon: And Other True Tales of Madness, Love, and the History of the World from the Periodic Table of the ElementsRating: 4 out of 5 stars4/5 (146)
- The Periodic Table of Elements - Post-Transition Metals, Metalloids and Nonmetals | Children's Chemistry BookFrom EverandThe Periodic Table of Elements - Post-Transition Metals, Metalloids and Nonmetals | Children's Chemistry BookNo ratings yet
- Chemistry: a QuickStudy Laminated Reference GuideFrom EverandChemistry: a QuickStudy Laminated Reference GuideRating: 5 out of 5 stars5/5 (1)
- The Elements We Live By: How Iron Helps Us Breathe, Potassium Lets Us See, and Other Surprising Superpowers of the Periodic TableFrom EverandThe Elements We Live By: How Iron Helps Us Breathe, Potassium Lets Us See, and Other Surprising Superpowers of the Periodic TableRating: 3.5 out of 5 stars3.5/5 (22)
- Meltdown: Nuclear disaster and the human cost of going criticalFrom EverandMeltdown: Nuclear disaster and the human cost of going criticalRating: 5 out of 5 stars5/5 (5)
- Essential Oil Chemistry Formulating Essential Oil Blends that Heal - Aldehyde - Ketone - Lactone: Healing with Essential OilFrom EverandEssential Oil Chemistry Formulating Essential Oil Blends that Heal - Aldehyde - Ketone - Lactone: Healing with Essential OilRating: 5 out of 5 stars5/5 (1)
- Handbook of Formulating Dermal Applications: A Definitive Practical GuideFrom EverandHandbook of Formulating Dermal Applications: A Definitive Practical GuideNo ratings yet
- The Regenerative Grower's Guide to Garden Amendments: Using Locally Sourced Materials to Make Mineral and Biological Extracts and FermentsFrom EverandThe Regenerative Grower's Guide to Garden Amendments: Using Locally Sourced Materials to Make Mineral and Biological Extracts and FermentsRating: 5 out of 5 stars5/5 (3)
- Tribology: Friction and Wear of Engineering MaterialsFrom EverandTribology: Friction and Wear of Engineering MaterialsRating: 5 out of 5 stars5/5 (1)
- Science Goes Viral: Captivating Accounts of Science in Everyday LifeFrom EverandScience Goes Viral: Captivating Accounts of Science in Everyday LifeRating: 5 out of 5 stars5/5 (1)
- A Perfect Red: Empire, Espionage, and the Quest for the Color of DesireFrom EverandA Perfect Red: Empire, Espionage, and the Quest for the Color of DesireRating: 4 out of 5 stars4/5 (129)
- Bioplastics: A Home Inventors HandbookFrom EverandBioplastics: A Home Inventors HandbookRating: 4 out of 5 stars4/5 (2)
- Formulating, Packaging, and Marketing of Natural Cosmetic ProductsFrom EverandFormulating, Packaging, and Marketing of Natural Cosmetic ProductsNo ratings yet
- The Periodic Table: A Very Short IntroductionFrom EverandThe Periodic Table: A Very Short IntroductionRating: 4.5 out of 5 stars4.5/5 (3)
- Phase Equilibria in Chemical EngineeringFrom EverandPhase Equilibria in Chemical EngineeringRating: 4 out of 5 stars4/5 (11)
- The Periodic Table of Elements - Alkali Metals, Alkaline Earth Metals and Transition Metals | Children's Chemistry BookFrom EverandThe Periodic Table of Elements - Alkali Metals, Alkaline Earth Metals and Transition Metals | Children's Chemistry BookNo ratings yet