You might also like
- Psych Nursing Complete Edited Royal PentagonDocument32 pagesPsych Nursing Complete Edited Royal PentagonRichard Ines Valino100% (68)
- The Red EyeDocument71 pagesThe Red Eyehenok biruk80% (5)
- Maternity Nursing Edited Royal PentagonDocument49 pagesMaternity Nursing Edited Royal PentagonRichard Ines Valino95% (38)
- 6th Central Pay Commission Salary CalculatorDocument15 pages6th Central Pay Commission Salary Calculatorrakhonde100% (436)
- Maternity Nursing Edited Royal PentagonDocument49 pagesMaternity Nursing Edited Royal PentagonRichard Ines Valino95% (38)
- 6th Central Pay Commission Salary CalculatorDocument15 pages6th Central Pay Commission Salary Calculatorrakhonde100% (436)
- Estate of Gerardo Gutierrez vs. PublixDocument12 pagesEstate of Gerardo Gutierrez vs. PublixPeterBurkeNo ratings yet
- Og - Applying To The Ndis v5.0 Approved - External 2023-09-28Document55 pagesOg - Applying To The Ndis v5.0 Approved - External 2023-09-28faithgaye432No ratings yet
- Red Eye - Student VersionDocument69 pagesRed Eye - Student VersionKreshnik HAJDARINo ratings yet
- Blefaritis EarlyDocument28 pagesBlefaritis EarlyPaomo Zhixia EarlyNo ratings yet
- Eye & Ear Medical TerminologyDocument2 pagesEye & Ear Medical TerminologyRizki Arniawati UlfahNo ratings yet
- The Red EyeDocument42 pagesThe Red EyeDenise CarbonellNo ratings yet
- Common Eye DiseasesDocument54 pagesCommon Eye Diseaseskyro draxNo ratings yet
- Red Eye Differential DiagnosisDocument70 pagesRed Eye Differential DiagnosisAdetz HaedetzNo ratings yet
- Diseases of The EyeDocument14 pagesDiseases of The EyeGunel AliyevaNo ratings yet
- Special Senses 2014 - 1Document91 pagesSpecial Senses 2014 - 1Winz DolleteNo ratings yet
- Corneal Reaction Towards Contact Lens Wear-2003poppyDocument6 pagesCorneal Reaction Towards Contact Lens Wear-2003poppyFeiruz Hamid Umar BahasywenNo ratings yet
- BlepharitisDocument20 pagesBlepharitisNorshahidah IedaNo ratings yet
- Corneal Dystrophies: Retinal DetachmentDocument5 pagesCorneal Dystrophies: Retinal DetachmentCake ManNo ratings yet
- DRY EYE AgungDocument23 pagesDRY EYE AgungGustiAngriAngalanNo ratings yet
- Care For Patients With Alteration in Perception and CoordinationDocument12 pagesCare For Patients With Alteration in Perception and Coordinationevlujtrep9690100% (1)
- Corneal Dystrophies, Contact Lenses, and Retinal Detachment GuideDocument6 pagesCorneal Dystrophies, Contact Lenses, and Retinal Detachment GuideMarissa AsimNo ratings yet
- Red EyeDocument54 pagesRed EyeT786 kharNo ratings yet
- Dry Eye Syndrome: Causes, Symptoms and Treatment in 40 CharactersDocument8 pagesDry Eye Syndrome: Causes, Symptoms and Treatment in 40 CharactersMuhammad AwaluddinNo ratings yet
- Ocular Emergencies: DR Sathiyan Karunanithi MD (Aiims) Ophthalmologist and Retinal SurgeonDocument57 pagesOcular Emergencies: DR Sathiyan Karunanithi MD (Aiims) Ophthalmologist and Retinal SurgeonAdithi SathiyanNo ratings yet
- Eye and Ear Disorders UpdatedDocument78 pagesEye and Ear Disorders Updatedjose arreolaNo ratings yet
- Ocular EmergDocument61 pagesOcular EmergKBR RS UNHAS100% (1)
- Dry Eye AgungDocument23 pagesDry Eye AgungAgung TriatmojoNo ratings yet
- DRY EYE AgungDocument23 pagesDRY EYE AgungGustiAngriAngalanNo ratings yet
- Blepharitis - Medical Disability GuidelinesDocument3 pagesBlepharitis - Medical Disability GuidelinesFerni ArmantiNo ratings yet
- Red Eye - Conjunctivitis I Dr. Nuke Erlina Mayasari, SPMDocument23 pagesRed Eye - Conjunctivitis I Dr. Nuke Erlina Mayasari, SPMismkipendprowil2No ratings yet
- Retinal DetachmentDocument3 pagesRetinal DetachmentRownald Lakandula PanuncialNo ratings yet
- The Red EyeDocument37 pagesThe Red EyeJan Marnie ReniedoNo ratings yet
- Ophthalmology For 5th Year Exams: Visual AcuityDocument7 pagesOphthalmology For 5th Year Exams: Visual AcuitySaloni PatelNo ratings yet
- Eye Path12Document45 pagesEye Path12JillKellyNo ratings yet
- Phase 4 Ophthalmology 2021-22Document62 pagesPhase 4 Ophthalmology 2021-22Olivia Genevieve El JassarNo ratings yet
- Eyelid Disorders: Ii. ChalazionDocument62 pagesEyelid Disorders: Ii. ChalazionFreeburn SimunchembuNo ratings yet
- Corneal Ulcer Causes, Symptoms, Diagnosis and TreatmentDocument23 pagesCorneal Ulcer Causes, Symptoms, Diagnosis and TreatmentSol JoeNo ratings yet
- Ophtalmic Remedi HomeopathyDocument59 pagesOphtalmic Remedi Homeopathymihaipopescu0No ratings yet
- Homeo Treatment of Eye Diseases and AllergiesDocument17 pagesHomeo Treatment of Eye Diseases and AllergiesZia AbbasiNo ratings yet
- SENSESDocument18 pagesSENSESJimlord GarciaNo ratings yet
- The Essential Role of Eyelids in Eye HealthDocument96 pagesThe Essential Role of Eyelids in Eye HealthArwa QishtaNo ratings yet
- Eye Infection /inflammation: Presented byDocument49 pagesEye Infection /inflammation: Presented byPriya bhattiNo ratings yet
- Pharmacotherapy 10 (Oph & Oto, Derm Disorders) 1700-2000 Tue Assessment-Introduction To The Eye, Definition of Terms 15/15Document26 pagesPharmacotherapy 10 (Oph & Oto, Derm Disorders) 1700-2000 Tue Assessment-Introduction To The Eye, Definition of Terms 15/15richard bolinaoNo ratings yet
- Causes and Treatment of Red EyeDocument52 pagesCauses and Treatment of Red EyePatricia May CruzNo ratings yet
- D.D of Red EyeDocument116 pagesD.D of Red Eyehassan daacadNo ratings yet
- Bacterial ConjunctivitisDocument5 pagesBacterial ConjunctivitisBnB UsmleNo ratings yet
- Ophthalmology - Passmedicine 2012 - 62013146Document18 pagesOphthalmology - Passmedicine 2012 - 62013146abuahmed&janaNo ratings yet
- Signs and Symptoms of Macular DegenerationDocument19 pagesSigns and Symptoms of Macular DegenerationJayveersinh JadejaNo ratings yet
- Grodno State Medical University: Assistant Lecturer of The Department of OphthalmologyDocument24 pagesGrodno State Medical University: Assistant Lecturer of The Department of OphthalmologyTeguh Imana NugrahaNo ratings yet
- Ocular EmergencyDocument86 pagesOcular EmergencyMohammadNo ratings yet
- Disorder of The Eye LashesDocument9 pagesDisorder of The Eye Lasheshonovezaann.a.campita.ctucvmNo ratings yet
- BlepharitisDocument2 pagesBlepharitisPranay SriNo ratings yet
- Topic 12-Special Senses: Eyes: Name: Jewel Eve Balida Competency Appraisal Date: 10/17/16Document9 pagesTopic 12-Special Senses: Eyes: Name: Jewel Eve Balida Competency Appraisal Date: 10/17/16Lewej Eve Laurente AdilabNo ratings yet
- Current Trend in Medical Treatment of Dry Eye SyndromeDocument43 pagesCurrent Trend in Medical Treatment of Dry Eye SyndromeFaiz NazriNo ratings yet
- Mahmood J ShowailDocument47 pagesMahmood J ShowailFauzanFazaAzizNo ratings yet
- Differential Causes of Red EyeDocument4 pagesDifferential Causes of Red EyeEmily Williams100% (1)
- Geriatric OptomDocument63 pagesGeriatric OptomHarum MasyithohNo ratings yet
- Computer Vision Syndrome and Dry Eye: Causes, Symptoms, and TreatmentsDocument37 pagesComputer Vision Syndrome and Dry Eye: Causes, Symptoms, and TreatmentsIntan Winta PratiwiNo ratings yet
- Eyes DisorderDocument5 pagesEyes DisorderKathleenJoyGalAlmasinNo ratings yet
- Summary of Article: Eye Care in The Intensive Care UnitDocument6 pagesSummary of Article: Eye Care in The Intensive Care Unitparisa mohseniNo ratings yet
- James B &bron A. Lecture Notes: Ophthalmology. Ed 11. John Wiley & Sons. 2011Document9 pagesJames B &bron A. Lecture Notes: Ophthalmology. Ed 11. John Wiley & Sons. 2011qisthiNo ratings yet
- Bhavna, M Optom, FASCO. Faculty, Sankara College of Optometry, BangaloreDocument9 pagesBhavna, M Optom, FASCO. Faculty, Sankara College of Optometry, BangaloreBHUVANANo ratings yet
- Mata Merah 2Document26 pagesMata Merah 2Miftahuljnh01No ratings yet
- P 137Document8 pagesP 137Nur Rakhma AkmaliaNo ratings yet
- Dry EyeDocument72 pagesDry EyeSikha MisraNo ratings yet
- Dry Eyes, A Simple Guide To The Condition, Treatment And Related ConditionsFrom EverandDry Eyes, A Simple Guide To The Condition, Treatment And Related ConditionsNo ratings yet
- Ms - Lec8 - Cancer - NursingDocument13 pagesMs - Lec8 - Cancer - NursingDarius Crisostomo100% (1)
- Nursing Interventions for DKA and HypokalemiaDocument3 pagesNursing Interventions for DKA and HypokalemiaDarius CrisostomoNo ratings yet
- Fundamentals of NursingDocument48 pagesFundamentals of Nursinganon-429003100% (31)
- Ms - Lec2 - PainDocument15 pagesMs - Lec2 - PainDarius CrisostomoNo ratings yet
- Fundamentals of NursingDocument48 pagesFundamentals of Nursinganon-429003100% (31)
- Fundamentals of NursingDocument48 pagesFundamentals of Nursinganon-429003100% (31)
- Fundamentals of NursingDocument48 pagesFundamentals of Nursinganon-429003100% (31)
- Special Edition E-80 4Document2 pagesSpecial Edition E-80 4Ankit AgarwalNo ratings yet
- Gen 2 - Unit Test - 25.2.2022Document8 pagesGen 2 - Unit Test - 25.2.2022Phương Thảo NguyễnNo ratings yet
- Cadorna, Chesca L. - NCPDocument2 pagesCadorna, Chesca L. - NCPCadorna Chesca LoboNo ratings yet
- Acute GlomerulonephritisDocument1 pageAcute GlomerulonephritisAyrheen FornolesNo ratings yet
- Viastar Blue Oral Dissolving Film 50 MG - Sildenafil Sitrat - DKI1953300196A1 - 2019Document17 pagesViastar Blue Oral Dissolving Film 50 MG - Sildenafil Sitrat - DKI1953300196A1 - 2019RIRINo ratings yet
- Resusciation Equipments in IcuDocument29 pagesResusciation Equipments in Icuvinoli100% (1)
- International Journal of Cardiology May 2021 Issue 1Document275 pagesInternational Journal of Cardiology May 2021 Issue 1Fareesha KhanNo ratings yet
- الميكروبيولوجى والتحكم فى العدوىDocument115 pagesالميكروبيولوجى والتحكم فى العدوىmahmoud salahNo ratings yet
- Acute Common Carotid Artery Bifurcation ThrombusDocument2 pagesAcute Common Carotid Artery Bifurcation ThrombusChavdarNo ratings yet
- Exercise 3. Handling and Mass Production of Biological Control AgentsDocument5 pagesExercise 3. Handling and Mass Production of Biological Control AgentsRoxan AngonNo ratings yet
- Learning Guide 18: Animal Health Care Service NTQF Level-IVDocument105 pagesLearning Guide 18: Animal Health Care Service NTQF Level-IVRafez JoneNo ratings yet
- 1 PBDocument11 pages1 PBNaswa Alifia PutriNo ratings yet
- CariesCare-International Consensus-Manuscript BDJ-corrected 12062019Document13 pagesCariesCare-International Consensus-Manuscript BDJ-corrected 12062019pocket4love4yeahNo ratings yet
- Transportation in Animals and Plants Worksheet 7Document2 pagesTransportation in Animals and Plants Worksheet 7Parul ShahNo ratings yet
- Nauclea Latifolia: A Medicinal, Economic and Pharmacological ReviewDocument19 pagesNauclea Latifolia: A Medicinal, Economic and Pharmacological ReviewMichael Kwesi BaahNo ratings yet
- BOSH For SO1 Student Manual SampleDocument65 pagesBOSH For SO1 Student Manual SampleFroilan olazo100% (1)
- Skilled Birth Attendant (SBA) : State Institute of Health & Family Welfare JaipurDocument32 pagesSkilled Birth Attendant (SBA) : State Institute of Health & Family Welfare JaipurDurga NaikNo ratings yet
- Uts Advocacy PaperDocument11 pagesUts Advocacy PaperPlu AldiniNo ratings yet
- Guidelines For Case Classification For The National Birth Defects Prevention StudyDocument9 pagesGuidelines For Case Classification For The National Birth Defects Prevention Studyjorge davidNo ratings yet
- Nilufa Shariff - Pain Dissertation PresentationDocument31 pagesNilufa Shariff - Pain Dissertation PresentationNilufar JivrajNo ratings yet
- Review On Contact Tracing With Machine LearningDocument4 pagesReview On Contact Tracing With Machine LearningInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Statistical vs clinical significanceDocument38 pagesStatistical vs clinical significanceGeorge StoicaNo ratings yet
- Khatib2017 PDFDocument14 pagesKhatib2017 PDFluxmansrikanthaNo ratings yet
- Journal - A Bracket Positioning OverviewDocument5 pagesJournal - A Bracket Positioning OverviewRetta GabriellaNo ratings yet
- Material Safety Data Sheet - NITRIC ACID PDFDocument9 pagesMaterial Safety Data Sheet - NITRIC ACID PDFJunaid AhmadNo ratings yet
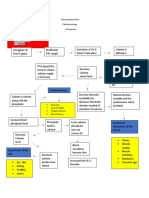
- Hypoparathyroidism PathophysiologyDocument1 pageHypoparathyroidism PathophysiologymaricarNo ratings yet
- Community Question Bank (N.a)Document41 pagesCommunity Question Bank (N.a)Sumaya AfifyNo ratings yet
- 13 AntibioticsAntiRetroviralsAIDS PDFDocument90 pages13 AntibioticsAntiRetroviralsAIDS PDFjenniferluzonNo ratings yet