You might also like
- Current Trends in The Understanding and Treatment of Social Phobia inDocument14 pagesCurrent Trends in The Understanding and Treatment of Social Phobia inDenise Nuñez0% (1)
- Adhd Autism The Two Conditions Can Occur TogetherDocument7 pagesAdhd Autism The Two Conditions Can Occur TogetherHariharanNo ratings yet
- Ultralearning: Scott H. YoungDocument16 pagesUltralearning: Scott H. YoungRui Gonçalves Domingues100% (4)
- Research About Depression and SuicideDocument32 pagesResearch About Depression and SuicideMarcus Kenji100% (2)
- Autism-Mind, Emotion, and The Spectrum of Autism - Dr. Dan SiegelDocument2 pagesAutism-Mind, Emotion, and The Spectrum of Autism - Dr. Dan Siegelcinfer75No ratings yet
- The LGBQ Microaggressions On Campus Scale A Scale Development and Validation Study Woodford2015Document29 pagesThe LGBQ Microaggressions On Campus Scale A Scale Development and Validation Study Woodford2015Salman Tahir100% (1)
- Confusion Between Depression and Autism in A High Functioning ChildDocument14 pagesConfusion Between Depression and Autism in A High Functioning ChildClaudia MihaiNo ratings yet
- Running Head: Reading Facial Expressions 1Document26 pagesRunning Head: Reading Facial Expressions 1Shyan TanuNo ratings yet
- A Cognitive Model of SchizophreniaDocument9 pagesA Cognitive Model of SchizophreniaLopaal83No ratings yet
- Depression and Trauma A Transgenerational Psychoanalytic PerspectiveDocument20 pagesDepression and Trauma A Transgenerational Psychoanalytic PerspectiveAnonymous 18EBcIw2C100% (1)
- 2b English Pe221Document13 pages2b English Pe221Patchy chyNo ratings yet
- Can Collage-Based Art Therapy Be A Bridge To Engage Patients ExpeDocument44 pagesCan Collage-Based Art Therapy Be A Bridge To Engage Patients ExpeRaelna SahaarNo ratings yet
- Final EPQDocument19 pagesFinal EPQtanishasen4No ratings yet
- Aust N Z J Psychiatry 2013 Marnane 12 5Document5 pagesAust N Z J Psychiatry 2013 Marnane 12 5KThreopusNo ratings yet
- Student'S Having Anxiety & DepressionDocument10 pagesStudent'S Having Anxiety & DepressionAmie TabiNo ratings yet
- The Effects Isolation Has On Anxiety and DepressionDocument13 pagesThe Effects Isolation Has On Anxiety and Depressionapi-601562832No ratings yet
- Sample Paper 1Document36 pagesSample Paper 1Annshai Jam MetanteNo ratings yet
- Family Profiles in Eating Disorders Family Functioning and PsychopathologyDocument9 pagesFamily Profiles in Eating Disorders Family Functioning and Psychopathologygiulia.ballarottoNo ratings yet
- Rumination and Loneliness Independently Predict Six-Month Later Depression Symptoms Among Chinese Elderly in Nursing HomesDocument10 pagesRumination and Loneliness Independently Predict Six-Month Later Depression Symptoms Among Chinese Elderly in Nursing HomesgejibNo ratings yet
- Becker 2007Document6 pagesBecker 2007Stroe EmmaNo ratings yet
- Loneliness, Resilience, Mental Health, and Quality of Life in Old Age: A Structural Equation ModelDocument12 pagesLoneliness, Resilience, Mental Health, and Quality of Life in Old Age: A Structural Equation ModelpangaribuansantaNo ratings yet
- Artical 2Document8 pagesArtical 2Noori Zahoor KhanNo ratings yet
- Coun 646 Research Paper FinalDocument18 pagesCoun 646 Research Paper FinalMaLinda DiTonnoNo ratings yet
- Example of A Research Paper On SchizophreniaDocument4 pagesExample of A Research Paper On Schizophreniaafeawjjwp100% (1)
- Research Paper Schizophrenia OutlineDocument5 pagesResearch Paper Schizophrenia Outlineguzxwacnd100% (1)
- Morgades Bamba2019 PDFDocument7 pagesMorgades Bamba2019 PDFArif IrpanNo ratings yet
- Research EssayDocument13 pagesResearch Essayapi-549209684No ratings yet
- Vassetal 2015Document9 pagesVassetal 2015njevkoNo ratings yet
- Soledad y PsicosisDocument12 pagesSoledad y PsicosisMiniNo ratings yet
- Bandelow, Michaelis - 2015 - Epidemiology of Anxiety Disorders in The 21st Century PDFDocument9 pagesBandelow, Michaelis - 2015 - Epidemiology of Anxiety Disorders in The 21st Century PDFjan5437No ratings yet
- Beyond Worry - How Psychologists Help With Anxiety DisordersDocument5 pagesBeyond Worry - How Psychologists Help With Anxiety DisordersPaola BertelloNo ratings yet
- Five Source Annotated BibliographyDocument10 pagesFive Source Annotated Bibliographyapi-382971858No ratings yet
- Artículo Tema 4 Tratamiento para La Depresión en Niños y PreescolaresDocument5 pagesArtículo Tema 4 Tratamiento para La Depresión en Niños y PreescolaresMariaAn DominguezNo ratings yet
- Social Anxiety Research Paper IdeasDocument6 pagesSocial Anxiety Research Paper Ideaswkzcoprhf100% (1)
- Clinical Practice & Epidemiology in Mental HealthDocument10 pagesClinical Practice & Epidemiology in Mental HealthAngeloNo ratings yet
- Vass 2015Document9 pagesVass 2015Amina LabiadhNo ratings yet
- Lon IlnessDocument23 pagesLon Ilnesschris24332178No ratings yet
- Literature Review - Pankhuri Saxena 3Document3 pagesLiterature Review - Pankhuri Saxena 3api-610037275No ratings yet
- How Anxiety Exacerbates Youth Development - Malik AliDocument13 pagesHow Anxiety Exacerbates Youth Development - Malik Aliapi-609501452No ratings yet
- Anxiety: A Concept Analysis: Frontiers ofDocument4 pagesAnxiety: A Concept Analysis: Frontiers ofMathewNo ratings yet
- Journal of Affective Disorders: Social Anxiety and Depression Stigma Among AdolescentsDocument10 pagesJournal of Affective Disorders: Social Anxiety and Depression Stigma Among AdolescentsPutri Indah PermataNo ratings yet
- Mental Health Class Assignment 1 Week 7 Sem 3Document17 pagesMental Health Class Assignment 1 Week 7 Sem 3api-582247328No ratings yet
- The Impact of A PsychoeducationalDocument8 pagesThe Impact of A PsychoeducationalDragos IvanNo ratings yet
- Causes & Relation of Anxiety DXDocument23 pagesCauses & Relation of Anxiety DXMustabeen TairNo ratings yet
- Managing Teen Stress: December 2015Document11 pagesManaging Teen Stress: December 2015Lan TrầnNo ratings yet
- HHS Public Access: Assessment and Treatment of Anxiety Disorders in Children and AdolescentsDocument19 pagesHHS Public Access: Assessment and Treatment of Anxiety Disorders in Children and Adolescentsayub01No ratings yet
- Epidemiology of Anxiety Disorders in The 21st CenturyDocument10 pagesEpidemiology of Anxiety Disorders in The 21st CenturyRebeca EspinosaNo ratings yet
- Tapos Na PaghihirapDocument41 pagesTapos Na Paghihirapharreh hotdoggssNo ratings yet
- Research PaperDocument10 pagesResearch Paperapi-523240479No ratings yet
- Psychiatry Research: Jack Tsai, Robert A. RosenheckDocument5 pagesPsychiatry Research: Jack Tsai, Robert A. RosenheckRaj DesaiNo ratings yet
- Research Paper Over SchizophreniaDocument8 pagesResearch Paper Over Schizophreniafvfee39d100% (3)
- Schizophrenia Research Paper PDFDocument6 pagesSchizophrenia Research Paper PDFef71d9gw100% (1)
- English ResearchDocument20 pagesEnglish ResearchIñaki Zuriel ConstantinoNo ratings yet
- The Etiology of Social Anxiety Disorder - An Evidence-Based ModelDocument3 pagesThe Etiology of Social Anxiety Disorder - An Evidence-Based ModelEvy Sulfiani KomalaNo ratings yet
- Schizophrenia: Etiology, Pathophysiology and Management - A ReviewDocument7 pagesSchizophrenia: Etiology, Pathophysiology and Management - A ReviewFausiah Ulva MNo ratings yet
- Research Paper Schizophrenia Apa StyleDocument4 pagesResearch Paper Schizophrenia Apa Stylevshyrpznd100% (1)
- Introduction MIATIMOTIEDocument6 pagesIntroduction MIATIMOTIEmanaloroberto455No ratings yet
- Childhood Separation Anxiety and The Pathogenesis and Treatment of Adult AnxietyDocument10 pagesChildhood Separation Anxiety and The Pathogenesis and Treatment of Adult AnxietyyesumovsNo ratings yet
- 10 Kuckuk Original 9 1Document12 pages10 Kuckuk Original 9 1KatherineLaTorreCayetanoNo ratings yet
- Cervin2019 PDFDocument10 pagesCervin2019 PDFAhmet Fatih SarıkayaNo ratings yet
- Stigma - Schizophrenia BulletinDocument2 pagesStigma - Schizophrenia BulletinRobsonNo ratings yet
- Neuroanatomia Funcional Machado 3 Ed 2014Document34 pagesNeuroanatomia Funcional Machado 3 Ed 2014ThiagoSoaresNo ratings yet
- Links Between Creativity and Mental DisorderDocument19 pagesLinks Between Creativity and Mental DisorderTuğçe DemirciNo ratings yet
- Handbook of Autism and AnxietyFrom EverandHandbook of Autism and AnxietyThompson E. Davis IIINo ratings yet
- Job Satisfaction, Organizational Commitment and Job Involvement: The Mediating Role of Job InvolvementDocument12 pagesJob Satisfaction, Organizational Commitment and Job Involvement: The Mediating Role of Job InvolvementmehakNo ratings yet
- BoswellOlson BuchananLePine2004JVBStressDocument18 pagesBoswellOlson BuchananLePine2004JVBStressmehakNo ratings yet
- A Review of The Challenge-Hindrance Stress Model: Recent Advances, Expanded Paradigms, and Recommendations For Future ResearchDocument12 pagesA Review of The Challenge-Hindrance Stress Model: Recent Advances, Expanded Paradigms, and Recommendations For Future ResearchmehakNo ratings yet
- A Review Corporate Governance and SustainabilityDocument11 pagesA Review Corporate Governance and SustainabilitymehakNo ratings yet
- Ijbel22 204Document9 pagesIjbel22 204mehakNo ratings yet
- Impact of Corporate Governance On Corporate Sustainable GrowthDocument18 pagesImpact of Corporate Governance On Corporate Sustainable GrowthmehakNo ratings yet
- Corporate Governance Integration With Sustainability: A Systematic Literature ReviewDocument15 pagesCorporate Governance Integration With Sustainability: A Systematic Literature ReviewmehakNo ratings yet
- Governance and SustainabilityDocument17 pagesGovernance and SustainabilitymehakNo ratings yet
- The Corporate Governance of Environmental Sustainability: A Review and Proposal For More Integrated ResearchDocument30 pagesThe Corporate Governance of Environmental Sustainability: A Review and Proposal For More Integrated ResearchmehakNo ratings yet
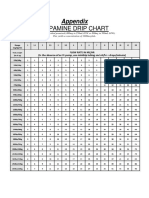
- Dopamine Drip ChartDocument1 pageDopamine Drip ChartmehakNo ratings yet
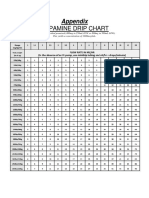
- Dopamine Drip ChartDocument1 pageDopamine Drip ChartmehakNo ratings yet
- Anak - Kasus 7 - Kelompok 7Document48 pagesAnak - Kasus 7 - Kelompok 7mehakNo ratings yet
- Zhou2019 Article InsulinDegludecANovelUltra-LonDocument18 pagesZhou2019 Article InsulinDegludecANovelUltra-LonmehakNo ratings yet
- The Correlation of Structural and Binding Affinity of Insulin Analog To The Onset of Action For Diabetic TherapyDocument9 pagesThe Correlation of Structural and Binding Affinity of Insulin Analog To The Onset of Action For Diabetic TherapymehakNo ratings yet
- This Content Downloaded From 202.43.95.25 On Tue, 05 Oct 2021 01:35:52 UTCDocument8 pagesThis Content Downloaded From 202.43.95.25 On Tue, 05 Oct 2021 01:35:52 UTCmehakNo ratings yet
- Kementerian Pendidikan, Kebudayaan Riset Dan Teknologi: Direktorat Jenderal Pendidikan TinggiDocument11 pagesKementerian Pendidikan, Kebudayaan Riset Dan Teknologi: Direktorat Jenderal Pendidikan TinggimehakNo ratings yet
- Podcast 3 ScriptDocument6 pagesPodcast 3 Scriptapi-553355146No ratings yet
- Nicole Ohl-Shaws RecommendationDocument2 pagesNicole Ohl-Shaws Recommendationapi-545763427No ratings yet
- 2 Final UPDATED SYNOPSIS of PHDDocument22 pages2 Final UPDATED SYNOPSIS of PHDtarun aggarwalNo ratings yet
- Lowen Alexander - The Betrayal of The Body 1967 - Neurosis - IdDocument1 pageLowen Alexander - The Betrayal of The Body 1967 - Neurosis - IdSthevan dos SantosNo ratings yet
- Political Affect - Connecting The Social and The Somatic Conclunsion ChapDocument9 pagesPolitical Affect - Connecting The Social and The Somatic Conclunsion ChapSun PraboonyaNo ratings yet
- Horizon Report Europe 2014 Schools Edition: EUR 26673 ENDocument60 pagesHorizon Report Europe 2014 Schools Edition: EUR 26673 ENAdelina SilvaNo ratings yet
- Assessment Type: Formative Assessments: Embedded Questions in VideoDocument2 pagesAssessment Type: Formative Assessments: Embedded Questions in Video18 Mansi MengdeNo ratings yet
- Huma 2nd Quarter ReviewerDocument5 pagesHuma 2nd Quarter ReviewerBea Elisha JanabanNo ratings yet
- Confessional Poetry of Eunice de Souza and Sylvia Plath A Study in ComparisonDocument9 pagesConfessional Poetry of Eunice de Souza and Sylvia Plath A Study in ComparisonRahul Ranjan100% (1)
- Sining Silabus AgricultureDocument11 pagesSining Silabus AgricultureJudemarife RicoroyoNo ratings yet
- Publications Related To The DASS Itself: - Ed.) Sydney: Psychology Foundation. ISBN 7334-1423-0Document2 pagesPublications Related To The DASS Itself: - Ed.) Sydney: Psychology Foundation. ISBN 7334-1423-0Bora TagoraNo ratings yet
- PoliticsDocument27 pagesPoliticsParantak YadavNo ratings yet
- Classroom Management PhilosophyDocument7 pagesClassroom Management Philosophyapi-533496819No ratings yet
- Beck 2011Document16 pagesBeck 2011MariaNo ratings yet
- 7 Ways To Lead Your Team (Notes)Document3 pages7 Ways To Lead Your Team (Notes)BrianNo ratings yet
- Analisis Negosiasi Bisnis Pada PT Allegrindo NusantaraDocument5 pagesAnalisis Negosiasi Bisnis Pada PT Allegrindo Nusantaramuhammad akmalulmazaya ChoiriNo ratings yet
- Introduction To World Religions and Belief SystemsDocument4 pagesIntroduction To World Religions and Belief SystemsDanilo Siquig Jr.No ratings yet
- Use of A Writing Web-Site by Pre-Masters Students On An English For Academic Purposes Course. A. J. Gillett, University of HertfordshireDocument1 pageUse of A Writing Web-Site by Pre-Masters Students On An English For Academic Purposes Course. A. J. Gillett, University of HertfordshirerezkyNo ratings yet
- Aj Thesis-ReviewerDocument4 pagesAj Thesis-ReviewerRichmon SantosNo ratings yet
- Syllabus - CourseraDocument4 pagesSyllabus - CourseraRahulChampNo ratings yet
- Ms Grimes Letter of RecDocument1 pageMs Grimes Letter of Recapi-545428249No ratings yet
- Cwts 10023 - Civic Welfare Training ServiceDocument3 pagesCwts 10023 - Civic Welfare Training ServiceAly CapistranoNo ratings yet
- Lesson 2 AbstractionDocument5 pagesLesson 2 AbstractionLovely Grace CajegasNo ratings yet
- AAF Hong KongDocument10 pagesAAF Hong KongCarlo L. TongolNo ratings yet
- Erikson's 8 Stages of Psychosocial Development: Attitudes MasteryDocument29 pagesErikson's 8 Stages of Psychosocial Development: Attitudes MasterySushma SwathiNo ratings yet