You might also like
- The Qualitative Estimation of BCR-ABL Transcript: An In-Lab Procedural Study on Leukemia PatientsFrom EverandThe Qualitative Estimation of BCR-ABL Transcript: An In-Lab Procedural Study on Leukemia PatientsNo ratings yet
- Hematological Profile of Sickle Cell Disorder in Tertiary Care HospitalDocument4 pagesHematological Profile of Sickle Cell Disorder in Tertiary Care HospitalIOSRjournalNo ratings yet
- An Etiological Reappraisal of Pancytopenia - LargestDocument9 pagesAn Etiological Reappraisal of Pancytopenia - LargestKaye Antonette AntioquiaNo ratings yet
- Diagnosis of Blood and Bone Marrow DisordersFrom EverandDiagnosis of Blood and Bone Marrow DisordersSa A. WangNo ratings yet
- A Clinicohaematological Profile of Splenomegaly: Varsha S. Dabadghao, Arundhati G.Diwan, Amol M. RaskarDocument9 pagesA Clinicohaematological Profile of Splenomegaly: Varsha S. Dabadghao, Arundhati G.Diwan, Amol M. RaskarLianSiahaanNo ratings yet
- Evaluation of Hematological Parameters and Bone Marrow in Indian Patients Suffering From PancytopeniaDocument15 pagesEvaluation of Hematological Parameters and Bone Marrow in Indian Patients Suffering From PancytopeniaJUAN PABLONo ratings yet
- Thrombocytopenia in Plasmodium Falciparum MalariaDocument3 pagesThrombocytopenia in Plasmodium Falciparum MalariaArja' WaasNo ratings yet
- PVDI Scientific AbstractsDocument2 pagesPVDI Scientific AbstractsBombinTallerdeTeatroNo ratings yet
- To Study The Hematological Profile in Patients With Alcoholic Liver Cirrhosis in A Tertiary Care Hospital in ManipurDocument9 pagesTo Study The Hematological Profile in Patients With Alcoholic Liver Cirrhosis in A Tertiary Care Hospital in ManipurIJAR JOURNALNo ratings yet
- 2Document6 pages2Srinath M VNo ratings yet
- Spectrum of Thalassemia Syndromes and Abnormal Haemoglobins in Adult PatientDocument4 pagesSpectrum of Thalassemia Syndromes and Abnormal Haemoglobins in Adult PatientBharat MahajanNo ratings yet
- Case Report: Autoimmune Hemolytic Anemia and Hodgkin's Disease: An Unusual Pediatric AssociationDocument3 pagesCase Report: Autoimmune Hemolytic Anemia and Hodgkin's Disease: An Unusual Pediatric AssociationFega ArabelaNo ratings yet
- Summary of Summary 5Document36 pagesSummary of Summary 5anon-265120100% (2)
- Hematological Parameters and Prevalence of Anemia Among Free-Living Elderly in South BrazilDocument4 pagesHematological Parameters and Prevalence of Anemia Among Free-Living Elderly in South BrazilEmy YulianaNo ratings yet
- Clinico-Aetiological Profile of Pancytopenia in Paediatric PracticeDocument4 pagesClinico-Aetiological Profile of Pancytopenia in Paediatric PracticeDesi AdiyatiNo ratings yet
- Nailfold Capillaroscopy in Behçet's Disease, AnalysisDocument3 pagesNailfold Capillaroscopy in Behçet's Disease, AnalysisAlinaBNo ratings yet
- 100015IJBTIWI2015 WoldieDocument5 pages100015IJBTIWI2015 WoldieSigrid MiNo ratings yet
- Bone Marrow Evaluation of Patients Having Pancytopenia at Tertiary Care Center, M. Y. Hospital, Indore, India: One-Year StudyDocument4 pagesBone Marrow Evaluation of Patients Having Pancytopenia at Tertiary Care Center, M. Y. Hospital, Indore, India: One-Year StudyivanNo ratings yet
- Complementary and Alternative Medical Lab Testing Part 16: HematologyFrom EverandComplementary and Alternative Medical Lab Testing Part 16: HematologyNo ratings yet
- Pancytopenia: A Clinico Hematological Study: Gayathri B N, Kadam Satyanarayan RaoDocument6 pagesPancytopenia: A Clinico Hematological Study: Gayathri B N, Kadam Satyanarayan RaoYeni PuspitasariNo ratings yet
- Complementary and Alternative Medical Lab Testing Part 3: CardiologyFrom EverandComplementary and Alternative Medical Lab Testing Part 3: CardiologyRating: 1 out of 5 stars1/5 (1)
- 8 PDFDocument8 pages8 PDFBaru Chandrasekhar RaoNo ratings yet
- Comparative Evaluation of Blood Parameters in Chronic Periodontitis Patients and Healthy Patients For Signs of AnemiaDocument7 pagesComparative Evaluation of Blood Parameters in Chronic Periodontitis Patients and Healthy Patients For Signs of AnemiaInternational Organization of Scientific Research (IOSR)No ratings yet
- Misra 2012Document7 pagesMisra 2012Carlos RiquelmeNo ratings yet
- Pharmaceutical SciencesDocument6 pagesPharmaceutical SciencesiajpsNo ratings yet
- DR T Dinesh Guide DR Baba YelkeDocument27 pagesDR T Dinesh Guide DR Baba YelkeDinesh AshwinNo ratings yet
- 2.Applied-Elevated Serum Acid Phosphatase-Mamta YadavDocument4 pages2.Applied-Elevated Serum Acid Phosphatase-Mamta YadavImpact JournalsNo ratings yet
- Study of Anemia Among Hemophilia Patients: Original ArticleDocument3 pagesStudy of Anemia Among Hemophilia Patients: Original ArticleyouyouNo ratings yet
- Pancytopenia As Initial Presentation of Acute Lymphoblastic Leukemia and Its Associationwith Bone MarrowresponseDocument6 pagesPancytopenia As Initial Presentation of Acute Lymphoblastic Leukemia and Its Associationwith Bone MarrowresponseIJAR JOURNALNo ratings yet
- Hypercalcemia Leukocytosis SyndromeDocument7 pagesHypercalcemia Leukocytosis SyndromeTun MahadankNo ratings yet
- Study of Spectrum of Hemoglobinopathies in Adult Age Group Diagnosed On High Performance Liquid Chromatography in Tertiary Care HospitalDocument9 pagesStudy of Spectrum of Hemoglobinopathies in Adult Age Group Diagnosed On High Performance Liquid Chromatography in Tertiary Care HospitalIJAR JOURNALNo ratings yet
- Clinical Manifestation in Sickle Cell Anemia: A Study in Chhattisgarh Institute of Medical Sciences (CIMS) Bilaspur, Chhattisgarh, India.Document4 pagesClinical Manifestation in Sickle Cell Anemia: A Study in Chhattisgarh Institute of Medical Sciences (CIMS) Bilaspur, Chhattisgarh, India.IOSRjournalNo ratings yet
- Buttarello-2016-International Journal of Laboratory HematologyDocument10 pagesButtarello-2016-International Journal of Laboratory HematologyLaurentiusJohanNo ratings yet
- Levels of Markers of Myocardial Infarction and Atherogenicity in Individuals With Sickle Cell TraitDocument6 pagesLevels of Markers of Myocardial Infarction and Atherogenicity in Individuals With Sickle Cell TraitKIU PUBLICATION AND EXTENSIONNo ratings yet
- A Study of Thrombocytopenia in Malaria and Its Prognostic SignificanceDocument6 pagesA Study of Thrombocytopenia in Malaria and Its Prognostic SignificanceBobby Faisyal RakhmanNo ratings yet
- Hema 6Document7 pagesHema 6yanuarizkaNo ratings yet
- Pancytopenia - A Clinicopathological Analysis of 132 CasesDocument11 pagesPancytopenia - A Clinicopathological Analysis of 132 CasesKaye Antonette AntioquiaNo ratings yet
- ArtLinfoma InfolenteDocument5 pagesArtLinfoma InfolenteSamy De La Cruz SánchezNo ratings yet
- Hyperbilirubinemia: A Risk Factor For Infection in The Surgical Intensive Care UnitDocument14 pagesHyperbilirubinemia: A Risk Factor For Infection in The Surgical Intensive Care UnitChristian Karl B. LlanesNo ratings yet
- Pancytopenia A Clinico Hematological StudyDocument6 pagesPancytopenia A Clinico Hematological StudyUci Rahmadhani MNo ratings yet
- Naskah PublikasiDocument14 pagesNaskah PublikasiAyuratna SariNo ratings yet
- Laboratory Features of Systemic Lupus Erythematosus (SLE)Document6 pagesLaboratory Features of Systemic Lupus Erythematosus (SLE)AmrKamalNo ratings yet
- Brief CommunicationDocument3 pagesBrief CommunicationanrihmNo ratings yet
- A Study of Mean Platelet Volume As A Prognostic Marker in SepsisDocument3 pagesA Study of Mean Platelet Volume As A Prognostic Marker in SepsisIjsrnet EditorialNo ratings yet
- IndianJClinExpOphthalmol 6-4-497 500Document4 pagesIndianJClinExpOphthalmol 6-4-497 500Yogesh SinghNo ratings yet
- Rekam Anusha Et Al.Document3 pagesRekam Anusha Et Al.International Journal of Clinical and Biomedical Research (IJCBR)No ratings yet
- Pleural Effusion in A Patient With End-Stage Renal Disease - PMCDocument5 pagesPleural Effusion in A Patient With End-Stage Renal Disease - PMCCasemix rsudwaledNo ratings yet
- Original Article: Study of RBC Histogram in Various AnemiasDocument14 pagesOriginal Article: Study of RBC Histogram in Various AnemiasSirishaNo ratings yet
- Chen 2013Document6 pagesChen 2013malaNo ratings yet
- Diagnostic Approach for PancytopeniaDocument7 pagesDiagnostic Approach for PancytopeniaDani BelloNo ratings yet
- 2015 Takeuchi BMCPediatricsDocument9 pages2015 Takeuchi BMCPediatricsEduardo PasteneNo ratings yet
- HS BCSH Sept 2011Document40 pagesHS BCSH Sept 2011lidya_zhuangNo ratings yet
- Study of Hematological Parameters in Patients With Non-Hematological Malignancies and Their Correlation With Stage of The DiseaseDocument7 pagesStudy of Hematological Parameters in Patients With Non-Hematological Malignancies and Their Correlation With Stage of The DiseaseIJAR JOURNALNo ratings yet
- Abnormalities in Collagen Composition May Contribute To The Pathogenesis of Hemorrhoids: Morphometric AnalysisDocument5 pagesAbnormalities in Collagen Composition May Contribute To The Pathogenesis of Hemorrhoids: Morphometric Analysiseka henny suryaniNo ratings yet
- Pulmonary Tuberculosis and Its Haematological Correlates-1Document8 pagesPulmonary Tuberculosis and Its Haematological Correlates-1mentari_64No ratings yet
- Myelodysplastic Syndromes: Diagnosis, Prognosis, and TreatmentDocument11 pagesMyelodysplastic Syndromes: Diagnosis, Prognosis, and TreatmentTataNo ratings yet
- Allopurinol and Mortality in Hyperuricaemic Patients: Concise ReportDocument3 pagesAllopurinol and Mortality in Hyperuricaemic Patients: Concise ReporterilarchiNo ratings yet
- Low Systemic Vascular ResistanceDocument7 pagesLow Systemic Vascular ResistanceMuhammad BadrushshalihNo ratings yet
- Institute of Medical Education Technology and Teachers' TrainingDocument1 pageInstitute of Medical Education Technology and Teachers' TrainingdvenumohanNo ratings yet
- 1000 MCQ Bank for Palestine Faculty of MedicineDocument161 pages1000 MCQ Bank for Palestine Faculty of MedicineMuhsen Muneer89% (9)
- Scope of Research in Physiotherapy by DR - Ajay Midde of Kims HospitalDocument33 pagesScope of Research in Physiotherapy by DR - Ajay Midde of Kims HospitaldvenumohanNo ratings yet
- Research SyllabusDocument2 pagesResearch SyllabusdvenumohanNo ratings yet
- Scope of Physiotherapy in Government and Non Government Scheme S and New Trends in Private SectorDocument24 pagesScope of Physiotherapy in Government and Non Government Scheme S and New Trends in Private SectordvenumohanNo ratings yet
- Rehabilitation Guidelines For Total Hip (Anterior) ArthroplastyDocument4 pagesRehabilitation Guidelines For Total Hip (Anterior) ArthroplastydvenumohanNo ratings yet
- Sigma Medicare Systems: Quotation / Proforma InvoiceDocument17 pagesSigma Medicare Systems: Quotation / Proforma InvoicedvenumohanNo ratings yet
- Google Classroom PPT For TeachersDocument39 pagesGoogle Classroom PPT For TeachersMartin FranciscoNo ratings yet
- #KCRInsults ConstitutionDocument4 pages#KCRInsults ConstitutiondvenumohanNo ratings yet
- Clinical Reasoning and Neurodynamic Testing and Treatment-ShacklockDocument67 pagesClinical Reasoning and Neurodynamic Testing and Treatment-ShacklockSeda Joseph SaineNo ratings yet
- 1 Electric Force and Electric FieldDocument52 pages1 Electric Force and Electric FieldKhalid mohammed khalil KhabourNo ratings yet
- ICF-Ankle Trimalleolar (Cotton's) Fracture RehabDocument18 pagesICF-Ankle Trimalleolar (Cotton's) Fracture RehabdvenumohanNo ratings yet
- Registration for Neuro Dynamics Workshop in PuneDocument23 pagesRegistration for Neuro Dynamics Workshop in PunedvenumohanNo ratings yet
- Institute of Medical Education Technology and Teachers' TrainingDocument1 pageInstitute of Medical Education Technology and Teachers' TrainingdvenumohanNo ratings yet
- Mechanical Properties MCQsDocument2 pagesMechanical Properties MCQsKavin BalasubramaniamNo ratings yet
- Course Duration: Diploma in Beauty Culture: 4 Months (288 HRS)Document3 pagesCourse Duration: Diploma in Beauty Culture: 4 Months (288 HRS)dvenumohanNo ratings yet
- Flexor Tendon Repairs Zones I III 05-13-2013Document3 pagesFlexor Tendon Repairs Zones I III 05-13-2013Mihaela DoniciNo ratings yet
- Mobile BrochureDocument8 pagesMobile BrochuredvenumohanNo ratings yet
- Diwali PowerPointDocument30 pagesDiwali PowerPointakash baviskarNo ratings yet
- Diwali the+Festival+of+LightsDocument12 pagesDiwali the+Festival+of+LightsdvenumohanNo ratings yet
- Diwali: 28 October 2008 WALT Understand The Meaning of The Festival of DiwaliDocument11 pagesDiwali: 28 October 2008 WALT Understand The Meaning of The Festival of DiwalidvenumohanNo ratings yet
- Shortwave Diathermy: Prof. Dr. Gehan MosaadDocument29 pagesShortwave Diathermy: Prof. Dr. Gehan MosaaddvenumohanNo ratings yet
- Agency Energy Conservation ChecklistDocument2 pagesAgency Energy Conservation ChecklistdvenumohanNo ratings yet
- Diwali PowerPointDocument30 pagesDiwali PowerPointakash baviskarNo ratings yet
- Scope of Research in Physiotherapy by DR - Ajay Midde of Kims HospitalDocument33 pagesScope of Research in Physiotherapy by DR - Ajay Midde of Kims HospitaldvenumohanNo ratings yet
- Reliability of Clinical Tests To Evaluate Nerve Function and Mechanosensitivity of The Upper Limb Peripheral Nervous SystemDocument10 pagesReliability of Clinical Tests To Evaluate Nerve Function and Mechanosensitivity of The Upper Limb Peripheral Nervous SystemdvenumohanNo ratings yet
- Diwali the+Festival+of+LightsDocument12 pagesDiwali the+Festival+of+LightsdvenumohanNo ratings yet
- PH D Circular For Title and Synopsis 270921Document2 pagesPH D Circular For Title and Synopsis 270921dvenumohanNo ratings yet
- Intelect NMesDocument28 pagesIntelect NMesJuan CamiloNo ratings yet
- Reliability and Validity of Agility Tests for Team SportsDocument6 pagesReliability and Validity of Agility Tests for Team SportsdvenumohanNo ratings yet
- MODULE 4 (Basics of STI, HIV & AIDS)Document45 pagesMODULE 4 (Basics of STI, HIV & AIDS)Mark Johnuel Duavis100% (2)
- Journal 1Document2 pagesJournal 1Intan KartikasariNo ratings yet
- Peran Dan Fungsi IPCNDocument30 pagesPeran Dan Fungsi IPCNNurAnizhaNo ratings yet
- COVID-19 Diagnostic ReportDocument2 pagesCOVID-19 Diagnostic ReportSheetalNo ratings yet
- Avian Influenza in ChickensDocument19 pagesAvian Influenza in ChickensShah NawazNo ratings yet
- Farmakoterapi Penyakit Infeksi: in Infectious Diseases Dewi Rahmawati, M.Farm-Klin.,AptDocument87 pagesFarmakoterapi Penyakit Infeksi: in Infectious Diseases Dewi Rahmawati, M.Farm-Klin.,AptYemima MNo ratings yet
- Tuberculin Skin TestDocument14 pagesTuberculin Skin TestKaioNo ratings yet
- POGI Infection in Pregnancy 2022Document93 pagesPOGI Infection in Pregnancy 2022SDM RSTINo ratings yet
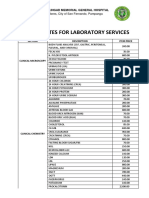
- JBLMGH Rates For Laboratory Services: Jose B. Lingad Memorial General HospitalDocument4 pagesJBLMGH Rates For Laboratory Services: Jose B. Lingad Memorial General HospitalApril NNo ratings yet
- Rubella and PregnancyDocument6 pagesRubella and PregnancyKABERA RENENo ratings yet
- 4.4 Emerging and Re-emerging Infectious DiseaseDocument75 pages4.4 Emerging and Re-emerging Infectious DiseasenorazlienaNo ratings yet
- Order Information Iwama, Moises: CommentsDocument1 pageOrder Information Iwama, Moises: CommentsLuis IwamaNo ratings yet
- Evaluation and Management of Young Febrile Infants 2023Document12 pagesEvaluation and Management of Young Febrile Infants 2023Felipe MayorcaNo ratings yet
- Signs and SymptomsDocument6 pagesSigns and Symptomsdareine22No ratings yet
- Early Diagnosis of Sepsis Using Serum Bio MarkersDocument5 pagesEarly Diagnosis of Sepsis Using Serum Bio Markersalemarques16No ratings yet
- Antifungal Breakpoints V 9.0 180212Document5 pagesAntifungal Breakpoints V 9.0 180212hergoNo ratings yet
- Immunology For AiimsDocument21 pagesImmunology For AiimssureshNo ratings yet
- ESKAPE Pathogen & AntibiogramDocument33 pagesESKAPE Pathogen & Antibiogramvijayasree bavireddyNo ratings yet
- DLL Mapeh g4 q2 w3Document6 pagesDLL Mapeh g4 q2 w3Daniel MingoyNo ratings yet
- Epi AssignmentDocument2 pagesEpi AssignmentStephanie BragatNo ratings yet
- OutbreakWksht UpdatedMay18 ADocument3 pagesOutbreakWksht UpdatedMay18 ASatya DwiparthaNo ratings yet
- Canine BabesiosisDocument10 pagesCanine BabesiosisIonuț Gabriel ȚoleaNo ratings yet
- Zika Virus FactsheetDocument2 pagesZika Virus Factsheetfriska_arianiNo ratings yet
- National Immunization ScheduleDocument4 pagesNational Immunization ScheduleKenneth Ralph UrbanNo ratings yet
- Autoimmune DiseasesDocument4 pagesAutoimmune DiseasesMahak JandwaniNo ratings yet
- Eji 201847659Document7 pagesEji 201847659marjoranovaNo ratings yet
- Lyme Disease Brochure TemplateDocument2 pagesLyme Disease Brochure Templatetburkle50% (2)
- Fever and RashDocument14 pagesFever and RashwirdahajaNo ratings yet
- Eurl Rhesus Lab: Listing Des Reactifs Et Consommables Snibe 2021Document5 pagesEurl Rhesus Lab: Listing Des Reactifs Et Consommables Snibe 2021Fateh AzwiNo ratings yet