You might also like
- Person-Centred Approach in Counselling and PsychotherapyDocument29 pagesPerson-Centred Approach in Counselling and PsychotherapyATHINA METAXANo ratings yet
- Revising the Person-Centered Approach: Pushing on the Envelope, but Not Very HardFrom EverandRevising the Person-Centered Approach: Pushing on the Envelope, but Not Very HardNo ratings yet
- Systems Theory in Action: Applications to Individual, Couple, and Family TherapyFrom EverandSystems Theory in Action: Applications to Individual, Couple, and Family TherapyNo ratings yet
- Systems Theory and Family Therapy: A PrimerFrom EverandSystems Theory and Family Therapy: A PrimerRating: 5 out of 5 stars5/5 (1)
- Therapy with Tough Clients: Exploring the Use of Indirect and Unconscious TechniquesFrom EverandTherapy with Tough Clients: Exploring the Use of Indirect and Unconscious TechniquesNo ratings yet
- Fanita English A Therapist's life and work: From psychoanalysis to transactional analysis and Gestalt therapyFrom EverandFanita English A Therapist's life and work: From psychoanalysis to transactional analysis and Gestalt therapyNo ratings yet
- Psycho Therapy: Therapy Practices for the Mind, Body and EmotionsFrom EverandPsycho Therapy: Therapy Practices for the Mind, Body and EmotionsNo ratings yet
- Mastering Family Therapy: Journeys of Growth and TransformationFrom EverandMastering Family Therapy: Journeys of Growth and TransformationRating: 4.5 out of 5 stars4.5/5 (2)
- Grace for the Injured Self: The Healing Approach of Heinz KohutFrom EverandGrace for the Injured Self: The Healing Approach of Heinz KohutNo ratings yet
- Counseling and Psychotherapy Theories in Context and Practice Study GuideFrom EverandCounseling and Psychotherapy Theories in Context and Practice Study GuideRating: 5 out of 5 stars5/5 (1)
- Fairbairn's Object Relations Theory in the Clinical SettingFrom EverandFairbairn's Object Relations Theory in the Clinical SettingNo ratings yet
- PSY1021 Foundation Counselling Skills Essay 1 Cover SheetDocument11 pagesPSY1021 Foundation Counselling Skills Essay 1 Cover SheetGRACE ON SPILL100% (1)
- 2007 What Every Therapist Should Know Be and DoDocument9 pages2007 What Every Therapist Should Know Be and Dodaniel segura100% (1)
- Humanistic Approaches in Counselling andDocument6 pagesHumanistic Approaches in Counselling andمالك مناصرةNo ratings yet
- Rogers Person Centred TheoryDocument18 pagesRogers Person Centred TheoryCourage Chigerwe100% (1)
- Person CentredDocument13 pagesPerson CentredRenan Antunes100% (1)
- Swaby, Helen (2020) - Learning To 'Live Upside Down' - Experiencing The True and False Self in Psychotherapy TrainingDocument15 pagesSwaby, Helen (2020) - Learning To 'Live Upside Down' - Experiencing The True and False Self in Psychotherapy TrainingPaul CNo ratings yet
- Client-Centered Therapy's Actualizing Tendency ConceptDocument13 pagesClient-Centered Therapy's Actualizing Tendency ConceptAnonymous ztqMxx75I100% (1)
- A Theory of Therapy, C. RogersDocument7 pagesA Theory of Therapy, C. RogersMarcelo Vial Roehe100% (1)
- Carl RogersDocument16 pagesCarl RogersCarlos Antonio SanchezNo ratings yet
- Role of Ethics in CounsellingDocument7 pagesRole of Ethics in CounsellingMarlyn Santos Deus Sindanum100% (2)
- Harlene Anderson: Postmodern Collaborative and Person-Centred Therapies: What Would Carl Rogers Say?Document22 pagesHarlene Anderson: Postmodern Collaborative and Person-Centred Therapies: What Would Carl Rogers Say?Alan MuñozNo ratings yet
- Personal Theory Reality TherapyDocument18 pagesPersonal Theory Reality Therapyapi-285903956100% (1)
- Person-Centred TheoryDocument18 pagesPerson-Centred TheoryJK Group LtdNo ratings yet
- Comparison and Assessment of The Three Approach Models - Sehar'sDocument10 pagesComparison and Assessment of The Three Approach Models - Sehar'sFatimeh Munawar100% (2)
- Adler University Psychotherapy Theories CourseDocument9 pagesAdler University Psychotherapy Theories CourseBrittanyWhiteNo ratings yet
- Topic 2-The Counselor As A Professional and As A PersonDocument37 pagesTopic 2-The Counselor As A Professional and As A Persondin7687No ratings yet
- Do A Client MapDocument1 pageDo A Client Mapapi-420206789No ratings yet
- Working at Relational Depth in Counselling and Psychotherapy - Dave MearnsDocument5 pagesWorking at Relational Depth in Counselling and Psychotherapy - Dave Mearnsjyjamewy33% (3)
- I'm Human Too Person-Centred Counsellors' Lived Experiences of Therapist Self-DisclosureDocument15 pagesI'm Human Too Person-Centred Counsellors' Lived Experiences of Therapist Self-DisclosureKaitheryNo ratings yet
- Cognitive Therapy by Aaron Beck and Rational Emotive Therapy by Albert Ellis-HizonDocument7 pagesCognitive Therapy by Aaron Beck and Rational Emotive Therapy by Albert Ellis-HizonDan HizonNo ratings yet
- Person-Centered Therapy and Solution-Focused Brief Therapy: An Integration of Present and Future Awareness by Lisa M. Cepeda and Donna S. DavenportDocument12 pagesPerson-Centered Therapy and Solution-Focused Brief Therapy: An Integration of Present and Future Awareness by Lisa M. Cepeda and Donna S. Davenportjacxx2100% (8)
- Person Centered TherapyDocument12 pagesPerson Centered Therapyapi-3704513100% (5)
- Carl Rogers's Client-Centered Therapy: Empathy, Unconditional Positive Regard and GenuinenessDocument8 pagesCarl Rogers's Client-Centered Therapy: Empathy, Unconditional Positive Regard and GenuinenessIqbal BaryarNo ratings yet
- Applications of Theory To Rehabilitation Counselling PracticDocument49 pagesApplications of Theory To Rehabilitation Counselling PracticShahinNo ratings yet
- Systemic-Dialogical Therapy Integrates Systemic Understanding and Dialogical PracticeDocument14 pagesSystemic-Dialogical Therapy Integrates Systemic Understanding and Dialogical PracticeFelipe SotoNo ratings yet
- DefinitionDocument5 pagesDefinitionEmma TaylorNo ratings yet
- The humanistic approach to personality and self-actualizationDocument3 pagesThe humanistic approach to personality and self-actualizationGuyton LoboNo ratings yet
- StewartDocument13 pagesStewartdewi arumNo ratings yet
- Change Process Research in PsychotherapyDocument19 pagesChange Process Research in PsychotherapyJuanaNo ratings yet
- Patterson Cognitive Behavioral Systems ApproachDocument14 pagesPatterson Cognitive Behavioral Systems ApproachSusana FossaNo ratings yet
- Person Centered TherapyDocument10 pagesPerson Centered TherapyFlavia Cardaş100% (1)
- Person-Centred Therapy GuideDocument128 pagesPerson-Centred Therapy GuideBotezat-AntonescuRaduAndrei100% (2)
- Introducing key counselling approachesDocument11 pagesIntroducing key counselling approachesLee Cheah EuNo ratings yet
- Advanced Techniques For Counseling and Psychotherapy by ConteDocument18 pagesAdvanced Techniques For Counseling and Psychotherapy by ConteDK NeriNo ratings yet
- Postmodern Ethics in Narrative TherapyDocument12 pagesPostmodern Ethics in Narrative Therapyemalinef0% (1)
- A Secure Base: Theoretical Context and OverviewDocument4 pagesA Secure Base: Theoretical Context and Overviewmadelaine_g1No ratings yet
- Mind Mapping Narrative TherapyDocument1 pageMind Mapping Narrative Therapyamni salsabilaNo ratings yet
- Humanistic ApproachDocument3 pagesHumanistic ApproachlaracanacarNo ratings yet
- Key Competencies in Psychodynamic TherapyDocument8 pagesKey Competencies in Psychodynamic TherapyfluidmindfulnessNo ratings yet
- Feminist Therapy HandoutDocument10 pagesFeminist Therapy HandoutJamie Villanueva CanauayNo ratings yet
- Comparing REBT and Person-Centered Counseling TheoriesDocument30 pagesComparing REBT and Person-Centered Counseling TheoriesIra Affandee100% (1)
- 213 What Is Existential Therapy Cooper 2Document23 pages213 What Is Existential Therapy Cooper 2bjant73No ratings yet
- Counselling Theories: Understand Construct of Theories and Its Application On PractiseDocument77 pagesCounselling Theories: Understand Construct of Theories and Its Application On PractiseYoker RonNo ratings yet
- A Person-Centered Approach To The Treatment of BPDDocument29 pagesA Person-Centered Approach To The Treatment of BPDAlbert Muya Muraya100% (1)
- Pre-Terapy A Treatment For Mental Retardation (Prouty, 2001)Document10 pagesPre-Terapy A Treatment For Mental Retardation (Prouty, 2001)luisrobles1977100% (1)
- Somatics and Revisioning PedagogyDocument25 pagesSomatics and Revisioning Pedagogyluisrobles1977No ratings yet
- Somatics Experiential Science and Transpersonal PsychologyDocument14 pagesSomatics Experiential Science and Transpersonal Psychologyluisrobles1977No ratings yet
- Allowing Painful Emotional Experiences (Greenberg, 1998)Document15 pagesAllowing Painful Emotional Experiences (Greenberg, 1998)luisrobles1977No ratings yet
- The Primacy of Experiential Practices inDocument9 pagesThe Primacy of Experiential Practices inluisrobles1977No ratings yet
- Carrying Forward Structure Bound ProcessesDocument10 pagesCarrying Forward Structure Bound Processesluisrobles1977No ratings yet
- Experiential Brief TherapyDocument18 pagesExperiential Brief Therapyluisrobles1977No ratings yet
- Anonymity and Self-Awareness in PhenomenologyDocument14 pagesAnonymity and Self-Awareness in Phenomenologyluisrobles1977No ratings yet
- The Person Centered Approach From An ExiDocument9 pagesThe Person Centered Approach From An Exiluisrobles1977No ratings yet
- Inicial Stage of Therapy in MPDDocument17 pagesInicial Stage of Therapy in MPDluisrobles1977No ratings yet
- New Ways of Processing Experience - Structure-Bound ProcessesDocument20 pagesNew Ways of Processing Experience - Structure-Bound Processesluisrobles1977No ratings yet
- Incorporating Psychotherapeutic Methods - Bridle - Psychosis MayDocument13 pagesIncorporating Psychotherapeutic Methods - Bridle - Psychosis Mayluisrobles1977No ratings yet
- Lysaker Hermans Schizophrenia2007Document12 pagesLysaker Hermans Schizophrenia2007luisrobles1977No ratings yet
- Leslie A Ellis - Body DreamWork - Using Focusing To Find The Life Force Inherent in DreamsDocument11 pagesLeslie A Ellis - Body DreamWork - Using Focusing To Find The Life Force Inherent in Dreamsluisrobles1977No ratings yet
- Internal Sel Helpers in MPDDocument6 pagesInternal Sel Helpers in MPDluisrobles1977No ratings yet
- The Changes Book: A Handbook for Bringing People TogetherDocument194 pagesThe Changes Book: A Handbook for Bringing People Togetherluisrobles1977100% (1)
- Inner Self HelperDocument13 pagesInner Self Helperluisrobles1977No ratings yet
- Dissociation and Schizophrenia - DisociationDocument11 pagesDissociation and Schizophrenia - Disociationluisrobles1977No ratings yet
- Iatrogenis of MisdiagnosisDocument7 pagesIatrogenis of Misdiagnosisluisrobles1977No ratings yet
- Iatrogenesis and DissociationDocument3 pagesIatrogenesis and Dissociationluisrobles1977No ratings yet
- Iatrogenic Creation of New AltersDocument9 pagesIatrogenic Creation of New Altersluisrobles1977No ratings yet
- Iatrogenic Perpetuation of SplittingDocument7 pagesIatrogenic Perpetuation of Splittingluisrobles1977No ratings yet
- Effects of Exorcism in MPDDocument17 pagesEffects of Exorcism in MPDluisrobles1977No ratings yet
- Extrenely Complex MPD - DisociationDocument12 pagesExtrenely Complex MPD - Disociationluisrobles1977No ratings yet
- Dream Character as a Prototype for Dissociative Identity Disorder AltersDocument8 pagesDream Character as a Prototype for Dissociative Identity Disorder Altersluisrobles1977No ratings yet
- DID in Play Therapy - DisociationDocument4 pagesDID in Play Therapy - Disociationluisrobles1977No ratings yet
- Error in Treatment of MPD - DisociationDocument6 pagesError in Treatment of MPD - Disociationluisrobles1977No ratings yet
- DID in Children and Adolescents - DisociationDocument9 pagesDID in Children and Adolescents - Disociationluisrobles1977No ratings yet
- Completed Suicides en DID - DisociationDocument8 pagesCompleted Suicides en DID - Disociationluisrobles1977No ratings yet
- Cover and Subtle Forms of MPD - DisociationDocument7 pagesCover and Subtle Forms of MPD - Disociationluisrobles1977No ratings yet
- Adult Assessment: Head To Toe Assessment Is The Baseline and Ongoing Data That Is Needed OnDocument2 pagesAdult Assessment: Head To Toe Assessment Is The Baseline and Ongoing Data That Is Needed OnAldrin NavarroNo ratings yet
- English Form 2 Mod23042022001Document10 pagesEnglish Form 2 Mod23042022001Qiash JontezNo ratings yet
- Physical Properties of Groups 1, 17 and 18 ElementsDocument5 pagesPhysical Properties of Groups 1, 17 and 18 ElementslenovosubaNo ratings yet
- Plasma MachiningDocument14 pagesPlasma MachiningMayankNo ratings yet
- Soalan Pecutan Akhir Fizik SPM 2010 Kertas 2 Set 3 PDFDocument18 pagesSoalan Pecutan Akhir Fizik SPM 2010 Kertas 2 Set 3 PDFAnna Latifah CammryNo ratings yet
- Medical Certificate: (Coaches, Assistant Coaches, Chaperone)Document1 pageMedical Certificate: (Coaches, Assistant Coaches, Chaperone)Keith Marinas Serquina100% (1)
- EWM Certification Syllabus (9.5) Topic Areas Topic Details, Courses, Books WeightingDocument2 pagesEWM Certification Syllabus (9.5) Topic Areas Topic Details, Courses, Books Weightingguru_3112No ratings yet
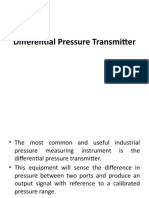
- Differential Pressure TransmitterDocument14 pagesDifferential Pressure TransmitterZainab KadhemNo ratings yet
- Physical ExaminationDocument7 pagesPhysical ExaminationCha CulveraNo ratings yet
- Pds - Sunshades Instrument CoverDocument2 pagesPds - Sunshades Instrument CoverAntonio LantiguaNo ratings yet
- F 856 - 97 - Rjg1ni05nw - PDFDocument7 pagesF 856 - 97 - Rjg1ni05nw - PDFRománBarciaVazquezNo ratings yet
- 2) VT Report Test FormatDocument3 pages2) VT Report Test FormatMoin KhanNo ratings yet
- University of Groningen MagazineDocument14 pagesUniversity of Groningen MagazineKhanh Phuong PhamNo ratings yet
- Marketing Environment Analysis and Trends Impacting CompaniesDocument27 pagesMarketing Environment Analysis and Trends Impacting CompaniesSamoyed KalraNo ratings yet
- Product RD Session 16 - Phase Eqm Part 3Document38 pagesProduct RD Session 16 - Phase Eqm Part 3Rishabh JainNo ratings yet
- Microwave TubesDocument36 pagesMicrowave TubesHINDUSTAN KNOW 1No ratings yet
- Grundfosliterature 743129Document7 pagesGrundfosliterature 743129Ted Andrew AbalosNo ratings yet
- Install Panel WallDocument10 pagesInstall Panel WallLuis PalaciosNo ratings yet
- Experiment # 04: Short-Circuit Test of Single Phase TransformerDocument5 pagesExperiment # 04: Short-Circuit Test of Single Phase TransformerNasir Ali / Lab Engineer, Electrical Engineering DepartmentNo ratings yet
- A Review of Empathy Education in NursingDocument11 pagesA Review of Empathy Education in Nursinglora ardyaNo ratings yet
- Exercise 5 - Journalizing TransactionsDocument10 pagesExercise 5 - Journalizing TransactionsMichael DiputadoNo ratings yet
- How to Compost at Home: A Guide to the BasicsDocument10 pagesHow to Compost at Home: A Guide to the BasicsYeo Choon SengNo ratings yet
- Working at Height PolicyDocument7 pagesWorking at Height PolicyAniekan AkpaidiokNo ratings yet
- 7Document40 pages7Felipe RichardiosNo ratings yet
- Midterm MMMDocument2 pagesMidterm MMMasdfghjkl zxcvbnmNo ratings yet
- Chapter 6Document2 pagesChapter 6Zhane CruzNo ratings yet
- District Potential Analysis of PilibhitDocument57 pagesDistrict Potential Analysis of PilibhitJasraj SinghNo ratings yet
- Buller, Paul F. - Schuler, Randall S - Managing Organizations and People - Cases in Management, Organizational Behavior and Human Resource Management-Thomson - South-Western (2006)Document530 pagesBuller, Paul F. - Schuler, Randall S - Managing Organizations and People - Cases in Management, Organizational Behavior and Human Resource Management-Thomson - South-Western (2006)ezekiel capuzNo ratings yet
- Water Purification Hardness Estimation EDTA Ion ExchangeDocument19 pagesWater Purification Hardness Estimation EDTA Ion ExchangesiddharthNo ratings yet
- AA3 My Favorite City - Comparing Places Ejercicio FinalDocument6 pagesAA3 My Favorite City - Comparing Places Ejercicio FinalCesar Augusto Triana AyalaNo ratings yet