You might also like
- Supportive Care in Pediatric Oncology: A Practical Evidence-Based ApproachFrom EverandSupportive Care in Pediatric Oncology: A Practical Evidence-Based ApproachJames H. FeusnerNo ratings yet
- Cancer Health Effects of Pesticides - The College of Family Physicians of CanadaDocument11 pagesCancer Health Effects of Pesticides - The College of Family Physicians of CanadaKashaf ButtNo ratings yet
- SR and Guidelines For Periop MGMT of Peds Patients Undergoing Major Plastic SurgeryDocument10 pagesSR and Guidelines For Periop MGMT of Peds Patients Undergoing Major Plastic SurgeryPaul MarjiNo ratings yet
- Recognition and Management of Sepsis in Children: Practice Patterns in The Emergency DepartmentDocument9 pagesRecognition and Management of Sepsis in Children: Practice Patterns in The Emergency DepartmentRahadian MalikNo ratings yet
- Haspel 2014Document7 pagesHaspel 2014FOURAT OUERGHEMMINo ratings yet
- Educationandadministration: Development of A Validated Exam To Assess Physician Transfusion Medicine KnowledgeDocument6 pagesEducationandadministration: Development of A Validated Exam To Assess Physician Transfusion Medicine KnowledgeFOURAT OUERGHEMMI100% (1)
- Severity Scoring Systems: Are They Internally Valid, Reliable and Predictive of Oxygen Use in Children With Acute Bronchiolitis?Document7 pagesSeverity Scoring Systems: Are They Internally Valid, Reliable and Predictive of Oxygen Use in Children With Acute Bronchiolitis?Ivan VeriswanNo ratings yet
- Karumbi Et Al 2013Document6 pagesKarumbi Et Al 2013sundaimeNo ratings yet
- Oral Antibiotics For Neonatal Infections: A Systematic Review and Meta-AnalysisDocument12 pagesOral Antibiotics For Neonatal Infections: A Systematic Review and Meta-AnalysisAzaliRiccoNo ratings yet
- Eria 3Document15 pagesEria 3ruth angelinaNo ratings yet
- Survey of Critical Value ReportingDocument6 pagesSurvey of Critical Value ReportingccumplidouNo ratings yet
- Development and Validation of College Students ' Tuberculosis Knowledge, Attitudes and Practices Questionnaire (CS-TBKAPQ)Document11 pagesDevelopment and Validation of College Students ' Tuberculosis Knowledge, Attitudes and Practices Questionnaire (CS-TBKAPQ)Vertavera SyaulatiaNo ratings yet
- Assessment of Self Management in Patients With DiaDocument9 pagesAssessment of Self Management in Patients With DiaPaula Francisca Moraga HidalgoNo ratings yet
- Tight Glycemic Control in Critically Ill PediatricDocument11 pagesTight Glycemic Control in Critically Ill Pediatricbella friscaamaliaNo ratings yet
- 1 s2.0 S2666577822001009 Main - 2Document10 pages1 s2.0 S2666577822001009 Main - 2Shandy Suwanto PutraNo ratings yet
- Comparison of Amoxicillin/Clavulanic Acid High Dose With Cef Dinir in The Treatment of Acute Otitis MediaDocument8 pagesComparison of Amoxicillin/Clavulanic Acid High Dose With Cef Dinir in The Treatment of Acute Otitis Mediaenggainget8663No ratings yet
- Nifas AnemiaDocument10 pagesNifas AnemiaFahmi SaputraNo ratings yet
- Review Mcad PkuDocument21 pagesReview Mcad PkuKamal JaoniNo ratings yet
- A Trial of An Anamnesis Based Score Applied As A.95804Document8 pagesA Trial of An Anamnesis Based Score Applied As A.95804ANA BEATRIZ MUNOZ URRIBARRINo ratings yet
- Precision Medicine in Pediatric Oncology: ReviewDocument8 pagesPrecision Medicine in Pediatric Oncology: ReviewCiocan AlexandraNo ratings yet
- Code Blue EmergenciesDocument17 pagesCode Blue EmergenciesEstherThompsonNo ratings yet
- 2017 La Iniciativa de Laboratorio Canadiense Sobre Intervalos de Referencia Pediátricos. Un Documento Técnico de CALIPERDocument57 pages2017 La Iniciativa de Laboratorio Canadiense Sobre Intervalos de Referencia Pediátricos. Un Documento Técnico de CALIPERpintopablo108bNo ratings yet
- Bookshelf NBK315902Document18 pagesBookshelf NBK315902Lucas WillianNo ratings yet
- Erdal-2017-The Economic Impact of Poor SampleDocument10 pagesErdal-2017-The Economic Impact of Poor SampleGökhanNo ratings yet
- Inappropriateness in Laboratory Medicine An Elephant in The RoomDocument4 pagesInappropriateness in Laboratory Medicine An Elephant in The RoomomaromranNo ratings yet
- Critical Value ReportingDocument7 pagesCritical Value Reportingjorguey100% (1)
- Bacterial Vaginosis Draft Evidence ReviewDocument206 pagesBacterial Vaginosis Draft Evidence Reviewaisa mutiaraNo ratings yet
- Art:10.1186/s13063 016 1365 6Document10 pagesArt:10.1186/s13063 016 1365 6fandyNo ratings yet
- Clinical Pathway, LosDocument3 pagesClinical Pathway, LosImuzz Al GhassanNo ratings yet
- A Consensus Report On Appropriate Treatment Optimization and Transitioning in The Management of Moderate-To-Severe Plaque PsoriasisDocument16 pagesA Consensus Report On Appropriate Treatment Optimization and Transitioning in The Management of Moderate-To-Severe Plaque PsoriasispancholarpancholarNo ratings yet
- Impact of ASP in IcuDocument8 pagesImpact of ASP in Icuguilherme_ribeirNo ratings yet
- Summ 1619Document8 pagesSumm 1619novialbarNo ratings yet
- Tailieuxanh cc3803 0597Document8 pagesTailieuxanh cc3803 0597Cu ChíNo ratings yet
- Hospital Outcomes For Paediatric Pneumonia and Diarrhoea Patients Admitted in A Tertiary Hospital On Weekdays Versus Weekends: A Retrospective StudyDocument9 pagesHospital Outcomes For Paediatric Pneumonia and Diarrhoea Patients Admitted in A Tertiary Hospital On Weekdays Versus Weekends: A Retrospective StudyZidni Arifa LuthfiNo ratings yet
- Anemia in Pregnancy in Malaysia: A Cross-Sectional Survey: Original ArticleDocument10 pagesAnemia in Pregnancy in Malaysia: A Cross-Sectional Survey: Original ArticleThomson AffendyNo ratings yet
- CUA MultivitDocument7 pagesCUA MultivitSarah AlmiraNo ratings yet
- Critical Value in HematologyDocument8 pagesCritical Value in HematologySTARK DIAGNOSTICSNo ratings yet
- Knowledge, Attitudes and Practice Survey About Antimicrobial Resistance and Prescribing Among Physicians in A Hospital Setting in Lima, PeruDocument8 pagesKnowledge, Attitudes and Practice Survey About Antimicrobial Resistance and Prescribing Among Physicians in A Hospital Setting in Lima, PeruShiuMan LimNo ratings yet
- HQ Vol12 PSP Coffey-2Document8 pagesHQ Vol12 PSP Coffey-2CadR 1No ratings yet
- Septic Shock Carcillo PDFDocument14 pagesSeptic Shock Carcillo PDFjesus_berber_2No ratings yet
- Cancer Health Effects of PesticidesDocument8 pagesCancer Health Effects of PesticidesnafpaktosNo ratings yet
- Ijlh 12526Document15 pagesIjlh 12526my accountNo ratings yet
- Stress Ulcer, Gastritis, and Gastrointestinal Bleeding Prophylaxis in Critically Ill Pediatric Patients: A Systematic ReviewDocument9 pagesStress Ulcer, Gastritis, and Gastrointestinal Bleeding Prophylaxis in Critically Ill Pediatric Patients: A Systematic ReviewIkrima MuhdarmuhallyNo ratings yet
- CirPed Diferença JPS 2014Document6 pagesCirPed Diferença JPS 2014Valmir MouraNo ratings yet
- Mesalamine Dosing Tor Ulcerative Colitis Remission MaintenanceDocument11 pagesMesalamine Dosing Tor Ulcerative Colitis Remission MaintenanceIasa FebrianusNo ratings yet
- Advances in Pediatric Reference Intervals For Biochemical Markers: Establishment of The Caliper Database in Healthy Children and AdolescentsDocument9 pagesAdvances in Pediatric Reference Intervals For Biochemical Markers: Establishment of The Caliper Database in Healthy Children and AdolescentsSid TyagiNo ratings yet
- The Path To Perfect Pediatric Posology - Drug Development in PediatricsDocument10 pagesThe Path To Perfect Pediatric Posology - Drug Development in PediatricsMaki-Chan マキNo ratings yet
- Acumulacion de Liquidos PulmonDocument4 pagesAcumulacion de Liquidos PulmonWando LunNo ratings yet
- What Are The Patterns of Compliance Whith Early Warning TrackDocument9 pagesWhat Are The Patterns of Compliance Whith Early Warning TrackPAULA SORAIA CHENNo ratings yet
- The Quality of Ambulatory Care Delivered To Children in The United StatesDocument9 pagesThe Quality of Ambulatory Care Delivered To Children in The United Statesnovia khairulbariaNo ratings yet
- Peds 2011-1330 FullDocument18 pagesPeds 2011-1330 FullbealacambraNo ratings yet
- Management of The Undescended Testis in ChildrenDocument16 pagesManagement of The Undescended Testis in ChildrenRashmeeta ThadhaniNo ratings yet
- Urine Specimen Collection - How A Multidisciplinary Team Improved Patient Outcomes Using Best Practices - ProQuestDocument9 pagesUrine Specimen Collection - How A Multidisciplinary Team Improved Patient Outcomes Using Best Practices - ProQuestHelmy HanafiNo ratings yet
- Brief Care Giver ProtocolDocument2 pagesBrief Care Giver ProtocolKhalid SoomroNo ratings yet
- Clinical Practice Guideline Safe Medication Use.32Document39 pagesClinical Practice Guideline Safe Medication Use.32Edward ZiyachechaNo ratings yet
- Srep08219 PDFDocument8 pagesSrep08219 PDFLinda JajauuooNo ratings yet
- Acm 2010 0572 PDFDocument6 pagesAcm 2010 0572 PDFRiley RilanNo ratings yet
- Acm 2010 0572 PDFDocument6 pagesAcm 2010 0572 PDFRiley RilanNo ratings yet
- AmbulasiDocument12 pagesAmbulasiRafii KhairuddinNo ratings yet
- IACC - Levey - Jennings - & - Westgard - Rules - DR - Fauqa, - SP - PKDocument53 pagesIACC - Levey - Jennings - & - Westgard - Rules - DR - Fauqa, - SP - PKAmanda Sonia ArliestaNo ratings yet
- Molecular Template MfrsDocument41 pagesMolecular Template Mfrsiq_dianaNo ratings yet
- MR Solomon Training Antigen SomaliaDocument10 pagesMR Solomon Training Antigen Somaliaiq_dianaNo ratings yet
- Ms Rebecca General Communication SkillDocument44 pagesMs Rebecca General Communication Skilliq_dianaNo ratings yet
- Ten Scientific Reasons in Support of Airborne Transmission of Sars-Cov-2Document3 pagesTen Scientific Reasons in Support of Airborne Transmission of Sars-Cov-2tuanda222No ratings yet
- DR Gabriel Wallau Genomic Data Sharing Covid19 BrazilDocument18 pagesDR Gabriel Wallau Genomic Data Sharing Covid19 Braziliq_dianaNo ratings yet
- ICSH Recommendations For The Standardization of Peripheral Blood Cell Morphological Features PDFDocument17 pagesICSH Recommendations For The Standardization of Peripheral Blood Cell Morphological Features PDFSaraswati Wulandari HartonoNo ratings yet
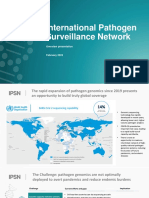
- DR Oliver Morgan International Pathogen Surveillance NetoworkDocument16 pagesDR Oliver Morgan International Pathogen Surveillance Netoworkiq_dianaNo ratings yet
- MR Tapiwanashe Training Nasal Antigen ZimbabweDocument25 pagesMR Tapiwanashe Training Nasal Antigen Zimbabweiq_dianaNo ratings yet
- Klarkowski 2013Document14 pagesKlarkowski 2013iq_dianaNo ratings yet
- Jamainternal Lee 2020 Oi 200057 1603479600.04745Document6 pagesJamainternal Lee 2020 Oi 200057 1603479600.04745Fina RepitiyanaNo ratings yet
- COVID-19 Testing One Size Does Not Fit AllDocument3 pagesCOVID-19 Testing One Size Does Not Fit Alliq_dianaNo ratings yet
- COVID19Document2 pagesCOVID19Tony Cogliano Allechi SpencerNo ratings yet
- 10 1001@jama 2020 8259 PDFDocument3 pages10 1001@jama 2020 8259 PDFTriLightNo ratings yet
- Crossm: Laboratory Diagnosis of COVID-19: Current Issues and ChallengesDocument9 pagesCrossm: Laboratory Diagnosis of COVID-19: Current Issues and ChallengesbelaariyantiNo ratings yet
- King 1994Document6 pagesKing 1994iq_dianaNo ratings yet
- EUA Seegene Allplex Ifu - 2Document85 pagesEUA Seegene Allplex Ifu - 2iq_dianaNo ratings yet
- DR Sanjay FIND Covid TestingDocument9 pagesDR Sanjay FIND Covid Testingiq_dianaNo ratings yet
- Dr. Ni Made Hustrini, SPPD-KGH - CKD Sysmex - 280522Document33 pagesDr. Ni Made Hustrini, SPPD-KGH - CKD Sysmex - 280522iq_dianaNo ratings yet
- 20 01 25 Anita SANDS - Omicron Risk Assessment - DR AnitaDocument9 pages20 01 25 Anita SANDS - Omicron Risk Assessment - DR Anitaiq_dianaNo ratings yet
- COVID19 Specimen Acceptability - LDT Roche Revised Version v4 32020Document11 pagesCOVID19 Specimen Acceptability - LDT Roche Revised Version v4 32020iq_dianaNo ratings yet
- DR Lara Vojnov Severe Acute Hepatitis of Unknown Aetiology WHO Incident Team Who WebinarDocument14 pagesDR Lara Vojnov Severe Acute Hepatitis of Unknown Aetiology WHO Incident Team Who Webinariq_dianaNo ratings yet
- 22 02 02 WHO EUL - PHLabs US Final - DR Ute FinalDocument10 pages22 02 02 WHO EUL - PHLabs US Final - DR Ute Finaliq_dianaNo ratings yet
- Anoverviewoftheantimicrobialmechanismsofbacteria AIMS PublishedDocument21 pagesAnoverviewoftheantimicrobialmechanismsofbacteria AIMS Publishediq_dianaNo ratings yet
- Hepatitis B Facts Testing and VaccinationDocument2 pagesHepatitis B Facts Testing and Vaccinationiq_dianaNo ratings yet
- BiochemMed2019 01Document6 pagesBiochemMed2019 01iq_dianaNo ratings yet
- 033240Document3 pages033240Josh AshNo ratings yet
- DR Jilian WHO Webinar Covid Self Testing GuideDocument10 pagesDR Jilian WHO Webinar Covid Self Testing Guideiq_dianaNo ratings yet
- Dr. Weny Rinawati - Important and Novel Biomarker For HepatitisDocument24 pagesDr. Weny Rinawati - Important and Novel Biomarker For Hepatitisiq_dianaNo ratings yet
- COVID-19 Back Tie Don Doff ChecklistDocument2 pagesCOVID-19 Back Tie Don Doff Checklistiq_dianaNo ratings yet
- Impacts of Extracurricular Activities On The Academic Performance of Student AthletesDocument3 pagesImpacts of Extracurricular Activities On The Academic Performance of Student AthletesKarlo VillanuevaNo ratings yet
- Brunswick Manual Preinstalacion GSXDocument33 pagesBrunswick Manual Preinstalacion GSXroberto dominguezNo ratings yet
- The DAMA Guide To The Data Management Body of Knowledge - First EditionDocument430 pagesThe DAMA Guide To The Data Management Body of Knowledge - First Editionkakarotodesu100% (10)
- QBM101Document37 pagesQBM101Shang BinNo ratings yet
- Make - Volume 13 - Volume 13Document212 pagesMake - Volume 13 - Volume 13Pedernal Lisiao100% (2)
- IBEF Cement-February-2023Document26 pagesIBEF Cement-February-2023Gurnam SinghNo ratings yet
- Intro To StarsDocument37 pagesIntro To StarsENo ratings yet
- 1250kva DG SetDocument61 pages1250kva DG SetAnagha Deb100% (1)
- CREDEDocument10 pagesCREDEDaffodilsNo ratings yet
- Armenotech PCIDSS AOCDocument13 pagesArmenotech PCIDSS AOCHakob ArakelyanNo ratings yet
- REACH ArticlesDocument12 pagesREACH ArticlesChristian SugasttiNo ratings yet
- 978-0393617542 Research MethodsDocument18 pages978-0393617542 Research MethodsReccebacaNo ratings yet
- Test Bank For Organizations Behavior Structure Processes 14th Edition James GibsonDocument36 pagesTest Bank For Organizations Behavior Structure Processes 14th Edition James Gibsonfurrygrindlett3t1bt100% (37)
- Papaer JournelDocument6 pagesPapaer JournelsonalisabirNo ratings yet
- Uber+PM+Prioritisation+Assignment+Submission+File-Shashank KaranthDocument6 pagesUber+PM+Prioritisation+Assignment+Submission+File-Shashank KaranthShashank KaranthNo ratings yet
- EKOFLUID PRODUCT SHEET FILOIL 6000 210x297 EN WEBDocument4 pagesEKOFLUID PRODUCT SHEET FILOIL 6000 210x297 EN WEBjunaidi.036No ratings yet
- Activity 1.1.2 Simple Machine Practice Problems KeyDocument6 pagesActivity 1.1.2 Simple Machine Practice Problems KeyNehemiah GriffinNo ratings yet
- Assignment 1 To 7Document23 pagesAssignment 1 To 7KashishNo ratings yet
- SIP Debugging Commands Overview - Cisco CommunityDocument5 pagesSIP Debugging Commands Overview - Cisco CommunitysenthilNo ratings yet
- h4 History of India Ad 1526 - Ad 1707Document2 pagesh4 History of India Ad 1526 - Ad 1707Baddela ReddyNo ratings yet
- 02 Geotechnical Investigation (General)Document35 pages02 Geotechnical Investigation (General)Miftahul JannaNo ratings yet
- Eating Well: Snacks For 1-4 Year OldsDocument42 pagesEating Well: Snacks For 1-4 Year OldsAndreea AndreiNo ratings yet
- Alternative Refrigerants Manny A PresentationDocument29 pagesAlternative Refrigerants Manny A PresentationEmmanuel Zr Dela CruzNo ratings yet
- Inspection and Test Plan (ITP) For Spherical Storage Tanks: Dehloran Olefin PlantDocument9 pagesInspection and Test Plan (ITP) For Spherical Storage Tanks: Dehloran Olefin PlantbahmanNo ratings yet
- Tutorial 2 EtherchannelDocument3 pagesTutorial 2 EtherchannelOng CHNo ratings yet
- HRM ModelDocument6 pagesHRM ModelsakshiNo ratings yet
- Data Science BooksDocument11 pagesData Science BooksAnalytics Insight100% (1)
- Safelisting in Office 365Document5 pagesSafelisting in Office 365Brett ThomasNo ratings yet
- Dunhill The Old WindmillDocument2 pagesDunhill The Old WindmillMaría Hernández MiraveteNo ratings yet
- Leave Management System: Software Requirements Specification DocumentDocument6 pagesLeave Management System: Software Requirements Specification Documentk767No ratings yet
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (403)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsRating: 5 out of 5 stars5/5 (1)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeNo ratings yet
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (78)
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (20)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisFrom EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisRating: 4.5 out of 5 stars4.5/5 (42)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsFrom EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo ratings yet
- Gut: the new and revised Sunday Times bestsellerFrom EverandGut: the new and revised Sunday Times bestsellerRating: 4 out of 5 stars4/5 (392)
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 4 out of 5 stars4/5 (5)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaFrom EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaRating: 4.5 out of 5 stars4.5/5 (266)
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 4 out of 5 stars4/5 (3)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.From EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Rating: 4.5 out of 5 stars4.5/5 (110)
- 12 Rules for Life by Jordan B. Peterson - Book Summary: An Antidote to ChaosFrom Everand12 Rules for Life by Jordan B. Peterson - Book Summary: An Antidote to ChaosRating: 4.5 out of 5 stars4.5/5 (207)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeFrom EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeRating: 4.5 out of 5 stars4.5/5 (253)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsFrom EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsRating: 4.5 out of 5 stars4.5/5 (169)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 3.5 out of 5 stars3.5/5 (3)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisFrom EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (1)
- Algorithms to Live By: The Computer Science of Human DecisionsFrom EverandAlgorithms to Live By: The Computer Science of Human DecisionsRating: 4.5 out of 5 stars4.5/5 (722)
- Sleep Stories for Adults: Overcome Insomnia and Find a Peaceful AwakeningFrom EverandSleep Stories for Adults: Overcome Insomnia and Find a Peaceful AwakeningRating: 4 out of 5 stars4/5 (3)
- When the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisFrom EverandWhen the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisRating: 3.5 out of 5 stars3.5/5 (2)
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDFrom EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDRating: 5 out of 5 stars5/5 (1)
- The Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsFrom EverandThe Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsNo ratings yet
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessFrom EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessRating: 4.5 out of 5 stars4.5/5 (328)