You might also like
- Analyzing Potential Audit Client LakesideDocument22 pagesAnalyzing Potential Audit Client LakesideLet it be100% (1)
- Step 5 - PragmaticsDocument7 pagesStep 5 - PragmaticsRomario García UrbinaNo ratings yet
- Rebels - in - Frills - A - Literature - Review - On 4Document93 pagesRebels - in - Frills - A - Literature - Review - On 4mariobogarinNo ratings yet
- BGDSV252C823MA211022Document2 pagesBGDSV252C823MA211022rubelquotex1996No ratings yet
- Indian Visa ApplicationDocument2 pagesIndian Visa ApplicationMd Kamruzzaman KhanNo ratings yet
- BGDDW467CA23MD010504Document2 pagesBGDDW467CA23MD010504Ridve AhmedNo ratings yet
- BGDDV676B723MD850101Document2 pagesBGDDV676B723MD850101Noor E Alam KibriaNo ratings yet
- BGDDV63E1724MS090112Document2 pagesBGDDV63E1724MS090112digitaltravelaNo ratings yet
- BGDDVCA0DA23RA790829Document2 pagesBGDDVCA0DA23RA790829Rahman ComputerNo ratings yet
- BGDDV63D7524RA020910Document2 pagesBGDDV63D7524RA020910digitaltravelaNo ratings yet
- BGDSV1150423BI891001Document2 pagesBGDSV1150423BI891001INDIAN VISANo ratings yet
- Dipali SahaDocument2 pagesDipali SahaMd Aminul AlamNo ratings yet
- High Commission of India: Visa Application FormDocument2 pagesHigh Commission of India: Visa Application FormAnonymous ZGcs7MwsLNo ratings yet
- Qab India Visa Aplcn FormDocument2 pagesQab India Visa Aplcn FormQurban Ali BulbulNo ratings yet
- BGDDV123D224MD700902Document2 pagesBGDDV123D224MD700902turkyvisapaymentNo ratings yet
- Visa Application Form: Assistant High Commission of IndiaDocument2 pagesVisa Application Form: Assistant High Commission of IndiaMd Kamruzzaman KhanNo ratings yet
- BGDDVF99B423MD990325Document2 pagesBGDDVF99B423MD990325Arif ZenNo ratings yet
- High Commission of India: Visa Application FormDocument2 pagesHigh Commission of India: Visa Application Formsaadehsan99No ratings yet
- BGDDV5B1E224MS900101Document2 pagesBGDDV5B1E224MS900101smhostbdcomNo ratings yet
- Nikhil Kumar BiswasDocument2 pagesNikhil Kumar BiswasMd Aminul AlamNo ratings yet
- BGDDV7404D24AN930710Document2 pagesBGDDV7404D24AN930710mdyasin786543No ratings yet
- Indian Visa ApplicationDocument2 pagesIndian Visa ApplicationMasud RanaNo ratings yet
- BGDCV3A27C23MO051109Document2 pagesBGDCV3A27C23MO051109rmc.labinfoNo ratings yet
- MD Abul Kalam Azad PDFDocument2 pagesMD Abul Kalam Azad PDFMd Aminul AlamNo ratings yet
- Indian Visa Application FormDocument2 pagesIndian Visa Application FormafNo ratings yet
- BGDDV4777923MD930101Document2 pagesBGDDV4777923MD930101rakibul islamNo ratings yet
- BGDDW4530F23MD990718Document2 pagesBGDDW4530F23MD990718mdfoysal12041996No ratings yet
- BGDDXECD4C17MD780702Document2 pagesBGDDXECD4C17MD780702Obayedullah MizanNo ratings yet
- High Commission of India: Visa Application FormDocument2 pagesHigh Commission of India: Visa Application Formahibadhaka2020No ratings yet
- High Commission of India: Visa Application FormDocument2 pagesHigh Commission of India: Visa Application FormJames AmirNo ratings yet
- BGDDV0B3BB24MD850104Document2 pagesBGDDV0B3BB24MD850104oppophotostatNo ratings yet
- High Commission of India: Visa Application FormDocument2 pagesHigh Commission of India: Visa Application FormTasnim AraNo ratings yet
- BGDDV1FD1923NO980711Document2 pagesBGDDV1FD1923NO980711Nowrid Bin AfazNo ratings yet
- INDIA VISA APPLICATIONDocument2 pagesINDIA VISA APPLICATIONalamgir80No ratings yet
- High Commission of India: Visa Application FormDocument2 pagesHigh Commission of India: Visa Application FormmahmudNo ratings yet
- BGDCV324F222MD820101Document2 pagesBGDCV324F222MD820101Muhammad Arifur RahmanNo ratings yet
- High Commission of India: Visa Application FormDocument2 pagesHigh Commission of India: Visa Application FormRonobir SarkerNo ratings yet
- Asst High Commission of India Rajshahi: Visa Application FormDocument2 pagesAsst High Commission of India Rajshahi: Visa Application Formalamgir80No ratings yet
- Indian Visa Application FormDocument2 pagesIndian Visa Application Formbosusabyasachi445No ratings yet
- MD Sowad KarimDocument2 pagesMD Sowad KarimMd Kamruzzaman KhanNo ratings yet
- Indian Visa ApplicationDocument2 pagesIndian Visa ApplicationGolam Samdanee TaneemNo ratings yet
- Indian Visa ApplicationDocument2 pagesIndian Visa Applicationalamgir80No ratings yet
- Indian Visa ApplicationDocument2 pagesIndian Visa Applicationvote 2015No ratings yet
- BGDRV25B8222MD761012Document2 pagesBGDRV25B8222MD761012alamgir80No ratings yet
- BGDDV22DCD24MD950101Document2 pagesBGDDV22DCD24MD950101mdyasin786543No ratings yet
- Indian Hospital Visa ApplicationDocument2 pagesIndian Hospital Visa ApplicationSaikat BiswasNo ratings yet
- Arnob GhoshDocument2 pagesArnob GhoshMd Kamruzzaman KhanNo ratings yet
- BGDDV2640619RO860610Document2 pagesBGDDV2640619RO860610mehedikhan21No ratings yet
- Selina BegumDocument2 pagesSelina BegumMd Aminul AlamNo ratings yet
- BGDDW1FEFA23MD890712Document2 pagesBGDDW1FEFA23MD890712Md.ZakariaNo ratings yet
- Indian Visa ApplicationDocument2 pagesIndian Visa ApplicationMd Aminul AlamNo ratings yet
- Visa Application FormDocument2 pagesVisa Application FormMd Kamruzzaman KhanNo ratings yet
- BGDCV30BA523MU990610Document2 pagesBGDCV30BA523MU990610Muhammad Mizanur RahmanNo ratings yet
- BGDDW04C9F23MD910911Document2 pagesBGDDW04C9F23MD910911noortele67No ratings yet
- High Commission of India: Visa Application FormDocument2 pagesHigh Commission of India: Visa Application FormRajanish BiswasNo ratings yet
- BGDDW6FBDD23MD790114Document2 pagesBGDDW6FBDD23MD790114noortele67No ratings yet
- Mohine AhmedDocument2 pagesMohine AhmedMd Aminul AlamNo ratings yet
- BGDDW6FD3623ZA131011Document2 pagesBGDDW6FD3623ZA131011noortele67No ratings yet
- AmranDocument2 pagesAmranOchana PothikNo ratings yet
- Indian Visa ApplicationDocument2 pagesIndian Visa Applicationalamgir80No ratings yet
- BGDR30313119BA811021Document2 pagesBGDR30313119BA811021alamgir80No ratings yet
- BGDDV4DAC324SA931118Document2 pagesBGDDV4DAC324SA931118Ehsaas RifatNo ratings yet
- Grade 6 Quarter 3 WHLP WEEK 4Document3 pagesGrade 6 Quarter 3 WHLP WEEK 4JaneDandanNo ratings yet
- English DWDM 2022 Book 7 Int Sample PagesDocument7 pagesEnglish DWDM 2022 Book 7 Int Sample PagesLuiz Roberto MartinesNo ratings yet
- Effects of The Sugar RevolutionDocument9 pagesEffects of The Sugar RevolutionSusan BarriotNo ratings yet
- Cad MCQ Unit 5Document3 pagesCad MCQ Unit 5ddeepak123No ratings yet
- All About The Hathras Case - IpleadersDocument1 pageAll About The Hathras Case - IpleadersBadhon Chandra SarkarNo ratings yet
- Lucid Dreaming Fast TrackDocument3 pagesLucid Dreaming Fast TrackWulan Funblogger50% (2)
- Prakash V MST SahaniDocument8 pagesPrakash V MST SahaniAditi IndraniNo ratings yet
- Kantar Worldpanel Division FMCG Monitor Q2 2022 EN Including Gift Shared-by-WorldLine-Technology-1Document13 pagesKantar Worldpanel Division FMCG Monitor Q2 2022 EN Including Gift Shared-by-WorldLine-Technology-1K59 Dau Minh VyNo ratings yet
- ED Review Test 4Document2 pagesED Review Test 4Huyen KimNo ratings yet
- Name of DrugDocument2 pagesName of Drugmonique fajardo100% (1)
- SHORLUBE Self Lubricating Bearings PDFDocument20 pagesSHORLUBE Self Lubricating Bearings PDFNickNo ratings yet
- Research Project On Capital PunishmentDocument6 pagesResearch Project On Capital PunishmentNitwit NoddyNo ratings yet
- Sales Confirmation: Alpha Trading S.P.A. Compagnie Tunisienne de NavigationDocument1 pageSales Confirmation: Alpha Trading S.P.A. Compagnie Tunisienne de NavigationimedNo ratings yet
- Persons Choki MotobuDocument4 pagesPersons Choki MotobuHessabi max100% (1)
- Jack Turner - Not On Any MapDocument13 pagesJack Turner - Not On Any MapormrNo ratings yet
- Oscillator Types and CharacteristicsDocument4 pagesOscillator Types and Characteristicspriyadarshini212007No ratings yet
- Sec. Gr. To BT History Temp Panel 2013Document50 pagesSec. Gr. To BT History Temp Panel 2013edwin_prakash75No ratings yet
- Journeys B2 Teacher's Resource Pack: Grammar ThemesDocument2 pagesJourneys B2 Teacher's Resource Pack: Grammar ThemesMiriam SanchezNo ratings yet
- 12th English Elec Lyp 2013 DelhiDocument10 pages12th English Elec Lyp 2013 DelhiKanishkha SivasankarNo ratings yet
- Vampire Stories in GreeceDocument21 pagesVampire Stories in GreeceΓιώργος ΣάρδηςNo ratings yet
- IT Industry in India: Indian Education SystemDocument9 pagesIT Industry in India: Indian Education SystemPradeep BommitiNo ratings yet
- Advanced Engineering Mathematics 10th EditionDocument7 pagesAdvanced Engineering Mathematics 10th EditionsamuelNo ratings yet
- Handout-Wisdom QuestionsDocument1 pageHandout-Wisdom Questionsapi-369459770No ratings yet
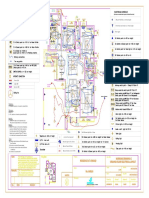
- Varun Valanjeri Electrical Layout-3Document1 pageVarun Valanjeri Electrical Layout-3ANOOP R NAIRNo ratings yet
- Distribution and Production of Rice in IndiaDocument6 pagesDistribution and Production of Rice in IndiaZehan SheikhNo ratings yet
- Information Prepared by The Project Gutenberg Legaladvisor: MokshaDocument2 pagesInformation Prepared by The Project Gutenberg Legaladvisor: MokshaMunnur PandariNo ratings yet
- Method of Statement For ELV SystemDocument7 pagesMethod of Statement For ELV SystemKo ZayNo ratings yet