You might also like
- Claim Form For Health Insurance Policies: The Issue of This Form Is Not To Be Taken As An Admission of LiabilityDocument4 pagesClaim Form For Health Insurance Policies: The Issue of This Form Is Not To Be Taken As An Admission of LiabilityShail ThakkarNo ratings yet
- Standard Claim Form Insured PDFDocument2 pagesStandard Claim Form Insured PDFSadasivuni007No ratings yet
- IRDA Claim FormDocument4 pagesIRDA Claim FormSatya SundarNo ratings yet
- Bill No Date Issued by Towards Amount (RS)Document4 pagesBill No Date Issued by Towards Amount (RS)mm8871No ratings yet
- Bill No Date Issued by Towards Amount (RS)Document4 pagesBill No Date Issued by Towards Amount (RS)SMNo ratings yet
- NAIC ClaimFormDocument4 pagesNAIC ClaimFormVinamra JaiswalNo ratings yet
- IRDA Reimbursement Claim FormDocument4 pagesIRDA Reimbursement Claim FormsumitNo ratings yet
- Claim DocumentDocument5 pagesClaim DocumentVishwas SharmaNo ratings yet
- Name of Insurance CompanyDocument3 pagesName of Insurance CompanyAnkit JainNo ratings yet
- Reimbursement Claim Form PDFDocument2 pagesReimbursement Claim Form PDFCHARLES MATHEWNo ratings yet
- MDIndia Claim FormDocument2 pagesMDIndia Claim FormSalil PatelNo ratings yet
- IRDA - Claim FormDocument4 pagesIRDA - Claim FormweblogicdocsNo ratings yet
- IRDA Reimbursement Claim Form - InsuredDocument2 pagesIRDA Reimbursement Claim Form - InsuredroshanNo ratings yet
- Health Claim FormDocument6 pagesHealth Claim Formqw qwNo ratings yet
- Reimbursement Claim Form VidalDocument3 pagesReimbursement Claim Form Vidalsarv2kNo ratings yet
- Inhouse TPA - Claim FormDocument2 pagesInhouse TPA - Claim FormJanarthanan KNo ratings yet
- Policy ClaimformDocument5 pagesPolicy ClaimformharshNo ratings yet
- Reimbursement Claim FormDocument4 pagesReimbursement Claim FormhariharanccetNo ratings yet
- State: Pin Code: Phone No: Email ID:: DateDocument4 pagesState: Pin Code: Phone No: Email ID:: DateChetan Vamshi MopuriNo ratings yet
- State: Pin Code: Phone No: Email ID:: DateDocument2 pagesState: Pin Code: Phone No: Email ID:: DateRatheesh TNo ratings yet
- Reimbursement Claim FormDocument2 pagesReimbursement Claim FormOmpalNo ratings yet
- HDFC ERGO General Insurance Company Limited: Claim Form - Part ADocument7 pagesHDFC ERGO General Insurance Company Limited: Claim Form - Part Aharsh SharmaNo ratings yet
- Claim Form - Part A: To Be Filled in by The InsuredDocument2 pagesClaim Form - Part A: To Be Filled in by The InsuredAli ArsalaanNo ratings yet
- Vipul Corp Lnsurance TPA PVT LTD.: Details of Insurance HistoryDocument4 pagesVipul Corp Lnsurance TPA PVT LTD.: Details of Insurance HistoryVediappan Alies RajaNo ratings yet
- Claim Form - Part A' To 'Claim Form For Health Insurance PolicyDocument6 pagesClaim Form - Part A' To 'Claim Form For Health Insurance PolicypawanNo ratings yet
- NICClaimForm PDFDocument2 pagesNICClaimForm PDFsanNo ratings yet
- Ericson TPA All Details For Existing Employees For 2022-23-1Document652 pagesEricson TPA All Details For Existing Employees For 2022-23-1Rohit AggarwalNo ratings yet
- Reimbursement CLaim Form IRDADocument5 pagesReimbursement CLaim Form IRDADhaval ThakkarNo ratings yet
- NIC Claim FormDocument4 pagesNIC Claim FormImtiazNo ratings yet
- HDFC ERGO General Insurance Company Limited: Claim Form - Part ADocument4 pagesHDFC ERGO General Insurance Company Limited: Claim Form - Part Avizag mdindiaNo ratings yet
- Claim Form Dhs ReimbursementDocument4 pagesClaim Form Dhs ReimbursementLakshmi NarasaiahNo ratings yet
- Claim Form DHS Reimbursement PDFDocument4 pagesClaim Form DHS Reimbursement PDFLakshmi NarasaiahNo ratings yet
- IRDA Reimbursement Claim FormDocument2 pagesIRDA Reimbursement Claim FormVaibhav PawarNo ratings yet
- Reimbursement Claim Form PDFDocument2 pagesReimbursement Claim Form PDFKen KhumanchaNo ratings yet
- Iffco Tokio ClaimFormDocument4 pagesIffco Tokio ClaimFormRaju.PalNo ratings yet
- IRDA - Sample Claim Form Highlighted Guidelines.Document5 pagesIRDA - Sample Claim Form Highlighted Guidelines.hariNo ratings yet
- Reimbursement - Claim - Form and Check List RandstadDocument3 pagesReimbursement - Claim - Form and Check List RandstadSajed AliNo ratings yet
- Claim Form - Part A' To 'Claim Form For Health Insurance PolicyDocument6 pagesClaim Form - Part A' To 'Claim Form For Health Insurance Policyanil sangwanNo ratings yet
- Claim Form 10 - EditableDocument7 pagesClaim Form 10 - EditableharshiNo ratings yet
- Claim Form - Part A' To 'Claim Form For Health Insurance PolicyDocument6 pagesClaim Form - Part A' To 'Claim Form For Health Insurance PolicySudipta DeNo ratings yet
- Reimbursement Claim Form-1Document7 pagesReimbursement Claim Form-1Mayuresh DalviNo ratings yet
- Claim Form - Part A' To 'Claim Form For Health Insurance PolicyDocument6 pagesClaim Form - Part A' To 'Claim Form For Health Insurance PolicyArunsNo ratings yet
- E Claim FormDocument8 pagesE Claim FormronNo ratings yet
- Claim Form For Health Insurance Policies - Part A Name of Insurance Company: Client NameDocument4 pagesClaim Form For Health Insurance Policies - Part A Name of Insurance Company: Client NameSatyadev KalraNo ratings yet
- Claim Form - Part A' To 'Claim Form For Health Insurance PolicyDocument6 pagesClaim Form - Part A' To 'Claim Form For Health Insurance PolicyMruthunjaya Reddy LakkamNo ratings yet
- Medi Assist Reimbursement Claim FormDocument5 pagesMedi Assist Reimbursement Claim FormRam MedarametlaNo ratings yet
- Reimbursement Claim FormDocument2 pagesReimbursement Claim FormprabhakarNo ratings yet
- Reimbursement Claim FormDocument2 pagesReimbursement Claim FormanjnaNo ratings yet
- Medi Assist Complete FormDocument4 pagesMedi Assist Complete FormKhushi ChauhanNo ratings yet
- Reimbursement Claim FormDocument3 pagesReimbursement Claim FormGanesh Kumar100% (1)
- Health Claim FormDocument2 pagesHealth Claim FormtharunNo ratings yet
- Details of Primary Insured: Claim Form - Part A' To 'Claim Form For Health Insurance PolicyDocument5 pagesDetails of Primary Insured: Claim Form - Part A' To 'Claim Form For Health Insurance PolicyRummy RajaNo ratings yet
- Myhealth-Suraksha-Claim-Form (1) - RemovedDocument2 pagesMyhealth-Suraksha-Claim-Form (1) - Removedaditya727No ratings yet
- Myhealth Suraksha Claim FormDocument5 pagesMyhealth Suraksha Claim Formaditya727No ratings yet
- Claim Form - Part A' To 'Claim Form For Health Insurance Policies Other Than Travel and Personal Accident - Part ADocument7 pagesClaim Form - Part A' To 'Claim Form For Health Insurance Policies Other Than Travel and Personal Accident - Part AkannagamNo ratings yet
- Florida Real Estate Exam Prep: Everything You Need to Know to PassFrom EverandFlorida Real Estate Exam Prep: Everything You Need to Know to PassNo ratings yet
- Interview Skills Guidebook GeneralDocument21 pagesInterview Skills Guidebook GeneralTrinetra AgarwalNo ratings yet
- Trinetra Ditto ResumeDocument1 pageTrinetra Ditto ResumeTrinetra AgarwalNo ratings yet
- Trinetra Ditto ResumeDocument1 pageTrinetra Ditto ResumeTrinetra AgarwalNo ratings yet
- LinksDocument2 pagesLinksTrinetra AgarwalNo ratings yet
- Internshala Resume Template1Document2 pagesInternshala Resume Template1shashi shekharNo ratings yet
- Health Insurance That Works For YouDocument5 pagesHealth Insurance That Works For YouTrinetra AgarwalNo ratings yet
- 30082019-Updated List of Service ChargesDocument12 pages30082019-Updated List of Service ChargesSanjay BhushanNo ratings yet
- Black Money Crackdown: Declare Your Foreign Assets, Income in Your ITRDocument2 pagesBlack Money Crackdown: Declare Your Foreign Assets, Income in Your ITRTrinetra AgarwalNo ratings yet
- Amazon Pay Guide Credit CardDocument5 pagesAmazon Pay Guide Credit CardTrinetra AgarwalNo ratings yet
- Elephone Irectory: Pawan Hans LimitedDocument19 pagesElephone Irectory: Pawan Hans LimitedYash SoniNo ratings yet
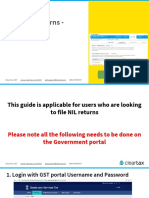
- Filing NIL Returns - GSTR 1Document15 pagesFiling NIL Returns - GSTR 1Trinetra AgarwalNo ratings yet
- Bought Property But Not Deposited TDS? You May Get A Tax NoticeDocument2 pagesBought Property But Not Deposited TDS? You May Get A Tax NoticeTrinetra AgarwalNo ratings yet
- SENIOR FIRST BROCHURE - Draft v7 - ProductsDocument6 pagesSENIOR FIRST BROCHURE - Draft v7 - ProductsTrinetra AgarwalNo ratings yet
- 28 - Best in Fin TechDocument1 page28 - Best in Fin TechTrinetra AgarwalNo ratings yet
- 28 - Best in Fin TechDocument1 page28 - Best in Fin TechTrinetra AgarwalNo ratings yet
- Amazon Pay Guide Credit CardDocument5 pagesAmazon Pay Guide Credit CardTrinetra AgarwalNo ratings yet
- GST E-Invoice SystemDocument21 pagesGST E-Invoice SystemTrinetra AgarwalNo ratings yet
- Amazon Pay Guide Credit CardDocument5 pagesAmazon Pay Guide Credit CardTrinetra AgarwalNo ratings yet
- A Complete Guide To E-Invoicing in India: BooksDocument19 pagesA Complete Guide To E-Invoicing in India: BooksTrinetra AgarwalNo ratings yet
- Pitch Anything Free Summary by Oren KlaffDocument9 pagesPitch Anything Free Summary by Oren KlaffTrinetra Agarwal100% (1)
- GST E Book PDFDocument63 pagesGST E Book PDFnaveen chaudharyNo ratings yet
- Fit For Success - Nick ShawDocument132 pagesFit For Success - Nick ShawLeon100% (4)
- Lead Your Firm To Success in The GST SystemDocument16 pagesLead Your Firm To Success in The GST SystemTrinetra AgarwalNo ratings yet
- Better Call Saul (Season 1) - WikipediaDocument19 pagesBetter Call Saul (Season 1) - WikipediaTrinetra AgarwalNo ratings yet
- GST E Book PDFDocument63 pagesGST E Book PDFnaveen chaudharyNo ratings yet
- A Complete Guide To E-Invoicing in India: BooksDocument19 pagesA Complete Guide To E-Invoicing in India: BooksTrinetra AgarwalNo ratings yet
- India TodayDocument68 pagesIndia TodayTrinetra AgarwalNo ratings yet
- Challenger Chinnamma: Sasikala's Return Could Upset AIADMK's PlansDocument39 pagesChallenger Chinnamma: Sasikala's Return Could Upset AIADMK's PlansTrinetra AgarwalNo ratings yet
- Family Health Floater PolicyDocument8 pagesFamily Health Floater PolicyTrinetra AgarwalNo ratings yet
- Bleeding in A NeonateDocument36 pagesBleeding in A NeonateDrBibek AgarwalNo ratings yet
- Pinch & Piston ValvesDocument8 pagesPinch & Piston ValvesJaldhij Patel100% (1)
- 20 Best Cognac CocktailsDocument1 page20 Best Cognac CocktailsHL XanticNo ratings yet
- Cor Tzar 2018Document12 pagesCor Tzar 2018alejandraNo ratings yet
- JAR Part 66 Examination Mod 03Document126 pagesJAR Part 66 Examination Mod 03Shreyas PingeNo ratings yet
- Case Study of Flixborough UK DisasterDocument52 pagesCase Study of Flixborough UK Disasteraman shaikhNo ratings yet
- Essential Intrapartum and Newborn CareDocument6 pagesEssential Intrapartum and Newborn CareDianne LabisNo ratings yet
- Case Analysis: Beth OwensDocument8 pagesCase Analysis: Beth OwensPhillip CookNo ratings yet
- Consolidation of ClayDocument17 pagesConsolidation of ClayMD Anan MorshedNo ratings yet
- 36 Petroland PD Serie DKDocument7 pages36 Petroland PD Serie DKBayu RahmansyahNo ratings yet
- Sore Throat, Hoarseness and Otitis MediaDocument19 pagesSore Throat, Hoarseness and Otitis MediaainaNo ratings yet
- Bonsai TreesDocument19 pagesBonsai TreesMayur ChoudhariNo ratings yet
- Eric CHE326 JournalpptDocument33 pagesEric CHE326 JournalpptRugi Vicente RubiNo ratings yet
- Advances in Agronomy v.84Document333 pagesAdvances in Agronomy v.84luisiunesNo ratings yet
- Diagnostic Evaluation and Management of The Solitary Pulmonary NoduleDocument21 pagesDiagnostic Evaluation and Management of The Solitary Pulmonary NoduleGonzalo Leal100% (1)
- Theoretical Background: Theories Relevance To The Study SourcesDocument3 pagesTheoretical Background: Theories Relevance To The Study SourcesAdelfa Mae BerdonNo ratings yet
- Cervical Changes During Menstrual Cycle (Photos)Document9 pagesCervical Changes During Menstrual Cycle (Photos)divyanshu kumarNo ratings yet
- 13 Methods To Increase Your Conditioning - Strength by SkylerDocument5 pages13 Methods To Increase Your Conditioning - Strength by SkylerMarko Štambuk100% (1)
- Prestress 3.0Document10 pagesPrestress 3.0Jonel CorbiNo ratings yet
- Anatomy and Physiology Chapter 2Document28 pagesAnatomy and Physiology Chapter 2Marshalee FrancisNo ratings yet
- 20BCEC1109, 20BCE1170, 20BCE1233 - IOT Final ReportDocument40 pages20BCEC1109, 20BCE1170, 20BCE1233 - IOT Final Reportharsh chauhanNo ratings yet
- Economics Half Yearly Question PaperDocument6 pagesEconomics Half Yearly Question PaperBhumika MiglaniNo ratings yet
- Anti-Bribery and Corruption PolicyDocument2 pagesAnti-Bribery and Corruption PolicyAJAY PatilNo ratings yet
- Pay Structure of Public Employees in PakistanDocument28 pagesPay Structure of Public Employees in PakistanAamir50% (10)
- Red Bank Squadron - 01/22/1942Document28 pagesRed Bank Squadron - 01/22/1942CAP History LibraryNo ratings yet
- Aits 2324 Ot I Jeea TD Paper 2 OfflineDocument14 pagesAits 2324 Ot I Jeea TD Paper 2 OfflineAshish SharmaNo ratings yet
- Open Courses Myanmar Strategic English Week 4: U Yan Naing Se NyuntDocument24 pagesOpen Courses Myanmar Strategic English Week 4: U Yan Naing Se NyuntYan Naing Soe NyuntNo ratings yet
- Helicopter Logging Operations - ThesisDocument7 pagesHelicopter Logging Operations - ThesisAleš ŠtimecNo ratings yet
- 2012 U.S. History End-of-Course (EOC) Assessment Field Test Fact SheetDocument2 pages2012 U.S. History End-of-Course (EOC) Assessment Field Test Fact SheetswainanjanNo ratings yet
- Reading TOEFL - Short Reading Per Question TypeDocument25 pagesReading TOEFL - Short Reading Per Question Typejax7202No ratings yet