You might also like
- Bikini Body Burn PDFDocument120 pagesBikini Body Burn PDFGratiana Timis100% (1)
- Phytochemicals of Cranberries and Cranberry Products Characterization, Potential Health Effects, and Processing StabilityDocument42 pagesPhytochemicals of Cranberries and Cranberry Products Characterization, Potential Health Effects, and Processing StabilityNasir AhmedNo ratings yet
- Bio 024 Lab Activity 9 General Characteristics of ChoDocument11 pagesBio 024 Lab Activity 9 General Characteristics of ChoMikka Kaye Calado100% (1)
- TMP A952Document6 pagesTMP A952FrontiersNo ratings yet
- Compuestos BioactivosDocument4 pagesCompuestos BioactivosJessy HowardNo ratings yet
- Nutraceuticals & Nutrigenomics: Subject Code: FN - 504Document14 pagesNutraceuticals & Nutrigenomics: Subject Code: FN - 504Saadman RahmanNo ratings yet
- CHORIBar HistoryDocument9 pagesCHORIBar HistoryK Mehmet ŞensoyNo ratings yet
- Health Benefits of Fruit and Vegetables Are From Additive and Synergistic Combinations of PhytochemicalsDocument4 pagesHealth Benefits of Fruit and Vegetables Are From Additive and Synergistic Combinations of PhytochemicalsRiley RilanNo ratings yet
- PhytochemicalsDocument4 pagesPhytochemicalsbragaru.vladNo ratings yet
- Defining A Healthy Diet - Evidence For The Role of Contemporary Dietary Patterns in Health and DiseaseDocument15 pagesDefining A Healthy Diet - Evidence For The Role of Contemporary Dietary Patterns in Health and DiseaseARESS RIPNo ratings yet
- Arabinoxylans and Human HealthDocument5 pagesArabinoxylans and Human HealthNasir AhmedNo ratings yet
- Health-Promoting Components of Fruits and Vegetables in The DietDocument9 pagesHealth-Promoting Components of Fruits and Vegetables in The DietGarv JainNo ratings yet
- Medicina: Nutritional Status and The Influence of The Vegan Diet On The Gut Microbiota and Human HealthDocument15 pagesMedicina: Nutritional Status and The Influence of The Vegan Diet On The Gut Microbiota and Human HealthCem Tunaboylu (Student)No ratings yet
- 1789S FullDocument5 pages1789S Fullgemma mutiaraNo ratings yet
- Leitzmann - Vegetarian Diets - What Are The AdvantagesDocument11 pagesLeitzmann - Vegetarian Diets - What Are The Advantageswbechara103No ratings yet
- Ijms 21 01250Document40 pagesIjms 21 01250silviNo ratings yet
- Chiou 2014Document23 pagesChiou 2014BRUNO JOSE BRITO TEIXEIRANo ratings yet
- Desordenes Gastrointestinales PDFDocument7 pagesDesordenes Gastrointestinales PDFMvz Mary Cielo Fernández FuentesNo ratings yet
- J Sci Food Agric - 2000 - Dillard - Phytochemicals Nutraceuticals and Human HealthDocument13 pagesJ Sci Food Agric - 2000 - Dillard - Phytochemicals Nutraceuticals and Human Healthyaseena6No ratings yet
- Using Probioticos in Gastrointestinal DisordersDocument7 pagesUsing Probioticos in Gastrointestinal DisordersRonald CampoverdeNo ratings yet
- Introduction and Basic Principles: Dr. K. S. Abbasi Department of Food Tech/Human NutritionDocument8 pagesIntroduction and Basic Principles: Dr. K. S. Abbasi Department of Food Tech/Human Nutritionnouman ashrafNo ratings yet
- Jurnal 9Document10 pagesJurnal 9Fryza SatriaNo ratings yet
- 25909-Article Text-86090-1-18-20240313Document13 pages25909-Article Text-86090-1-18-20240313aliciajeumpaNo ratings yet
- Cancer & Inflammation Herbal RemediesDocument22 pagesCancer & Inflammation Herbal RemediesAlice LeeNo ratings yet
- Efecto de Los Compuestos Bioactivos en La EpigenéticaDocument21 pagesEfecto de Los Compuestos Bioactivos en La EpigenéticaSteFy Reyes GilNo ratings yet
- Replenishing The Nutrients Depleted by Drugs Holistic PharmacistDocument3 pagesReplenishing The Nutrients Depleted by Drugs Holistic PharmacistnepretipNo ratings yet
- Gut Microbiota and Human HealthDocument3 pagesGut Microbiota and Human HealthJamie HaravataNo ratings yet
- 4d53 Diagnosis and Treatment of Nutritional Deficiencies and DiseasesDocument33 pages4d53 Diagnosis and Treatment of Nutritional Deficiencies and DiseasesLorenjoy BarridaNo ratings yet
- The Molecular Biology of How Dietary Supplements Support Optimal Human HealthDocument15 pagesThe Molecular Biology of How Dietary Supplements Support Optimal Human HealthKarlos Lds NvNo ratings yet
- Supportive 4GDocument2 pagesSupportive 4Goffice8187No ratings yet
- Functional Foods and Their Impact On HealthDocument15 pagesFunctional Foods and Their Impact On HealthAndrés ZapataNo ratings yet
- Ayushi Verma Practice SchoolDocument20 pagesAyushi Verma Practice SchoolAkash YadavNo ratings yet
- Nutraceuticals A ReviewDocument0 pagesNutraceuticals A ReviewharborNo ratings yet
- Pure Introduction Prof. 1Document14 pagesPure Introduction Prof. 1Qüàñtîùm Stâmîñà Jr.No ratings yet
- Molecules 20 19753Document19 pagesMolecules 20 19753Dreyden HaloNo ratings yet
- Nutition Effects On CancerDocument7 pagesNutition Effects On CancercmdcscribdNo ratings yet
- Amidiq: Applications of Soluble Dietary Fibers in Beverages Aplicaciones de La Fibra Dietetica Soluble en BebidasDocument15 pagesAmidiq: Applications of Soluble Dietary Fibers in Beverages Aplicaciones de La Fibra Dietetica Soluble en BebidasYukiKudoNo ratings yet
- Ecam2021 9995903Document19 pagesEcam2021 9995903Alfiah fira SyukriNo ratings yet
- Writingassignment 1Document4 pagesWritingassignment 1api-534320285No ratings yet
- Food Is Medicine PDFDocument18 pagesFood Is Medicine PDFDinesh SharmaNo ratings yet
- Gillies 2003Document6 pagesGillies 2003puspitaNo ratings yet
- Functional Foods and Nutracetical 2012-LibreDocument18 pagesFunctional Foods and Nutracetical 2012-LibreLeila MoghadasNo ratings yet
- Fermented Foods and Beverages in Human Diet and Their Influence On Gut Microbiota and HealthDocument13 pagesFermented Foods and Beverages in Human Diet and Their Influence On Gut Microbiota and HealthDamar MurtiNo ratings yet
- Functional Foods and Their Role in Cancer Prevention and Health PromotionDocument30 pagesFunctional Foods and Their Role in Cancer Prevention and Health PromotionSílfide XanatNo ratings yet
- Diet-Microbe Interactions in the Gut: Effects on Human Health and DiseaseFrom EverandDiet-Microbe Interactions in the Gut: Effects on Human Health and DiseaseKieran TuohyRating: 4.5 out of 5 stars4.5/5 (2)
- Antioxidants 12 00362 v2Document4 pagesAntioxidants 12 00362 v2Paskah DianNo ratings yet
- Scalbert Johnson Saltmarsh, 2005Document3 pagesScalbert Johnson Saltmarsh, 2005Jardel SchoffelNo ratings yet
- Functional Foods: The US Perspective: John A MilnerDocument6 pagesFunctional Foods: The US Perspective: John A MilnerAzizah MunitaNo ratings yet
- Nutrigenomics and Nutrigenetics: New Insight in Disease Prevention and CureDocument3 pagesNutrigenomics and Nutrigenetics: New Insight in Disease Prevention and CureTesa RafkhaniNo ratings yet
- 3 1 47 813 PDFDocument4 pages3 1 47 813 PDFMinh DuyNo ratings yet
- Special Article: Food, Not Nutrients, Is The Fundamental Unit in NutritionDocument12 pagesSpecial Article: Food, Not Nutrients, Is The Fundamental Unit in NutritionIvo Veloso VegaNo ratings yet
- International Research Conference On Food, Nutrition, and CancerDocument7 pagesInternational Research Conference On Food, Nutrition, and CancersahirbuleNo ratings yet
- Assignment No. 4: NutrigenomicsDocument7 pagesAssignment No. 4: NutrigenomicshajraNo ratings yet
- Food and Nutrition Biotechnology: UNU-IAS ReportDocument36 pagesFood and Nutrition Biotechnology: UNU-IAS Reportthanh_hai2014No ratings yet
- Nutrients 12 03209Document17 pagesNutrients 12 03209Rabhita AuliaNo ratings yet
- Nutritional GenomicsDocument4 pagesNutritional GenomicsSANDHEEP SNo ratings yet
- ARICULO4Document9 pagesARICULO4Adriana SalamancaNo ratings yet
- Antioxidant Relevance To Human Health: Mini ReviewDocument6 pagesAntioxidant Relevance To Human Health: Mini ReviewCecilia NunezNo ratings yet
- Materi Serat Air 3Document5 pagesMateri Serat Air 3ranaNo ratings yet
- Reader's Digest Plant Based Health BasicsFrom EverandReader's Digest Plant Based Health BasicsReader's DigestNo ratings yet
- Older Adults and Patients in Need of Nutritional Support Review of CurrentDocument10 pagesOlder Adults and Patients in Need of Nutritional Support Review of CurrentimwinnerNo ratings yet
- Pain - National Cancer InstituteDocument91 pagesPain - National Cancer InstituteCarlos ArbeláezNo ratings yet
- Adjuvant Analgesics: Helena Knotkova, PHD, Marco Pappagallo, MDDocument12 pagesAdjuvant Analgesics: Helena Knotkova, PHD, Marco Pappagallo, MDCarlos ArbeláezNo ratings yet
- Short-Term Neurodevelopmental Outcome in Term Neonates PDFDocument8 pagesShort-Term Neurodevelopmental Outcome in Term Neonates PDFCarlos ArbeláezNo ratings yet
- Levetiracetam Versus Phenobarbital For Neonatal SeizuresDocument14 pagesLevetiracetam Versus Phenobarbital For Neonatal SeizuresCarlos ArbeláezNo ratings yet
- International Classification of Functioning, Disability and Health (ICF) Core Set For Patients With Vertigo, Dizziness and Balance DisordersDocument11 pagesInternational Classification of Functioning, Disability and Health (ICF) Core Set For Patients With Vertigo, Dizziness and Balance DisordersCarlos ArbeláezNo ratings yet
- The Ketogenic Diet: A Detailed Beginner's GuideDocument20 pagesThe Ketogenic Diet: A Detailed Beginner's GuideSarthak Mishra100% (1)
- Biology Lab ReportDocument5 pagesBiology Lab Reportapi-2576094460% (1)
- 100ml Sugar Cane JusDocument5 pages100ml Sugar Cane JusHasna RofikawatiNo ratings yet
- Analysis of Fruit JuiceDocument14 pagesAnalysis of Fruit JuiceRAHUL ROY100% (1)
- Chemical Analysis of FoodDocument12 pagesChemical Analysis of Foodprince1900100% (1)
- Queso Con VegetalesDocument9 pagesQueso Con VegetalesJhon Fernando NiñoNo ratings yet
- Digestion of Starch in HumansDocument7 pagesDigestion of Starch in HumansMOHD MU'IZZ BIN MOHD SHUKRINo ratings yet
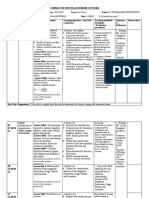
- Format of Unit Plan/Scheme of Work: A Learner Can Explain 1. Biology 8th Ed by Campbell and ReeceDocument19 pagesFormat of Unit Plan/Scheme of Work: A Learner Can Explain 1. Biology 8th Ed by Campbell and ReeceMutaganda Ami fideleNo ratings yet
- Gene SNP Sample ReportDocument29 pagesGene SNP Sample ReportBedington TherapeuticsNo ratings yet
- Marc Fitt Diete 3069 CaloriesDocument2 pagesMarc Fitt Diete 3069 Caloriesdonnix30No ratings yet
- Eating With Ostomy 2022Document76 pagesEating With Ostomy 2022PCMC Dietitians NDDNo ratings yet
- 3BSM Group 3 General Tests For CarbohydratesDocument42 pages3BSM Group 3 General Tests For CarbohydratesJeanette RiosNo ratings yet
- Pharmacotherapy Casa Patient Focused Approach 10Th Edition Full ChapterDocument41 pagesPharmacotherapy Casa Patient Focused Approach 10Th Edition Full Chaptermuriel.moreno949100% (29)
- Practical Manual ON Renewable Energy and Green TechnologyDocument48 pagesPractical Manual ON Renewable Energy and Green Technologyrejeesh_rajendranNo ratings yet
- The Apex Predator DietDocument73 pagesThe Apex Predator Dietdeclanku100% (2)
- Midterm Exam PHYED101 44-50 88%Document27 pagesMidterm Exam PHYED101 44-50 88%Jade Lagrana II67% (6)
- Food CaloriesDocument9 pagesFood Caloriesdohimbang4769No ratings yet
- MYS 2010 Guide To Nutrition Labelling and Claims PDFDocument44 pagesMYS 2010 Guide To Nutrition Labelling and Claims PDFMalikah Meny HartatyNo ratings yet
- Self-Defence Against Cancer - 10 Counter-Moves You Can UseDocument84 pagesSelf-Defence Against Cancer - 10 Counter-Moves You Can Usemukund gurujiNo ratings yet
- This Study Resource Was: Organic Chemistry I CHM3201Document8 pagesThis Study Resource Was: Organic Chemistry I CHM3201Wan Nur AtikahNo ratings yet
- Buckwheat. Fagopyrum Esculentum MoenchDocument95 pagesBuckwheat. Fagopyrum Esculentum MoenchJános Lazányi100% (4)
- Food: Where Does It Come From ?: Worksheet-1Document77 pagesFood: Where Does It Come From ?: Worksheet-1sanaNo ratings yet
- Fatigue Fighting TipsDocument3 pagesFatigue Fighting TipsYuni BongNo ratings yet
- Indian Food Carb CountingDocument84 pagesIndian Food Carb Countingpoptot000No ratings yet
- 28-12-19 SR - Icon All Gtm-5 Code-A Key & Sol'sDocument27 pages28-12-19 SR - Icon All Gtm-5 Code-A Key & Sol'smahesh tNo ratings yet
- 22Document2 pages22Dipayan DasNo ratings yet
- Nutritive Value of Indian FoodsDocument219 pagesNutritive Value of Indian FoodsReshmi Haflongbar94% (16)
- Dwnload Full Biology Concepts and Investigations 3rd Edition Hoefnagels Solutions Manual PDFDocument36 pagesDwnload Full Biology Concepts and Investigations 3rd Edition Hoefnagels Solutions Manual PDFjunemojarrazqmxj100% (17)