You might also like
- Uworld NotesDocument2 pagesUworld NotessarahNo ratings yet
- Evaluation and Management of Common Cardiac ConditionsDocument104 pagesEvaluation and Management of Common Cardiac ConditionsRatnam hospital100% (1)
- Neuro Notes Misc.Document11 pagesNeuro Notes Misc.slmrebeiroNo ratings yet
- International Medical Graduate and the United States Medical Residency Application: A Guide to Achieving SuccessFrom EverandInternational Medical Graduate and the United States Medical Residency Application: A Guide to Achieving SuccessRaghav GovindarajanNo ratings yet
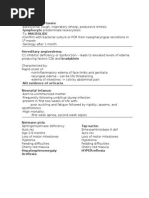
- Placental Site Trophoblastic Tumor:: Proliferation of Intermediate Trophoblasts ProduceDocument2 pagesPlacental Site Trophoblastic Tumor:: Proliferation of Intermediate Trophoblasts ProduceSteph Anie25% (4)
- SURVIVOR’S GUIDE Quick Reviews and Test Taking Skills for USMLE STEP 3From EverandSURVIVOR’S GUIDE Quick Reviews and Test Taking Skills for USMLE STEP 3Rating: 5 out of 5 stars5/5 (1)
- High Yield Uworld ReviewDocument43 pagesHigh Yield Uworld ReviewNazeer ShaikhNo ratings yet
- Uworld NotesDocument32 pagesUworld NotesRednose55100% (1)
- Meckel Diverticulum, H. Influenzae, Biotin, and more medical exam questionsDocument6 pagesMeckel Diverticulum, H. Influenzae, Biotin, and more medical exam questionsPatrik Osornio-CenterwallNo ratings yet
- Uworld NotesDocument17 pagesUworld NotesSinan Khudhur100% (1)
- UW Peds Notes - @pedunculatedDocument179 pagesUW Peds Notes - @pedunculatedMarion Sanchez100% (6)
- UWORLD Second Pass NotesDocument6 pagesUWORLD Second Pass NotesRaquelNo ratings yet
- UWorld Notes Neurology: Spontaneous cerebellar hemorrhageDocument6 pagesUWorld Notes Neurology: Spontaneous cerebellar hemorrhagesarahNo ratings yet
- UWORLD MedicineDocument126 pagesUWORLD Medicineaeltee100% (1)
- Citrate Activates Accoa Carboxylase (Fa Synthesis) and F-1,6 BP (Gluconeogenesis)Document6 pagesCitrate Activates Accoa Carboxylase (Fa Synthesis) and F-1,6 BP (Gluconeogenesis)Nahome YebassewNo ratings yet
- Uworld NotesDocument33 pagesUworld NotesRednose55No ratings yet
- USMLE Step 2 CK: CMS: Psychiatry Form 3Document17 pagesUSMLE Step 2 CK: CMS: Psychiatry Form 3usmleaddict pro57% (7)
- Uworld - PEDIATRICSDocument50 pagesUworld - PEDIATRICSNikxy100% (1)
- Uworld NotesDocument12 pagesUworld NotesTush Rame100% (1)
- DSM5 criteria and treatment for mental disorders and substance useDocument5 pagesDSM5 criteria and treatment for mental disorders and substance useJamesHowson100% (1)
- HY PsychDocument19 pagesHY PsychJamesIwuNo ratings yet
- HighYieldPsychiatry PDFDocument43 pagesHighYieldPsychiatry PDFYay100% (4)
- Psychiatry, Usmle Endpoint by DR Ahmed SheblDocument63 pagesPsychiatry, Usmle Endpoint by DR Ahmed SheblDaNy Chiriac100% (1)
- UW Ped Clerkship Final Exam From CLIPP CasesDocument4 pagesUW Ped Clerkship Final Exam From CLIPP CasesJoe ConeNo ratings yet
- Uworld NotesDocument17 pagesUworld NotesNamRita PrasadNo ratings yet
- CsDocument11 pagesCsmango91286No ratings yet
- Uworld NotesDocument18 pagesUworld NotesNamRita PrasadNo ratings yet
- Musculoskeletal and neurological anatomyDocument220 pagesMusculoskeletal and neurological anatomyRaymond Bernatowicz100% (2)
- Mehlmanmedical Hy PsychDocument19 pagesMehlmanmedical Hy PsychJennifer Ross-ComptisNo ratings yet
- Step 1 6 Week CalendarDocument3 pagesStep 1 6 Week CalendarKawther Abdallah0% (1)
- Divine HYDocument144 pagesDivine HYcasper doggieNo ratings yet
- Step 2 - Notes On Questions From USMLE WorldDocument16 pagesStep 2 - Notes On Questions From USMLE Worldbhav17z100% (1)
- USMLE World: Revision QuestionsDocument65 pagesUSMLE World: Revision QuestionsDustin91% (22)
- Uworld NotesDocument67 pagesUworld NotesNazeer Shaikh100% (4)
- Psychiatric DISORDERSDocument9 pagesPsychiatric DISORDERSNilay Bhatt100% (1)
- Psychiatry - Shelf ReviewDocument101 pagesPsychiatry - Shelf Reviewluck2liv100% (4)
- UWorld 2 CK Notes PDFDocument144 pagesUWorld 2 CK Notes PDFshawnvermaNo ratings yet
- Internal Medicine Notes on Cardiology, Endocrinology, Hematology & OncologyDocument16 pagesInternal Medicine Notes on Cardiology, Endocrinology, Hematology & OncologyLindaLou60% (10)
- Step2ck Practice TestDocument67 pagesStep2ck Practice TestAlf CarlNo ratings yet
- Cardiovascular, ENT, Gynecology Anatomy FlashcardsDocument80 pagesCardiovascular, ENT, Gynecology Anatomy Flashcardsnashra bukhariNo ratings yet
- Uworld Step 2 Question List PDFDocument17 pagesUworld Step 2 Question List PDFMitchell P. Creed100% (2)
- Robert Laverty's Peds UWorld NotesDocument20 pagesRobert Laverty's Peds UWorld NotesAriana SheridanNo ratings yet
- Uworld - ObstetricsDocument40 pagesUworld - ObstetricsNikxyNo ratings yet
- Notes on Medicine SubdivisionsDocument35 pagesNotes on Medicine SubdivisionsTush Rame100% (1)
- 2009 Pearl SheetDocument19 pages2009 Pearl Sheetmikez100% (1)
- U World Notes IIDocument54 pagesU World Notes IIFeroz RaZa SoomrOoNo ratings yet
- High Yield Notes From UW Q BlocksDocument159 pagesHigh Yield Notes From UW Q BlocksKunal Sharma100% (5)
- Pediatrics - Allergy & Immunology TopicsDocument40 pagesPediatrics - Allergy & Immunology TopicspreethamNo ratings yet
- AV UWorld EOs (Rough Draft) - Data - System PortraitDocument63 pagesAV UWorld EOs (Rough Draft) - Data - System PortraitFeroz RaZa SoomrOoNo ratings yet
- TiKi TaKa CK NEUROLOGYDocument24 pagesTiKi TaKa CK NEUROLOGYprofahmedNo ratings yet
- UWorld Notes Step 2 CKDocument11 pagesUWorld Notes Step 2 CKSamah Khan50% (2)
- CMS Psychiatry 1 FormDocument41 pagesCMS Psychiatry 1 FormDuriye Damla Sevgi100% (6)
- Surgery UworldDocument2 pagesSurgery UworldRednose55No ratings yet
- My NotesDocument24 pagesMy NotesrsimranjitNo ratings yet
- Uworld Notes Step 2CKDocument15 pagesUworld Notes Step 2CKMaría Camila Pareja Zabala100% (1)
- HY NBME Psych Review: Some MS4Document114 pagesHY NBME Psych Review: Some MS4Swisskelly1100% (2)
- CardiologySlides 23C 2020 4 Banvir 2aDocument479 pagesCardiologySlides 23C 2020 4 Banvir 2aBanvir SinghNo ratings yet
- Trouble Sleeping, No Anemia, No Pallor, No Night Sweats, No FeverDocument2 pagesTrouble Sleeping, No Anemia, No Pallor, No Night Sweats, No FeverNikxyNo ratings yet
- Guide to Clinical Rotations CourseDocument77 pagesGuide to Clinical Rotations CourseNikxyNo ratings yet
- CardiologySlides 23C 2020 4 Banvir 2aDocument479 pagesCardiologySlides 23C 2020 4 Banvir 2aBanvir SinghNo ratings yet
- High Yield Surgery Shelf ReviewDocument77 pagesHigh Yield Surgery Shelf ReviewDuke71% (7)
- The Kidney!) : Penicillin V Penicillin GDocument10 pagesThe Kidney!) : Penicillin V Penicillin GUsm LeeNo ratings yet
- Uworld - ObstetricsDocument40 pagesUworld - ObstetricsNikxyNo ratings yet
- Uworld - PEDIATRICSDocument50 pagesUworld - PEDIATRICSNikxy100% (1)
- Gynecology Notes Legal Issues and EthicsDocument19 pagesGynecology Notes Legal Issues and EthicsUsm LeeNo ratings yet
- Uworld - INTERNAL MEDICINEDocument131 pagesUworld - INTERNAL MEDICINENikxyNo ratings yet
- SURGICAL PROCEDURES AND COMPLICATIONSDocument55 pagesSURGICAL PROCEDURES AND COMPLICATIONSNikxyNo ratings yet
- Script StsDocument8 pagesScript StsChain HabanaNo ratings yet
- IVF Drug StudyDocument5 pagesIVF Drug StudyHannah Angelu CabadingNo ratings yet
- Sem Type Contoh Thesis !Document23 pagesSem Type Contoh Thesis !Anis Syafika86% (7)
- Utah KidneyDocument16 pagesUtah KidneyChristineGonzalesNo ratings yet
- Laban - Sub Kamal Salman Mahmoud Jaber Mustafa: Done byDocument40 pagesLaban - Sub Kamal Salman Mahmoud Jaber Mustafa: Done byKool Kaish100% (1)
- Laboratory Evaluation of PlateletsDocument28 pagesLaboratory Evaluation of PlateletsTom Anthony TonguiaNo ratings yet
- What Need Know About Wild OreganoDocument21 pagesWhat Need Know About Wild OreganoMatt PintoNo ratings yet
- Renal Disease PresentationDocument17 pagesRenal Disease Presentationapi-292524690No ratings yet
- Effectiveness of thoracic-abdominal rebalancing technique for acute viral bronchiolitisDocument9 pagesEffectiveness of thoracic-abdominal rebalancing technique for acute viral bronchiolitisrebeca paulinoNo ratings yet
- VitaminsDocument409 pagesVitaminsapi-3798616No ratings yet
- Evaluation and Management of Autonomic Nervous System DisordersDocument10 pagesEvaluation and Management of Autonomic Nervous System DisordersbpppbbNo ratings yet
- Clinical Surgery - A Practical GuideDocument449 pagesClinical Surgery - A Practical GuideNewvov100% (9)
- (SAN PEDRO - FGL GRP 2) Anatomy SGD CaseDocument4 pages(SAN PEDRO - FGL GRP 2) Anatomy SGD CaseKRIZIA CORRINE CAINGCOY SAN PEDRONo ratings yet
- Disease and Disease TransmissionDocument48 pagesDisease and Disease TransmissionAYO NELSONNo ratings yet
- Hindu Mantras for Disease Control and Spiritual HealingDocument33 pagesHindu Mantras for Disease Control and Spiritual Healingsunildubey02100% (7)
- EVOLUTION International Catalogue 2016 Charolais enDocument44 pagesEVOLUTION International Catalogue 2016 Charolais enCHe Mie Che AzizNo ratings yet
- IPM for Okra PestsDocument21 pagesIPM for Okra PestsParry Grewal100% (1)
- 4007 6537 1 PBDocument13 pages4007 6537 1 PBDian Gita RamadaniNo ratings yet
- Robert Murphy DissertationDocument6 pagesRobert Murphy DissertationPaperWritingCompanyCanada100% (1)
- 1307 Ascot Bpla (Sever)Document8 pages1307 Ascot Bpla (Sever)Fernando CamargoNo ratings yet
- Pi Is 0002937808008806Document7 pagesPi Is 0002937808008806venkayammaNo ratings yet
- Infant Formulas. Pediatr Rev 2011Document13 pagesInfant Formulas. Pediatr Rev 2011Zeniff ArciveNo ratings yet
- PSORIASISDocument9 pagesPSORIASISDianne BernardoNo ratings yet
- Tuesday, December 09, 2014 EditionDocument16 pagesTuesday, December 09, 2014 EditionFrontPageAfricaNo ratings yet
- Infection Prevention and Control (IPC) For COVID-19 VirusDocument21 pagesInfection Prevention and Control (IPC) For COVID-19 Virusalta graceNo ratings yet
- Cold vs. Flu vs. Allergies vs. COVID-19Document1 pageCold vs. Flu vs. Allergies vs. COVID-19prabuNo ratings yet
- Survivorfinal28 01 2020 PDFDocument25 pagesSurvivorfinal28 01 2020 PDFYogitaNo ratings yet
- Freelesson1endhairloss EulastversionDocument7 pagesFreelesson1endhairloss EulastversionDezant MiradzNo ratings yet
- Cardiac PacingDocument9 pagesCardiac PacingmatzoneNo ratings yet
- Compact Dry: An Easy Test Method For Counting MicroorganismsDocument12 pagesCompact Dry: An Easy Test Method For Counting MicroorganismsSyeda Nazish BokhariNo ratings yet
- The Happiness Trap: How to Stop Struggling and Start LivingFrom EverandThe Happiness Trap: How to Stop Struggling and Start LivingRating: 4 out of 5 stars4/5 (1)
- An Autobiography of Trauma: A Healing JourneyFrom EverandAn Autobiography of Trauma: A Healing JourneyRating: 5 out of 5 stars5/5 (2)
- Rewire Your Anxious Brain: How to Use the Neuroscience of Fear to End Anxiety, Panic, and WorryFrom EverandRewire Your Anxious Brain: How to Use the Neuroscience of Fear to End Anxiety, Panic, and WorryRating: 4.5 out of 5 stars4.5/5 (157)
- Rapid Weight Loss Hypnosis: How to Lose Weight with Self-Hypnosis, Positive Affirmations, Guided Meditations, and Hypnotherapy to Stop Emotional Eating, Food Addiction, Binge Eating and MoreFrom EverandRapid Weight Loss Hypnosis: How to Lose Weight with Self-Hypnosis, Positive Affirmations, Guided Meditations, and Hypnotherapy to Stop Emotional Eating, Food Addiction, Binge Eating and MoreRating: 5 out of 5 stars5/5 (17)
- Summary of The Body Keeps the Score: Brain, Mind, and Body in the Healing of Trauma by Bessel van der Kolk MDFrom EverandSummary of The Body Keeps the Score: Brain, Mind, and Body in the Healing of Trauma by Bessel van der Kolk MDRating: 4.5 out of 5 stars4.5/5 (167)
- Critical Thinking: How to Effectively Reason, Understand Irrationality, and Make Better DecisionsFrom EverandCritical Thinking: How to Effectively Reason, Understand Irrationality, and Make Better DecisionsRating: 4.5 out of 5 stars4.5/5 (38)
- My Grandmother's Hands: Racialized Trauma and the Pathway to Mending Our Hearts and BodiesFrom EverandMy Grandmother's Hands: Racialized Trauma and the Pathway to Mending Our Hearts and BodiesRating: 5 out of 5 stars5/5 (70)
- Feel the Fear… and Do It Anyway: Dynamic Techniques for Turning Fear, Indecision, and Anger into Power, Action, and LoveFrom EverandFeel the Fear… and Do It Anyway: Dynamic Techniques for Turning Fear, Indecision, and Anger into Power, Action, and LoveRating: 4 out of 5 stars4/5 (249)
- Somatic Therapy Workbook: A Step-by-Step Guide to Experiencing Greater Mind-Body ConnectionFrom EverandSomatic Therapy Workbook: A Step-by-Step Guide to Experiencing Greater Mind-Body ConnectionNo ratings yet
- The Upward Spiral: Using Neuroscience to Reverse the Course of Depression, One Small Change at a TimeFrom EverandThe Upward Spiral: Using Neuroscience to Reverse the Course of Depression, One Small Change at a TimeRating: 4.5 out of 5 stars4.5/5 (140)
- Summary: The Myth of Normal: Trauma, Illness, and Healing in a Toxic Culture By Gabor Maté MD & Daniel Maté: Key Takeaways, Summary & AnalysisFrom EverandSummary: The Myth of Normal: Trauma, Illness, and Healing in a Toxic Culture By Gabor Maté MD & Daniel Maté: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (9)
- When Religion Hurts You: Healing from Religious Trauma and the Impact of High-Control ReligionFrom EverandWhen Religion Hurts You: Healing from Religious Trauma and the Impact of High-Control ReligionRating: 4 out of 5 stars4/5 (11)
- Insecure in Love: How Anxious Attachment Can Make You Feel Jealous, Needy, and Worried and What You Can Do About ItFrom EverandInsecure in Love: How Anxious Attachment Can Make You Feel Jealous, Needy, and Worried and What You Can Do About ItRating: 4.5 out of 5 stars4.5/5 (84)
- The Complex PTSD Workbook: A Mind-Body Approach to Regaining Emotional Control & Becoming WholeFrom EverandThe Complex PTSD Workbook: A Mind-Body Approach to Regaining Emotional Control & Becoming WholeRating: 4.5 out of 5 stars4.5/5 (49)
- Don't Panic: Taking Control of Anxiety AttacksFrom EverandDon't Panic: Taking Control of Anxiety AttacksRating: 4 out of 5 stars4/5 (12)
- Heal the Body, Heal the Mind: A Somatic Approach to Moving Beyond TraumaFrom EverandHeal the Body, Heal the Mind: A Somatic Approach to Moving Beyond TraumaRating: 4.5 out of 5 stars4.5/5 (56)
- BORDERLINE PERSONALITY DISORDER: Help Yourself and Help Others. Articulate Guide to BPD. Tools and Techniques to Control Emotions, Anger, and Mood Swings. Save All Your Relationships and Yourself. NEW VERSIONFrom EverandBORDERLINE PERSONALITY DISORDER: Help Yourself and Help Others. Articulate Guide to BPD. Tools and Techniques to Control Emotions, Anger, and Mood Swings. Save All Your Relationships and Yourself. NEW VERSIONRating: 4.5 out of 5 stars4.5/5 (24)
- The Anatomy of Loneliness: How to Find Your Way Back to ConnectionFrom EverandThe Anatomy of Loneliness: How to Find Your Way Back to ConnectionRating: 4.5 out of 5 stars4.5/5 (162)
- Winning the War in Your Mind: Change Your Thinking, Change Your LifeFrom EverandWinning the War in Your Mind: Change Your Thinking, Change Your LifeRating: 5 out of 5 stars5/5 (558)
- Overcoming Unwanted Intrusive Thoughts: A CBT-Based Guide to Getting Over Frightening, Obsessive, or Disturbing ThoughtsFrom EverandOvercoming Unwanted Intrusive Thoughts: A CBT-Based Guide to Getting Over Frightening, Obsessive, or Disturbing ThoughtsRating: 4.5 out of 5 stars4.5/5 (48)
- Smart Phone Dumb Phone: Free Yourself from Digital AddictionFrom EverandSmart Phone Dumb Phone: Free Yourself from Digital AddictionRating: 5 out of 5 stars5/5 (11)
- Summary: No Bad Parts: Healing Trauma and Restoring Wholeness with the Internal Family Systems Model by Richard C. Schwartz PhD & Alanis Morissette: Key Takeaways, Summary & AnalysisFrom EverandSummary: No Bad Parts: Healing Trauma and Restoring Wholeness with the Internal Family Systems Model by Richard C. Schwartz PhD & Alanis Morissette: Key Takeaways, Summary & AnalysisRating: 5 out of 5 stars5/5 (5)
- Fighting Words Devotional: 100 Days of Speaking Truth into the DarknessFrom EverandFighting Words Devotional: 100 Days of Speaking Truth into the DarknessRating: 5 out of 5 stars5/5 (6)
- Are You Really OK?: Getting Real About Who You Are, How You’re Doing, and Why It MattersFrom EverandAre You Really OK?: Getting Real About Who You Are, How You’re Doing, and Why It MattersRating: 5 out of 5 stars5/5 (28)
- Anxious for Nothing: Finding Calm in a Chaotic WorldFrom EverandAnxious for Nothing: Finding Calm in a Chaotic WorldRating: 4.5 out of 5 stars4.5/5 (1243)