You might also like
- HPLC Method Development ProtocolDocument40 pagesHPLC Method Development ProtocolDavid Torres100% (1)
- Calcium Metabolism & Calcium Metabolism DisordersDocument45 pagesCalcium Metabolism & Calcium Metabolism Disorderstrisya arthaputriNo ratings yet
- Environmental Systems and SocietiesDocument18 pagesEnvironmental Systems and Societiesanthor100% (1)
- Renal Diet Cookbook for Beginners: Enjoy Delicious, Kidney-Friendly Recipes with Balanced Sodium, Phosphorus, and Potassium Levels [III EDITION]From EverandRenal Diet Cookbook for Beginners: Enjoy Delicious, Kidney-Friendly Recipes with Balanced Sodium, Phosphorus, and Potassium Levels [III EDITION]Rating: 5 out of 5 stars5/5 (18)
- Nursing Lab 3 Skill Performance Checklist Administering A Blood Transfusion S U NP CommentsDocument2 pagesNursing Lab 3 Skill Performance Checklist Administering A Blood Transfusion S U NP CommentsCandice Cheng88% (8)
- Fluid, Electrolyte, and Acid-Base BalanceDocument41 pagesFluid, Electrolyte, and Acid-Base BalanceRn nadeenNo ratings yet
- Parathyroid: Calcium and Vitamin DDocument135 pagesParathyroid: Calcium and Vitamin DPhysiology by Dr RaghuveerNo ratings yet
- Fluid Electrolyte ImbalanceDocument15 pagesFluid Electrolyte ImbalancePrasanth Kurien Mathew100% (9)
- Pizzorno AcidosisDocument106 pagesPizzorno AcidosisAmber ChenNo ratings yet
- (P) Physiology - CimDocument7 pages(P) Physiology - CimfilchibuffNo ratings yet
- Calcium and Phosphate MetabolismDocument70 pagesCalcium and Phosphate MetabolismHariprasad L0% (1)
- Alkaline Water StudyDocument5 pagesAlkaline Water StudyKENS 5No ratings yet
- SLEDAIDocument2 pagesSLEDAIKomang Adhi AmertajayaNo ratings yet
- MineralsDocument9 pagesMineralsDerek AtienzaNo ratings yet
- Calcium Metabolism: DR - Ammar Jawad MBCHB, MPHDocument54 pagesCalcium Metabolism: DR - Ammar Jawad MBCHB, MPHMurali ManiNo ratings yet
- Calcium Phosphorus Metabolic DisordersDocument102 pagesCalcium Phosphorus Metabolic DisordersAME DENTAL COLLEGE RAICHUR, KARNATAKANo ratings yet
- Dietry MineralsDocument269 pagesDietry MineralsNashrah Nashrah (22043)No ratings yet
- Calcium Metabolism / Orthodontic Courses by Indian Dental AcademyDocument23 pagesCalcium Metabolism / Orthodontic Courses by Indian Dental Academyindian dental academy100% (2)
- Potter & Perry: Fundamentals of Nursing, 7 EditionDocument11 pagesPotter & Perry: Fundamentals of Nursing, 7 Editionmissy23pap100% (1)
- Calcium & Phosphorus MetabolismDocument90 pagesCalcium & Phosphorus MetabolismSriya Saatwika ReddyNo ratings yet
- Department of Periodontics and Implantology: Calcium MetabolismDocument63 pagesDepartment of Periodontics and Implantology: Calcium Metabolismrasagna reddy100% (1)
- Fluid and Electrolyte BalanceDocument23 pagesFluid and Electrolyte BalanceRamadan PhysiologyNo ratings yet
- Fluids and ElectrolytesDocument19 pagesFluids and Electrolytesderic100% (5)
- Potassium Regulation in The NeonateDocument13 pagesPotassium Regulation in The NeonateLuis Ruelas SanchezNo ratings yet
- Calcium MetabolismDocument86 pagesCalcium MetabolismSushmitKojuNo ratings yet
- Calcium Metabolism: Dr. Yuliana Rahmah R, M.Kes, SPPDDocument28 pagesCalcium Metabolism: Dr. Yuliana Rahmah R, M.Kes, SPPDAhmad Jaelani Jayadi SiajengNo ratings yet
- Disorders of Calcium, Inorganic Phosphate and Magnesium Metabolism 1Document62 pagesDisorders of Calcium, Inorganic Phosphate and Magnesium Metabolism 1IiiNo ratings yet
- Function of The Renal and Urinary Tract System: Medical-Surgical Nursing, 4/eDocument117 pagesFunction of The Renal and Urinary Tract System: Medical-Surgical Nursing, 4/eBryJos tiongsonNo ratings yet
- Calcium Metabolism PraveenDocument42 pagesCalcium Metabolism PraveenDr PraveenNo ratings yet
- 5 Minute Biochemistry PresentationDocument23 pages5 Minute Biochemistry PresentationPITAGAN, Galda Boy 1-FNo ratings yet
- Nutrional Aspects of Calcium AbsorptionDocument4 pagesNutrional Aspects of Calcium Absorptiondian aristiaNo ratings yet
- NIH Public Access: Inherited Disorders of Calcium and Phosphate MetabolismDocument15 pagesNIH Public Access: Inherited Disorders of Calcium and Phosphate MetabolismWasim ShaheenNo ratings yet
- Minerals: From Essentials of Medical Biochemistry by R.C. GuptaDocument245 pagesMinerals: From Essentials of Medical Biochemistry by R.C. GuptaMalliga SundareshanNo ratings yet
- Parathyroid, Calcium, and Bone DR - EricDocument116 pagesParathyroid, Calcium, and Bone DR - EricRezka ZmNo ratings yet
- Body FluidsDocument2 pagesBody FluidsMaria Jenina CervantesNo ratings yet
- Fluid and Electrolyte Imbalances Part 1Document34 pagesFluid and Electrolyte Imbalances Part 1Gabrielle Frances FernandezNo ratings yet
- Kington Life Plasma IsotonicDocument69 pagesKington Life Plasma Isotonicahmad.albab.alfatihNo ratings yet
- Calcium MetabolismDocument51 pagesCalcium MetabolismAlan ThomasNo ratings yet
- Potassium and AnaesthesiaDocument16 pagesPotassium and AnaesthesiaAnonymous S0MyRHNo ratings yet
- Physiology and Pathophysiology of Potassium Homeostasis: Staying CurrentDocument11 pagesPhysiology and Pathophysiology of Potassium Homeostasis: Staying CurrentAngie CornejoNo ratings yet
- Calcium Metabolism: Moderators Prof Deepak Rai DR Mahesha K Presenter: DR Nabeel ShamsDocument67 pagesCalcium Metabolism: Moderators Prof Deepak Rai DR Mahesha K Presenter: DR Nabeel ShamsNabeel ShamsNo ratings yet
- Potasio 2015Document13 pagesPotasio 2015Santiago Basto CruzNo ratings yet
- Emma Wynn, Marc-Antoine Krieg, Jean-Marc Aeschlimann, Peter BurckhardtDocument5 pagesEmma Wynn, Marc-Antoine Krieg, Jean-Marc Aeschlimann, Peter BurckhardtMihai MishuNo ratings yet
- NotesDocument5 pagesNotesjcornell1230No ratings yet
- Calcium PPT BSDocument58 pagesCalcium PPT BSMedical NotesNo ratings yet
- Renal PDFDocument16 pagesRenal PDFsestramitaNo ratings yet
- HypocalemkaDocument13 pagesHypocalemkaLuis Ruelas SanchezNo ratings yet
- Ann. Din. Biochem.: Regulation of Calcium MetabolismDocument22 pagesAnn. Din. Biochem.: Regulation of Calcium MetabolismAzmi FarhadiNo ratings yet
- Ca N P MetaDocument71 pagesCa N P MetaJagadish S GowdaNo ratings yet
- Fluid and Electrolyte in InfantDocument44 pagesFluid and Electrolyte in InfantVibin K vNo ratings yet
- Fluid Therapy in Various ConditionsDocument62 pagesFluid Therapy in Various ConditionsAndy F MonroeNo ratings yet
- Calcium Metabolism: Presented By-Dr. Chinansha Arya Second Year Postgraduate Department of Conservative and EndodonticsDocument103 pagesCalcium Metabolism: Presented By-Dr. Chinansha Arya Second Year Postgraduate Department of Conservative and EndodonticsmeghaNo ratings yet
- Monalisha Ca MetabolismDocument86 pagesMonalisha Ca MetabolismNingombam Robinson SinghNo ratings yet
- Calcium BookDocument28 pagesCalcium BookLucius33No ratings yet
- Mineral: I F Z A L, S.GZ.,RDDocument40 pagesMineral: I F Z A L, S.GZ.,RDAyi Da-VinciNo ratings yet
- Calcium & Phosphorus DentalDocument48 pagesCalcium & Phosphorus Dentalfathimatezil123No ratings yet
- Endocrine Physiology: Dale Buchanan Hales, PHD Department of Physiology & BiophysicsDocument74 pagesEndocrine Physiology: Dale Buchanan Hales, PHD Department of Physiology & BiophysicsOngen AchillesNo ratings yet
- Gupta 2018Document21 pagesGupta 2018Safa NaturasifahNo ratings yet
- Calcium Balance I 2020Document35 pagesCalcium Balance I 2020Nadun MethwadaneNo ratings yet
- LECT 8 Fluids and Electrolyte Balance 2221Document32 pagesLECT 8 Fluids and Electrolyte Balance 2221SaraNo ratings yet
- Calcium Metabolism and Disorders (Hanan)Document169 pagesCalcium Metabolism and Disorders (Hanan)drhananfathyNo ratings yet
- Body Fluid CompartmentsDocument37 pagesBody Fluid Compartmentsmanu sethiNo ratings yet
- CalciuDocument80 pagesCalciuAleks_88No ratings yet
- Calcium Homeostasis and Effects of Hormones On BloodDocument77 pagesCalcium Homeostasis and Effects of Hormones On Bloodkomal nanavatiNo ratings yet
- Antimicrobial Renal Dosing Guidelines PDFDocument25 pagesAntimicrobial Renal Dosing Guidelines PDFjennyNo ratings yet
- n-3 Polyunsaturated Fatty Acids RecommendationsDocument2 pagesn-3 Polyunsaturated Fatty Acids RecommendationsEka RendyNo ratings yet
- AnamnesaDocument29 pagesAnamnesaEka RendyNo ratings yet
- Table of ContentDocument1 pageTable of ContentEka RendyNo ratings yet
- n-3 Polyunsaturated Fatty Acids RecommendationsDocument2 pagesn-3 Polyunsaturated Fatty Acids RecommendationsEka RendyNo ratings yet
- Daftar Kehadiran PPDS IKA Per Juli 2021Document2 pagesDaftar Kehadiran PPDS IKA Per Juli 2021Eka RendyNo ratings yet
- Rundown 10 Juli 2021Document1 pageRundown 10 Juli 2021Eka RendyNo ratings yet
- Rundown: Seminar Online UKK Nefrologi IDAI Sabtu, 10 Juli 2021Document1 pageRundown: Seminar Online UKK Nefrologi IDAI Sabtu, 10 Juli 2021Eka RendyNo ratings yet
- Metabolic Response To The Stress of Critical IllnessDocument10 pagesMetabolic Response To The Stress of Critical IllnessValentina bustamanteNo ratings yet
- Jaundice and Acute Liver Failure As The First Manifestation of Acute Myeloid LeukemiaDocument4 pagesJaundice and Acute Liver Failure As The First Manifestation of Acute Myeloid LeukemiaEka RendyNo ratings yet
- Fosfomycin (Oral) Monograph - Paediatric: Children'S Antimicrobial Management Program (Champ)Document4 pagesFosfomycin (Oral) Monograph - Paediatric: Children'S Antimicrobial Management Program (Champ)Eka RendyNo ratings yet
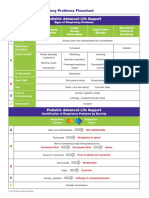
- Recog Resp Problems ChartDocument1 pageRecog Resp Problems ChartEka RendyNo ratings yet
- Pengaruh Penggantian Bovine Serum Albumin BSA DengDocument10 pagesPengaruh Penggantian Bovine Serum Albumin BSA DengRifqy YazidNo ratings yet
- Weather and Climate Extremes: Temperature Extremes: Effect On Plant Growth and DevelopmentDocument14 pagesWeather and Climate Extremes: Temperature Extremes: Effect On Plant Growth and DevelopmentFhenny Rama ShenthauryNo ratings yet
- Case Pres Imperforated HymenDocument133 pagesCase Pres Imperforated Hymenpongiyalabs50% (2)
- Encantia BrochureDocument4 pagesEncantia BrochureVu LeNo ratings yet
- Regulation of Glycogen MetabolismDocument36 pagesRegulation of Glycogen MetabolismNaji Mohamed AlfatihNo ratings yet
- Serodos Plus: Target Values / Sollwerte / Valores Meta/ Valeurs SouhaitéesDocument3 pagesSerodos Plus: Target Values / Sollwerte / Valores Meta/ Valeurs SouhaitéesAniket dubeyNo ratings yet
- Principles of Synthetic BiologyDocument21 pagesPrinciples of Synthetic BiologyOpale PapaleNo ratings yet
- Genetics - CMIDocument177 pagesGenetics - CMI7ett_100% (1)
- Microbial Degradation and Valorization of Plastic WastesDocument20 pagesMicrobial Degradation and Valorization of Plastic WastesSpingus CharlestonNo ratings yet
- Poster ApmlDocument1 pagePoster Apmlkuel1511No ratings yet
- Biology Form 4 AnswersDocument55 pagesBiology Form 4 Answersmasyi meNo ratings yet
- 07 Staining Part 2 and MountingDocument12 pages07 Staining Part 2 and MountingMae BillynNo ratings yet
- Contraceptive Physiology: by Dr.M.Anthony David MD Professor of PhysiologyDocument44 pagesContraceptive Physiology: by Dr.M.Anthony David MD Professor of PhysiologyFlavius AnghelNo ratings yet
- Ecg Made EasyDocument45 pagesEcg Made EasyfisiopopNo ratings yet
- Muscle FibersDocument23 pagesMuscle FibersPhyo TheinkhaNo ratings yet
- Anatomy: Petr Hájek, MD, Phd. Head of Anatomy Dept. Assoc. Prof. Dáša Slížová, MD, Phd. Senior LecturerDocument27 pagesAnatomy: Petr Hájek, MD, Phd. Head of Anatomy Dept. Assoc. Prof. Dáša Slížová, MD, Phd. Senior LecturerTodesengelNo ratings yet
- Biological AnthropologyDocument3 pagesBiological AnthropologyGene'sNo ratings yet
- CancerDocument20 pagesCancerJulio BenitesNo ratings yet
- Compare and Contrast Animal Cell & Plant Cell and Prokaryotic & Eukaryotic Cell Using Venn Diagram.Document1 pageCompare and Contrast Animal Cell & Plant Cell and Prokaryotic & Eukaryotic Cell Using Venn Diagram.Blair Skyreiz NymphNo ratings yet
- Clone 123C3: Monoclonal Mouse Anti-Human CD56 Code M7304Document3 pagesClone 123C3: Monoclonal Mouse Anti-Human CD56 Code M7304Jaimier CajandabNo ratings yet
- Evidence of Evolution PacketDocument8 pagesEvidence of Evolution PacketBeckett DeMossNo ratings yet
- Sage Genetics Lecture 2017 ExpoDocument55 pagesSage Genetics Lecture 2017 ExpoJosé Nigadera de la SotaNo ratings yet
- Plant Diversity and Ethnobotany in Berehet District, North Shewa Zone of Amhara Region (Ethiopia) With Emphasis On Wild Edible PlantsDocument13 pagesPlant Diversity and Ethnobotany in Berehet District, North Shewa Zone of Amhara Region (Ethiopia) With Emphasis On Wild Edible Plantstrradhikashirke5583No ratings yet
- Hardback Test Split Ch4-Refs Index-July18 PDFDocument301 pagesHardback Test Split Ch4-Refs Index-July18 PDFChenier Vega MejiaNo ratings yet
- Nurul Berliana Aini - 081911433043 - D1 - Laporan Praktikum Sampling BentosDocument17 pagesNurul Berliana Aini - 081911433043 - D1 - Laporan Praktikum Sampling Bentosprisca wibawaNo ratings yet
- Grade 4 Science QuestionsDocument7 pagesGrade 4 Science QuestionsJoey CodillaNo ratings yet



![Renal Diet Cookbook for Beginners: Enjoy Delicious, Kidney-Friendly Recipes with Balanced Sodium, Phosphorus, and Potassium Levels [III EDITION]](https://imgv2-2-f.scribdassets.com/img/word_document/623037346/149x198/5582c31ab3/1711569018?v=1)